Rosacea
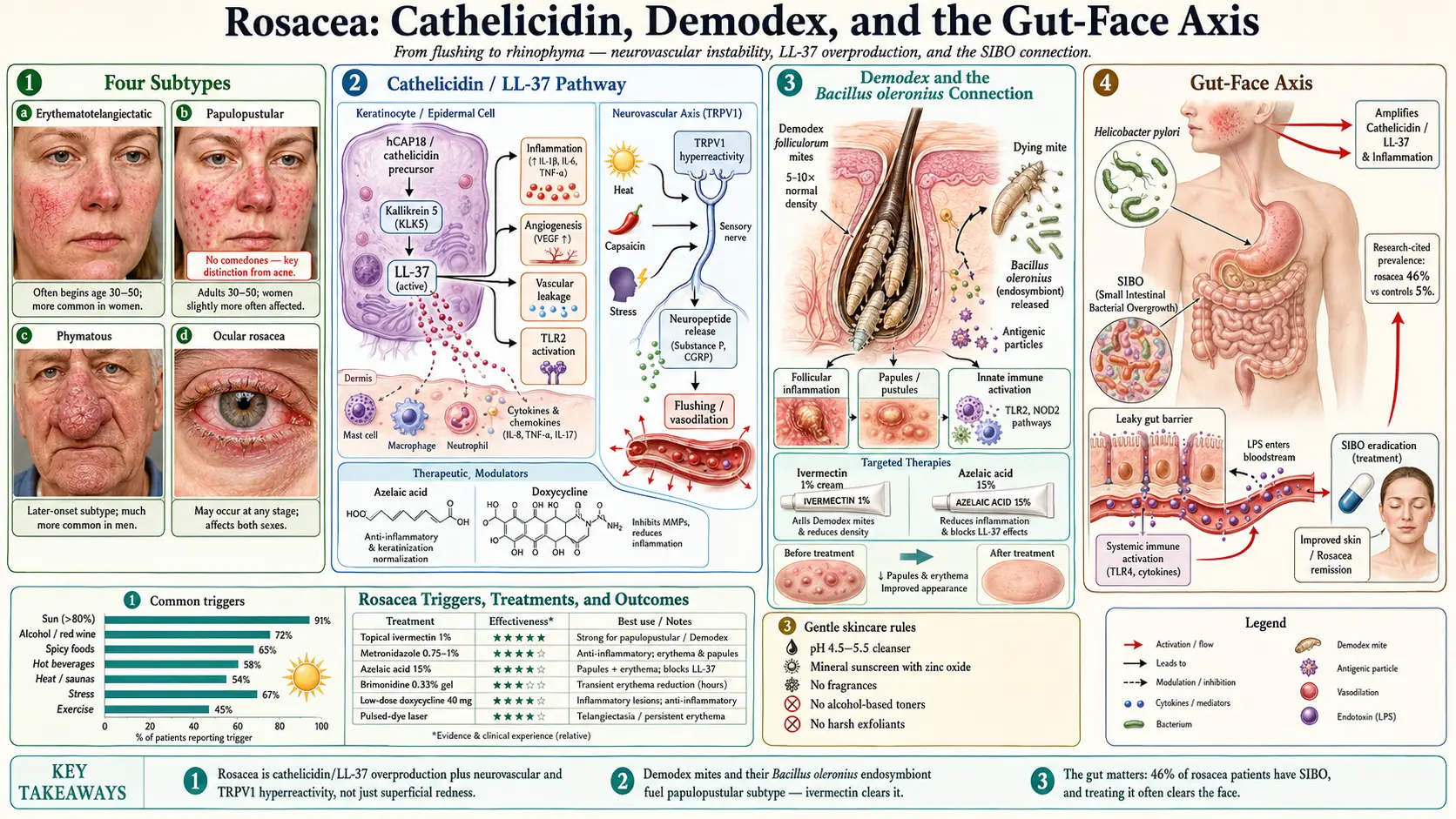
Table of Contents
- What Is Rosacea?
- Subtypes of Rosacea
- Who Gets Rosacea?
