Coronary Calcium Score (CAC): The 10-Minute CT Scan That Sees Your Heart Disease Decades Before a Heart Attack

A coronary artery calcium (CAC) score — also called a heart scan, calcium-score CT, or Agatston score — is a specialized, non-contrast CT scan of the chest that quantifies the calcified plaque in the coronary arteries. It takes about 10 minutes, costs roughly $100 to $200 out of pocket in the United States, uses a radiation dose similar to a mammogram, and returns a single number from 0 upward. That number — the Agatston score — is one of the strongest long-range predictors of cardiovascular events available in clinical medicine.
Because calcium in the coronary arteries is visible only after atherosclerotic plaque has been forming for years, a CAC score shows whether your heart disease has already started and how advanced it is. A score of zero in a 55-year-old is one of the most reassuring numbers in medicine; a high score should re-order priorities.
Deep-Dive Articles
The CAC score number is simple; the interpretation is not. The nine articles below break down what the Agatston number actually represents, how the MESA percentile reframes a single result, why a zero score is the strongest negative result in preventive cardiology, when CAC outperforms other cardiac tests (and when it doesn't), how it changes the statin conversation, what it misses (the soft-plaque problem), the cost-and-insurance reality in the US, the special considerations for women and younger adults, and what the evidence says about plaque stabilization and reversal. Start wherever your question lives.
Agatston Score: How the Number Is Calculated
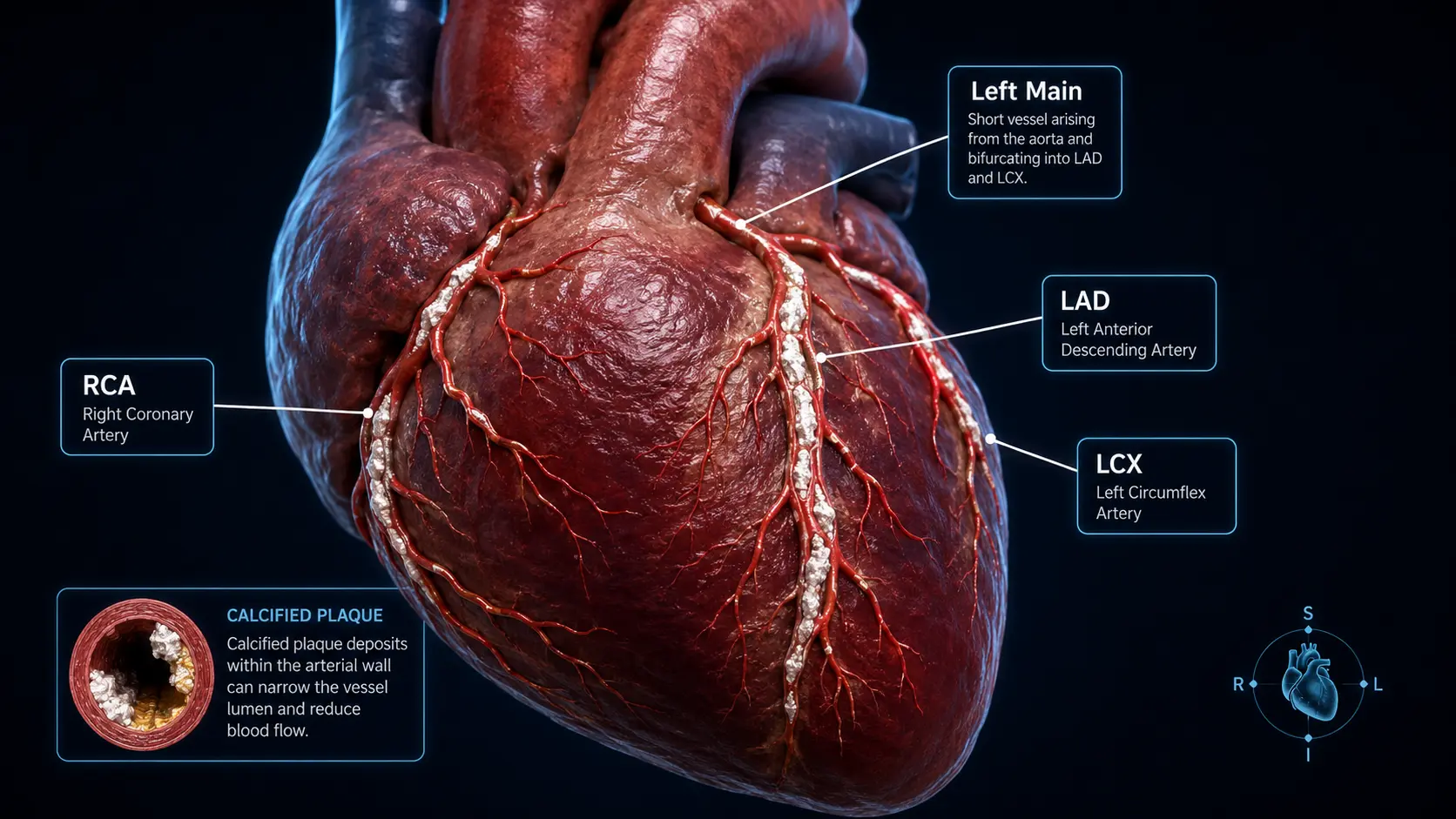
The math behind the score: density factor (1–4), lesion area × density, summed across the LAD, LCX, RCA, and Left Main. Why volume scoring is sometimes preferred, the 130 HU threshold, and the misinterpretations radiologists see most often.
MESA Risk Calculator & Age Percentiles
The Multi-Ethnic Study of Atherosclerosis (MESA) calculator is the standard tool for percentile-based interpretation. Why a CAC of 100 in a 45-year-old is alarming and the same score in a 70-year-old is reassuring. Sex, race, and statin-use modifiers.
