Hashimoto's Thyroiditis: The Most Common Cause of Hypothyroidism in the Developed World
Deep-Dive Articles
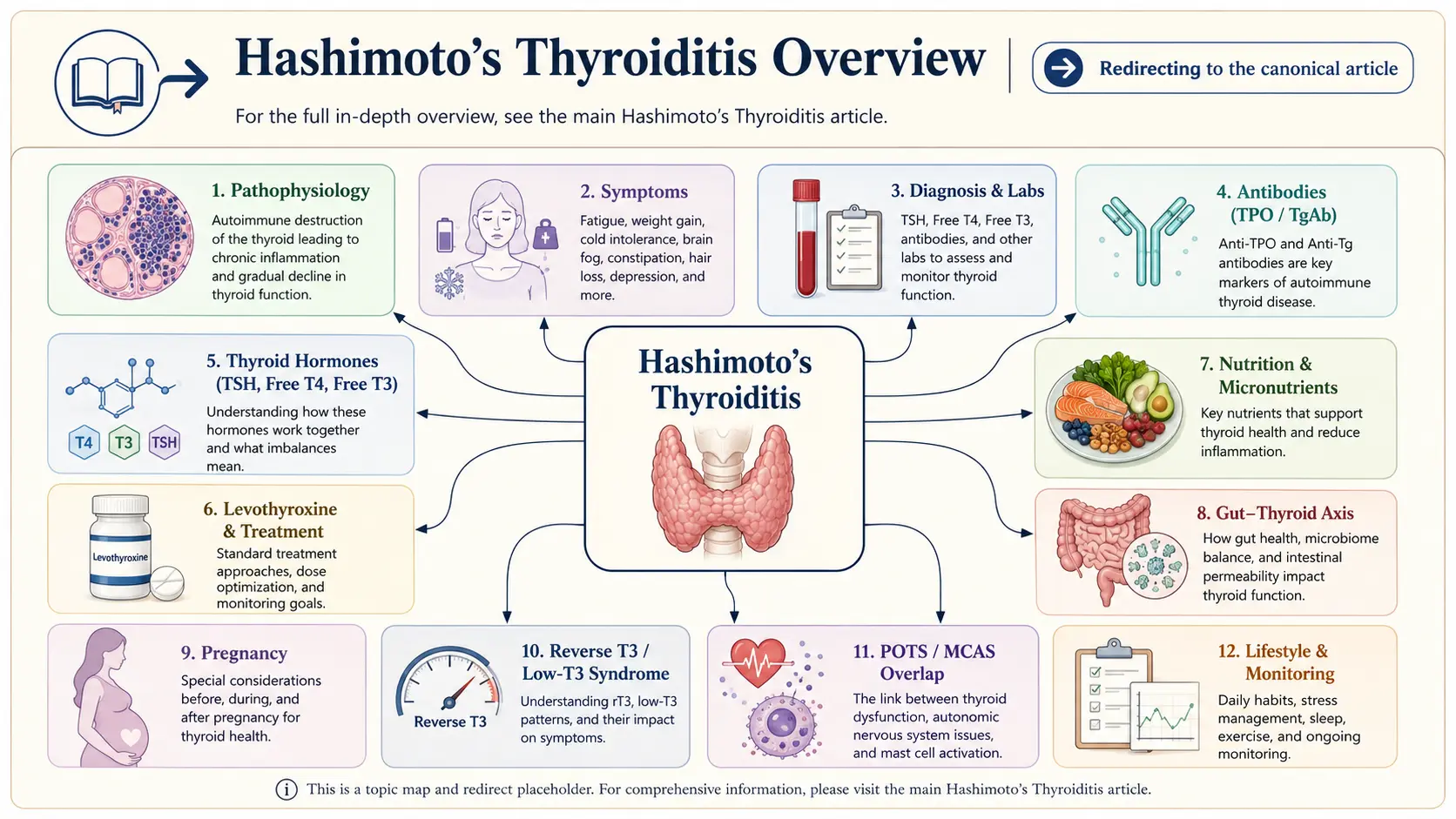
Hashimoto’s is almost never just “take your Synthroid and move on.” The eight guides below tackle the pieces your endocrinologist may never explain — what TPO and TgAb antibodies actually mean, why the “normal” TSH range hides so many undertreated patients, the levothyroxine-vs-NDT-vs-T3 debate, the AIP diet and gluten connection, mineral cofactors for conversion, reverse T3 and low-T3 syndrome, pregnancy dose changes, and the Hashimoto’s / POTS / MCAS overlap. Start wherever you are.