- Causes and Theories
- Common Triggers
- Conventional Treatments
- Natural and Naturopathic Approaches
- SIBO Treatment Protocol
- Gut Healing for Rosacea
- Anti-Inflammatory Diet
- Gentle Skincare for Rosacea
- Cautions and Considerations
- References & Research
- Featured Videos
What Is Rosacea?
Rosacea is a chronic inflammatory skin condition that primarily affects the central face — the cheeks, nose, chin, and forehead. It is characterized by persistent redness, visible blood vessels, and in some cases, acne-like bumps and skin thickening. Rosacea affects an estimated 16 million Americans and over 415 million people worldwide.
From a naturopathic perspective, rosacea is far more than a surface-level skin condition. It is a systemic inflammatory disorder with deep connections to the gut, immune system, and vascular health. While conventional treatment focuses primarily on symptom suppression, naturopathic medicine seeks to identify and address the underlying drivers of inflammation, immune dysregulation, and microbial imbalance that fuel this condition.
Rosacea typically begins after age 30 and follows a progressive course if left unaddressed. Early signs include a tendency to flush or blush easily, followed by persistent redness that does not resolve. Over time, visible blood vessels, papules, pustules, and in some cases, tissue overgrowth may develop.
Subtypes of Rosacea
Rosacea is classified into four main subtypes, though many patients exhibit features of more than one subtype simultaneously.
1. Erythematotelangiectatic Rosacea (ETR)
This is the most common subtype and is characterized by:
- Persistent central facial redness (erythema) that may resemble a sunburn
- Visible blood vessels (telangiectasia), particularly on the cheeks and nose
- Frequent flushing and blushing in response to triggers
- Skin sensitivity, stinging, and burning sensations
- Dryness and rough texture in the affected areas
ETR reflects underlying vascular instability and heightened neurovascular reactivity. The blood vessels in rosacea-affected skin are abnormally responsive to stimuli that would not cause visible flushing in unaffected individuals.
2. Papulopustular Rosacea
Often mistaken for acne, this subtype involves:
- Red, inflamed papules (bumps without pus) and pustules (bumps with pus)
- Persistent background redness
- Central facial distribution — differs from acne, which commonly involves the forehead, jawline, and back
- Absence of comedones (blackheads and whiteheads) — a key distinction from acne vulgaris
This subtype involves a stronger immune and inflammatory component, with elevated levels of cathelicidin antimicrobial peptides and matrix metalloproteinases in the skin.
3. Phymatous Rosacea
The least common but most disfiguring subtype, characterized by:
- Thickening and enlargement of the skin, most commonly on the nose (rhinophyma)
- Irregular skin surface with enlarged pores and nodular bumps
- Fibrous tissue overgrowth driven by chronic inflammation
- More common in men than women
Rhinophyma, the bulbous enlargement of the nose, was historically and incorrectly attributed to excessive alcohol consumption. While alcohol can worsen rosacea, rhinophyma is a result of chronic rosacea-driven tissue remodeling.
4. Ocular Rosacea
This subtype affects the eyes and can occur independently of skin symptoms:
- Red, irritated, dry eyes
- Burning, stinging, and gritty sensation in the eyes
- Swollen eyelids (blepharitis)
- Recurrent styes and chalazia
- Sensitivity to light (photophobia)
- In severe cases, corneal damage and vision impairment
Ocular rosacea is frequently underdiagnosed. Up to 50% of rosacea patients may have some degree of eye involvement. An ophthalmology referral is important when ocular symptoms are present.
Who Gets Rosacea?
While rosacea can affect anyone, certain populations are at higher risk:
- Fair-skinned individuals of Northern European descent (Celtic, Scandinavian, and English backgrounds) are most commonly affected, though rosacea occurs in all skin types and ethnicities and is likely underdiagnosed in darker skin tones
- Age 30-60 — Rosacea most commonly appears in the third to sixth decades of life
- Women are diagnosed more frequently than men, though men tend to develop more severe forms, including rhinophyma
- Family history — A genetic predisposition is common, with many patients reporting affected family members
- History of easy flushing or blushing in earlier years
Causes and Theories
The exact cause of rosacea remains incompletely understood, but research has identified several interconnected factors that contribute to the disease.
Demodex Mites
Demodex folliculorum and Demodex brevis are microscopic mites that live in human hair follicles and sebaceous glands. While present on most healthy adults, rosacea patients harbor significantly higher densities of Demodex — often 5 to 10 times more than unaffected skin. The mites contribute to rosacea through several mechanisms:
- Physical blockage and damage to follicles
- Release of bacterial antigens from the bacterium Bacillus oleronius, which lives inside Demodex and triggers an immune response upon mite death
- Stimulation of toll-like receptor 2 (TLR2) in the skin, amplifying inflammation
Cathelicidin and LL-37
Cathelicidin is an antimicrobial peptide produced by the innate immune system. In rosacea, there is an overproduction of cathelicidin and its active fragment LL-37. The enzyme kallikrein 5 (KLK5) cleaves cathelicidin into LL-37 at abnormally high levels in rosacea skin. LL-37 is a potent promoter of:
- Inflammation and immune cell recruitment
- Angiogenesis (new blood vessel formation), contributing to telangiectasia
- Vascular leakage and edema
This cathelicidin dysregulation is considered one of the central pathological mechanisms in rosacea.
Vascular Dysfunction
Rosacea involves abnormalities in the blood vessels and nerves of the facial skin:
- Increased density of blood vessels in rosacea-affected skin
- Heightened neurovascular reactivity — blood vessels dilate excessively in response to stimuli
- Transient receptor potential (TRP) channel dysfunction — These ion channels in sensory nerves respond to temperature, capsaicin, and other stimuli. In rosacea, they are abnormally sensitive, leading to flushing, burning, and stinging.
- Impaired vasoconstriction — Once dilated, vessels are slow to constrict, leading to persistent redness
The Gut Connection
The gut-rosacea connection is one of the most compelling areas of emerging research:
H. pylori — Helicobacter pylori infection has been found to be significantly more prevalent in rosacea patients. H. pylori produces a protein called RhoA-activating toxin that increases the production of reactive oxygen species and nitric oxide, promoting vascular dilation. Some studies have shown rosacea improvement or remission following successful H. pylori eradication.
SIBO (Small Intestinal Bacterial Overgrowth) — A landmark study found that SIBO was present in approximately 46% of rosacea patients compared to 5% of controls. Remarkably, successful SIBO treatment led to complete rosacea remission in the majority of affected patients and significant improvement in most others. The proposed mechanism involves bacterial endotoxins entering the bloodstream through a compromised gut lining and triggering the inflammatory cascade that manifests as rosacea.
Common Triggers
Rosacea flares are often provoked by identifiable triggers. Keeping a trigger diary is one of the most practical strategies for managing rosacea. Common triggers include:
Environmental Triggers
- Sun exposure — The most commonly reported trigger, cited by over 80% of rosacea patients. UV radiation increases inflammation, cathelicidin production, and vascular damage.
- Heat — Hot weather, saunas, hot baths, and heated indoor environments can trigger flushing
- Cold and wind — Harsh weather can damage the skin barrier and provoke flares
Dietary Triggers
- Alcohol — Particularly red wine, which contains histamine and sulfites. Alcohol causes vasodilation and triggers flushing through multiple mechanisms.
- Spicy foods — Capsaicin activates TRPV1 receptors in the skin, directly triggering flushing and inflammation
- Hot beverages — The temperature of the beverage, rather than its content, is the primary trigger. Allowing drinks to cool slightly can help.
- Histamine-rich foods — Aged cheeses, fermented foods, cured meats, and certain fruits can trigger flares in sensitive individuals
Lifestyle Triggers
- Emotional stress — Activates the sympathetic nervous system and HPA axis, leading to flushing and inflammation
- Vigorous exercise — Can provoke flushing, though regular moderate exercise is beneficial overall
- Certain medications — Vasodilators, some blood pressure medications, and topical steroids (which cause steroid rosacea with prolonged use)
- Irritating skincare products — Alcohol-based products, fragrances, astringents, and harsh exfoliants
Conventional Treatments
Topical Medications
- Metronidazole (0.75-1%) — An antibiotic and anti-inflammatory agent that is a first-line topical treatment. It reduces papules, pustules, and redness. Available as gel, cream, or lotion.