TPO & TgAb Antibodies Explained
What anti-thyroid peroxidase and anti-thyroglobulin antibodies actually measure, what a “positive with normal TSH” result means, why antibody levels rise and fall, and the evidence on bringing them down.
TSH / T4 / T3 Optimal Ranges
The lab “normal” range is 0.5–4.5 — the optimal range is narrower. How to read a full thyroid panel (TSH, free T4, free T3, reverse T3, TPO, TgAb), and the case for treating to free T4 and free T3 targets, not just TSH.
Levothyroxine vs NDT vs T3
Synthroid / Levoxyl / Tirosint vs. natural desiccated thyroid (Armour, NP Thyroid, WP Thyroid) vs. combination T4+T3 (Cytomel / liothyronine). Why T4-only fails some patients, DIO2 polymorphism, and how to advocate for alternatives.
AIP Diet & Gluten Elimination
The Autoimmune Protocol, the gluten-thyroid molecular-mimicry evidence, Hakaru Hashimoto’s original observation, and the 30- and 90-day trials that shift antibody levels — what the evidence supports and what it doesn’t.
Selenium, Zinc, Iron & Iodine
Selenium 200 mcg/day — the trial evidence for antibody reduction. Zinc for conversion. Iron (ferritin > 70) for symptoms. Iodine — when to supplement, when to strictly avoid, and why Hashimoto’s changes the usual answer.
Reverse T3 & Low-T3 Syndrome
Why some Hashi patients feel awful on “optimized” T4 — conversion failure, stress/cortisol interference, the rT3/fT3 ratio, nonthyroidal illness, and the protocols clinicians use to restore T3.
Pregnancy & Hashimoto’s
The trimester-specific TSH targets (<2.5 first trimester), the 25–30% dose increase starting week 4–8, miscarriage risk with antibodies, and postpartum thyroiditis — the triphasic pattern clinicians miss.
Hashi / POTS / MCAS Overlap
Why Hashimoto’s patients disproportionately have POTS, MCAS, celiac, and endometriosis. The shared autoimmune/dysautonomia/mast-cell wiring, and a workup order that saves years.
Gut-Thyroid Axis & Intestinal Permeability
Leaky gut, SIBO, H. pylori, and how gut health drives thyroid autoimmunity.
Hashimoto’s thyroiditis (also called Hashimoto’s disease or chronic autoimmune thyroiditis) is an autoimmune condition in which the immune system attacks the thyroid gland, progressively destroying thyroid tissue and impairing hormone production. It is the most common cause of hypothyroidism in iodine-replete populations, affecting roughly 5% of women and 1% of men in the United States. Diagnosis hinges on the combination of thyroid dysfunction and circulating antibodies against thyroid peroxidase (TPO) and/or thyroglobulin.
Table of Contents
- Deep-Dive Articles
- What Hashimoto’s Is
- Symptoms of Thyroid Failure
- Diagnosis — Labs That Matter
- Standard Pharmaceutical Treatment
- Low-Dose Naltrexone and Immune Modulation
- Root-Cause and Functional Approaches
- Pregnancy and Fertility Considerations
- Connections
- Featured Videos
What Hashimoto’s Is
The immune system generates antibodies (anti-TPO, anti-thyroglobulin) and cytotoxic T-cell infiltration that progressively destroy thyroid follicular cells. The gland initially enlarges (goiter), then shrinks over years to decades. Many patients have circulating antibodies for years before clinical hypothyroidism develops. Genetic predisposition is real — HLA-DR3, HLA-DR5, CTLA-4, and PTPN22 variants are associated — but environmental triggers clearly matter, since the condition has become much more common in recent decades.
Symptoms of Thyroid Failure
- Fatigue, particularly mid-afternoon energy crash
- Cold intolerance, perpetually cold hands and feet
- Weight gain, difficulty losing weight
- Dry skin, brittle hair, hair loss including the lateral eyebrow
- Constipation
- Depression, brain fog, slowed thinking
- Puffiness (myxedema), particularly periorbital
- Menstrual irregularities, heavy periods
- Muscle aches, weakness, slow reflex relaxation
- Elevated cholesterol
- Bradycardia
- Hoarseness
Diagnosis — Labs That Matter
- TSH — elevated in overt hypothyroidism. The reference range top (often 4.5 mIU/L) is debated; many functional practitioners target <2.5.