- Azelaic acid (15%) — Reduces inflammation, normalizes keratinization, and has mild antimicrobial effects. Particularly effective for papulopustular rosacea and post-inflammatory hyperpigmentation. Also used in naturopathic practice as it is a naturally occurring dicarboxylic acid.
- Ivermectin (1% cream) — An anti-parasitic agent highly effective against Demodex mites. Studies show it may be more effective than metronidazole for papulopustular rosacea. Applied once daily.
- Brimonidine (0.33% gel) — An alpha-2 adrenergic agonist that constricts blood vessels, temporarily reducing redness. Effects last 8-12 hours. Some patients experience rebound redness upon discontinuation.
Oral Medications
- Low-dose doxycycline (40 mg modified-release) — At sub-antimicrobial doses, doxycycline acts as an anti-inflammatory by inhibiting matrix metalloproteinases (MMPs) and does not contribute to antibiotic resistance
- Oral antibiotics — Higher-dose doxycycline or minocycline for more severe papulopustular rosacea
- Oral isotretinoin — Reserved for severe, treatment-resistant rosacea
Laser and Light Therapy
- Pulsed dye laser (PDL) — Targets hemoglobin in blood vessels, reducing telangiectasia and persistent redness
- Intense pulsed light (IPL) — Broad-spectrum light that reduces redness and visible vessels
- CO2 laser — Used for tissue remodeling in phymatous rosacea
Natural and Naturopathic Approaches
A naturopathic approach to rosacea addresses the underlying inflammation, immune dysregulation, microbial imbalance, and gut dysfunction that drive the condition.
Azelaic Acid
Azelaic acid occupies a unique position as both a conventional and natural treatment. It is a naturally occurring dicarboxylic acid found in grains such as wheat, rye, and barley. At concentrations of 10-20%, it reduces inflammation, kills Demodex-associated bacteria, and normalizes keratinocyte proliferation. It is well-tolerated and safe for long-term use.
MSM (Methylsulfonylmethane)
MSM is an organic sulfur compound with anti-inflammatory and antioxidant properties. Both oral supplementation (1-3 g daily) and topical application have shown benefit in rosacea. MSM helps reduce redness, hydrate the skin, and support the structural integrity of blood vessels. A topical cream containing MSM and silymarin (from milk thistle) has been studied with positive results for rosacea.
Omega-3 Fatty Acids
EPA and DHA are potent anti-inflammatory agents that help resolve the chronic inflammation underlying rosacea. They reduce pro-inflammatory eicosanoids, support vascular health, and may help with ocular rosacea symptoms. A dose of 2,000-3,000 mg combined EPA/DHA daily from fish oil or algal sources is recommended.
Probiotics
Given the strong gut-rosacea connection, probiotics are a foundational part of the naturopathic approach. Specific strains that have shown benefit include Lactobacillus rhamnosus, Lactobacillus plantarum, and Saccharomyces boulardii. Probiotics help restore gut barrier integrity, reduce endotoxemia, modulate the immune response, and may help address underlying SIBO and dysbiosis.
Zinc
Zinc supports immune function, wound healing, and has anti-inflammatory properties. Low zinc status has been associated with rosacea. Zinc supplementation at 25-30 mg daily (as zinc picolinate or bisglycinate) may help reduce papules and pustules. Topical zinc preparations can also soothe irritated skin.
B Vitamins
Riboflavin (B2) and niacinamide (B3) are particularly relevant for rosacea. Niacinamide at 500-750 mg daily or applied topically (4-5%) improves skin barrier function, reduces transepidermal water loss, decreases redness, and has anti-inflammatory effects. Note that niacin (nicotinic acid) should be avoided as it can trigger flushing, while niacinamide does not.
Aloe Vera
Aloe vera gel applied topically provides cooling, anti-inflammatory, and hydrating benefits. It contains compounds that inhibit cyclooxygenase and reduce prostaglandin production. For rosacea, use pure aloe vera gel (without added fragrances or alcohol) as a soothing agent and moisturizer.
Green Tea
Green tea polyphenols, particularly EGCG, have significant anti-inflammatory, antioxidant, and anti-angiogenic properties. A topical cream containing green tea extract has been shown to reduce pustule count and redness in rosacea. Oral consumption of 3-4 cups daily provides systemic anti-inflammatory benefits. Green tea also inhibits the activity of MMP-2 and MMP-9, enzymes involved in rosacea-related tissue damage.
Licorice Root Extract (Topical)
Licorice root (Glycyrrhiza glabra) contains glycyrrhizin and licochalcone A, compounds with potent anti-inflammatory and anti-redness properties. Topical preparations containing licorice extract have been shown to reduce erythema, irritation, and itching. Licochalcone A specifically inhibits NF-kB signaling and reduces pro-inflammatory cytokine production in the skin.
Niacinamide (Topical)
Topical niacinamide at 4-5% concentration is one of the most versatile and well-tolerated ingredients for rosacea-prone skin. Benefits include strengthened skin barrier, reduced sensitivity, decreased redness, improved hydration, and anti-inflammatory effects. It can be used in combination with other topical treatments and is safe for long-term daily use.
SIBO Treatment Protocol
Given the strong association between SIBO and rosacea, testing for and treating SIBO is an important component of the naturopathic approach.
Testing
A lactulose or glucose breath test measures hydrogen and methane gases produced by bacteria in the small intestine. Elevated levels indicate bacterial overgrowth. Newer tests also measure hydrogen sulfide, a third gas now recognized as a SIBO subtype.
Herbal Antimicrobial Protocol
Herbal antimicrobials have been shown to be as effective as the antibiotic rifaximin for SIBO eradication. A typical protocol includes a combination of the following, taken for 4-6 weeks:
- Berberine (from goldenseal, Oregon grape, or barberry) — 500 mg 2-3 times daily
- Oregano oil (standardized to carvacrol) — 200 mg 2-3 times daily
- Neem — 300 mg 2-3 times daily
- Allicin (from garlic) — particularly effective for methane-dominant SIBO — 450 mg 2-3 times daily
Prokinetics
After SIBO treatment, prokinetic agents are essential to prevent relapse by supporting the migrating motor complex (MMC), the cleansing wave that sweeps bacteria from the small intestine between meals:
- Ginger (Iberogast or ginger root extract) — stimulates gastric motility
- 5-HTP — supports serotonin production, which regulates gut motility
- Meal spacing — Allow 4-5 hours between meals to allow the MMC to function
Gut Healing for Rosacea
Beyond SIBO treatment, comprehensive gut healing is often necessary for lasting rosacea improvement.
Remove
Identify and remove factors that damage the gut: food sensitivities (common culprits include gluten, dairy, and eggs), excess alcohol, NSAIDs, and unnecessary antibiotics. Consider testing for H. pylori and treating if positive.
Replace
Support adequate digestive function with digestive enzymes if needed, and ensure sufficient stomach acid production. Low stomach acid (hypochlorhydria) contributes to SIBO by failing to sterilize incoming bacteria. Betaine HCl with pepsin may be appropriate for some patients.
Reinoculate
Restore a healthy microbiome with probiotics (as discussed above) and prebiotic foods such as garlic, onions, asparagus, and artichokes. Start slowly with prebiotics, as they may initially worsen symptoms in SIBO patients.
Repair
Support gut lining repair with nutrients including:
- L-glutamine — 3-5 g daily, the primary fuel source for intestinal cells
- Zinc carnosine — Supports mucosal healing and reduces intestinal inflammation
- Deglycyrrhizinated licorice (DGL) — Promotes mucus production and soothes the gut lining
- Collagen or bone broth — Provides amino acids (glycine, proline) that support gut lining integrity
- Aloe vera juice — Soothes inflammation and supports mucosal healing
Anti-Inflammatory Diet
Dietary modification is a powerful tool in rosacea management. An anti-inflammatory diet reduces systemic inflammation, supports gut health, and minimizes dietary triggers.