- Free T4, free T3 — complete picture of hormone availability.
- Reverse T3 — sometimes elevated in illness and chronic stress, blocking T3 action.
- Anti-TPO antibodies — positive in roughly 90% of Hashimoto’s.
- Anti-thyroglobulin antibodies — positive in roughly 50%.
- Thyroid ultrasound — characteristic heterogeneous hypoechoic pattern with increased vascularity early, atrophy late.
Standard Pharmaceutical Treatment
- Levothyroxine (T4) — standard first-line. Taken on empty stomach, separate from coffee, calcium, iron, and PPIs by at least 30–60 minutes. Dose titrated to TSH target, typically 0.5–2.5.
- Liothyronine (T3) or combined T4/T3 therapy for patients who remain symptomatic on levothyroxine alone despite normal TSH, particularly those with impaired T4-to-T3 conversion (DIO2 polymorphism).
- Desiccated thyroid extract (NDT, Armour, Nature-Throid) — contains both T4 and T3 in a fixed ratio from porcine thyroid. Popular in integrative practice. Not preferred by endocrinology guidelines but valued by many patients.
Low-Dose Naltrexone and Immune Modulation
Case series and clinical experience suggest low-dose naltrexone (LDN) at 1.5–4.5 mg nightly can reduce TPO antibodies and improve symptoms in some Hashimoto’s patients. Evidence is early and not from large RCTs, but safety is favorable and the intervention is inexpensive.
Root-Cause and Functional Approaches
Triggers and contributors frequently addressed in functional and naturopathic approaches:
- Gluten sensitivity. Celiac disease co-occurs in up to 5% of Hashimoto’s; a trial of gluten elimination is reasonable even without biopsy-confirmed celiac.
- Selenium. 200 µg/day of selenomethionine has reduced TPO antibodies and improved quality of life in several randomized trials.
- Vitamin D. Deficiency is associated with worse disease activity; replete to >40 ng/mL.
- Iron and ferritin. Low ferritin impairs thyroid hormone synthesis and conversion; target ferritin >70 ng/mL.
- Gut health. Intestinal permeability and dysbiosis correlate with antibody levels in some studies.
- Environmental toxins. Halogens (fluoride, bromide), heavy metals, and endocrine disruptors can impair thyroid function.
- Stress and cortisol. Chronic stress impairs T4-to-T3 conversion and worsens symptoms.
- EBV reactivation has been implicated as a trigger in some cases.
- Iodine. Controversial in Hashimoto’s — both deficiency and excess can worsen disease. Avoid high-dose iodine supplementation without clinician guidance.
Pregnancy and Fertility Considerations
Adequate thyroid hormone is essential for fertility, pregnancy, and fetal neurodevelopment. Women with Hashimoto’s attempting conception should target TSH <2.5 mIU/L before pregnancy and in first trimester. Levothyroxine dose typically needs to be increased by 25–30% immediately upon confirming pregnancy, with frequent monitoring thereafter.
Connections
- Levothyroxine vs NDT vs T3
- AIP and Gluten Elimination
- Gut-Thyroid Axis and Intestinal Permeability
- TSH, T4, and T3 Optimal Ranges
- Selenium, Zinc, Iron, and Iodine
- TPO and TgAb Antibodies
- Reverse T3 and Low T3 Syndrome
- Pregnancy and Hashimoto's
- Hashimoto, POTS, and MCAS Overlap
- Selenium
- Iron
- Iodine
- Thyroid Disorders
- Graves' Disease
- Celiac Disease
- POTS
- Vitamin D3
- Hair Loss
- Postpartum Depression
Research Papers
The following PubMed topic searches aggregate the current peer-reviewed literature. Each link opens a live PubMed query — results update as new studies are indexed.
- PubMed — Hashimoto thyroiditis
- PubMed — autoimmune hypothyroidism
- PubMed — anti-TPO antibodies
- PubMed — thyroglobulin antibodies
- PubMed — levothyroxine therapy
- PubMed — subclinical hypothyroidism
- PubMed — selenium Hashimoto
- PubMed — gluten Hashimoto autoimmunity
- PubMed — low dose naltrexone autoimmune
- PubMed — pregnancy hypothyroidism
- PubMed — vitamin D hypothyroidism
- PubMed — thyroid lymphocytic infiltration