Foods to Emphasize
- Cold-water fatty fish (wild salmon, sardines, mackerel) — Rich in anti-inflammatory omega-3 fatty acids
- Colorful vegetables and fruits — Provide antioxidants and polyphenols that combat inflammation
- Leafy greens — High in folate, magnesium, and anti-inflammatory compounds
- Turmeric and ginger — Potent anti-inflammatory spices
- Olive oil — Contains oleocanthal, a natural anti-inflammatory compound
- Green tea — Anti-inflammatory and antioxidant
- Fiber-rich foods — Support healthy microbiome diversity and bowel regularity
Foods to Minimize or Avoid
- Alcohol, particularly red wine and spirits
- Spicy foods containing capsaicin
- Histamine-rich foods (aged cheeses, cured meats, fermented foods, vinegar) if histamine intolerance is suspected
- Refined sugar and processed foods — Promote inflammation and insulin resistance
- Dairy — May be inflammatory for some individuals
- Gluten — Consider a trial elimination if gut symptoms are present
- Trans fats and excessive omega-6 fatty acids from processed vegetable oils
Gentle Skincare for Rosacea
Rosacea-affected skin has a compromised barrier and heightened sensitivity. A minimalist, gentle skincare approach is essential.
Cleansing
- Use a fragrance-free, soap-free, pH-balanced cleanser (pH 4.5-5.5)
- Cleanse with lukewarm water — never hot water
- Pat dry gently with a soft towel; never rub
- Avoid foaming cleansers, scrubs, and any product containing alcohol, menthol, camphor, or sodium lauryl sulfate
Moisturizing
- Apply a fragrance-free, hypoallergenic moisturizer daily
- Look for barrier-repairing ingredients: ceramides, hyaluronic acid, niacinamide, and squalane
- Apply moisturizer while skin is slightly damp to lock in hydration
Sun Protection
- Use a mineral sunscreen (zinc oxide and/or titanium dioxide) with SPF 30 or higher daily
- Mineral sunscreens are better tolerated than chemical sunscreens by rosacea-prone skin
- Tinted mineral sunscreens can help camouflage redness while providing protection
- Wear a wide-brimmed hat for additional protection
Ingredients to Avoid
- Alcohol (ethanol, denatured alcohol, isopropyl alcohol)
- Fragrances and essential oils (with the exception of carefully diluted, anti-inflammatory options like chamomile)
- Menthol, camphor, and peppermint
- Witch hazel (contains irritating tannins)
- Strong chemical exfoliants (high-percentage glycolic acid, salicylic acid)
- Retinoids (unless introduced very gradually and at low concentrations under professional guidance)
Cautions and Considerations
- Topical steroids should never be used on rosacea. While they may temporarily reduce redness, they cause rebound flaring and can lead to steroid rosacea, a difficult-to-treat condition that develops after prolonged topical steroid use on the face.
- Ocular rosacea requires evaluation by an ophthalmologist, especially if there is any change in vision or significant eye pain.
- Rhinophyma in advanced stages may require surgical intervention (laser or excision). Early treatment of rosacea helps prevent progression to this stage.
- SIBO testing and treatment should be supervised by a knowledgeable practitioner. Self-treatment with antimicrobials can be counterproductive if not properly guided.
- Herbal antimicrobials such as berberine and oregano oil should not be used long-term without professional supervision. They can affect liver enzymes and may interact with medications.
- Histamine intolerance may coexist with rosacea and can be assessed through a structured elimination diet and, in some cases, DAO enzyme testing.
- Patience is essential — Rosacea responds gradually to treatment. Most naturopathic protocols require 2-3 months to show significant improvement, and long-term management is often necessary.
- Psychological impact — Rosacea can significantly affect quality of life and self-esteem. Emotional support and stress management are important components of comprehensive care.
13. References & Research
Historical Background
Rosacea was first described in the 14th century by the French surgeon Guy de Chauliac, who called it "goutterose" (French for "pink droplet"). The English dermatologist Thomas Bateman provided the first detailed clinical description in 1812. The modern classification into four subtypes was established by the National Rosacea Society Expert Committee in 2002, led by Jonathan Wilkin. The discovery of elevated cathelicidin LL-37 in rosacea skin by Richard Gallo and colleagues in 2007 was a landmark finding that reshaped understanding of the disease's pathophysiology.
Key Research Papers
- Two AM, Wu W, Gallo RL, Hata TR. Rosacea: part I. Introduction, categorization, histology, pathogenesis, and risk factors. J Am Acad Dermatol. 2015;72(5):749-758.
- Two AM, Wu W, Gallo RL, Hata TR. Rosacea: part II. Topical and systemic therapies in the treatment of rosacea. J Am Acad Dermatol. 2015;72(5):761-770.
- Yamasaki K, Di Nardo A, Bardan A, et al. Increased serine protease activity and cathelicidin promotes skin inflammation in rosacea. Nat Med. 2007;13(8):975-980.
- Stein Gold L, Kircik L, Fowler J, et al. Efficacy and safety of ivermectin 1% cream in treatment of papulopustular rosacea: results of two randomized, double-blind, vehicle-controlled pivotal studies. J Drugs Dermatol. 2014;13(3):316-323.
- Parodi A, Paolino S, Greco A, et al. Small intestinal bacterial overgrowth in rosacea: clinical effectiveness of its eradication. Clin Gastroenterol Hepatol. 2008;6(7):759-764.
- Wilkin J, Dahl M, Detmar M, et al. Standard classification of rosacea: report of the National Rosacea Society Expert Committee on the classification and staging of rosacea. J Am Acad Dermatol. 2002;46(4):584-587.
- Tan J, Berg M. Rosacea: current state of epidemiology. J Am Acad Dermatol. 2013;69(6 Suppl 1):S27-S35.
- Del Rosso JQ, Thiboutot D, Gallo RL, et al. Consensus recommendations from the American Acne and Rosacea Society on the management of rosacea. Cutis. 2014;93(3):134-138.
- Forton FMN, De Maertelaer V. Two consecutive standardized skin surface biopsies: an improved sampling method to evaluate Demodex density as a diagnostic tool for rosacea. Acta Derm Venereol. 2017;97(2):242-248.
- Egeberg A, Hansen PR, Gislason GH, Thyssen JP. Clustering of autoimmune diseases in patients with rosacea. J Am Acad Dermatol. 2016;74(4):667-672.
- Schwab VD, Sulk M, Seeliger S, et al. Neurovascular and neuroimmune aspects in the pathophysiology of rosacea. J Investig Dermatol Symp Proc. 2011;15(1):53-62.
- Mikkelsen CS, Holmgren HR, Kjellman P, et al. Rosacea: a clinical review. Dermatol Reports. 2016;8(1):6387.
Research Papers
Curated PubMed topic searches of peer-reviewed literature on Rosacea. Each link opens a live PubMed query so you always see the most current studies.
- PubMed: Rosacea pathogenesis
- PubMed: Ivermectin and Demodex
- PubMed: Topical brimonidine
- PubMed: Low-dose doxycycline
- PubMed: IPL and laser therapy
- PubMed: Rosacea and SIBO
- PubMed: H. pylori and rosacea
- PubMed: Dietary triggers
- PubMed: Ocular rosacea
- PubMed: Azelaic acid therapy
- PubMed: Rhinophyma treatment
- PubMed: Cathelicidin and inflammation
Connections
- Melasma
- Acne
- Zinc
- SIBO
- Gut Healing
- Green Tea
- Elimination Diet
- Eczema
- Psoriasis
- Peptic Ulcer Disease
- Gut-Brain Axis
- Probiotics
- Licorice
- Anti-Inflammatory Diet
- Ginger
- Turmeric
- Fermented Foods
- Omega-3 Fatty Acids
- Neem
- Dry Eye Disease