CAC = 0: The Strongest "All Clear" in Preventive Cardiology
What a zero score actually rules out (and doesn't), the 5- to 10-year "warranty" concept, when to re-scan, who the rare "zero CAC but heart attack" patients are, and how to use a zero score to avoid years of unnecessary statin debate.
CAC vs CT Angiography vs Stress Test vs ApoB
How CAC compares to coronary CT angiography (CCTA), exercise stress testing, cardiac MRI, EKG, and the lipid markers (ApoB, Lp(a)). When CAC is the right test, when CCTA wins, and when stress testing is still relevant.
CAC, Statins & the Density Paradox
How CAC reshapes statin decisions, the SCOT-HEART and ROBINSCA trial data, the >100 score threshold for statin recommendation regardless of LDL, and the counterintuitive finding that statins increase calcium density (while reducing events).
Soft Plaque & the CAC-Zero False Sense of Security
What CAC cannot see — non-calcified (soft) plaque, vulnerable plaque, the “CAC-zero MI” phenomenon. Why CCTA may be needed for full evaluation in young patients with strong family history or markedly elevated Lp(a).
Insurance, Cost & Access in the US
Typical cash prices ($99–$200), HSA/FSA eligibility, why most insurance still doesn't cover it, hospital vs imaging center pricing, no-prescription scan centers, and the Medicare landscape for higher-risk patients.
CAC in Women & Younger Adults
The 10-year sex offset, why perimenopause is the turning point, premature menopause as a risk amplifier, and the case for CAC testing in women in their late 40s and 50s. Plus when to consider CAC under 40 (familial hypercholesterolemia, elevated Lp(a), early CAD family history).
Can You Reverse Coronary Calcium?
The honest answer: stabilization yes, reversal of calcium volume rarely. The Esselstyn/Ornish/Pritikin trials, exercise data, the difference between event reduction and calcium-volume reduction, and the lifestyle stack that gives the best long-term outcome.
Table of Contents
- Deep-Dive Articles
- What CAC Scoring Measures
- How the Scan Works
- Interpreting Your Score
- Age and Sex Percentiles
- Who Should Consider CAC Testing
- Limits — Soft Plaque Invisibility
- What to Do with Your Result
- Connections
- Featured Videos
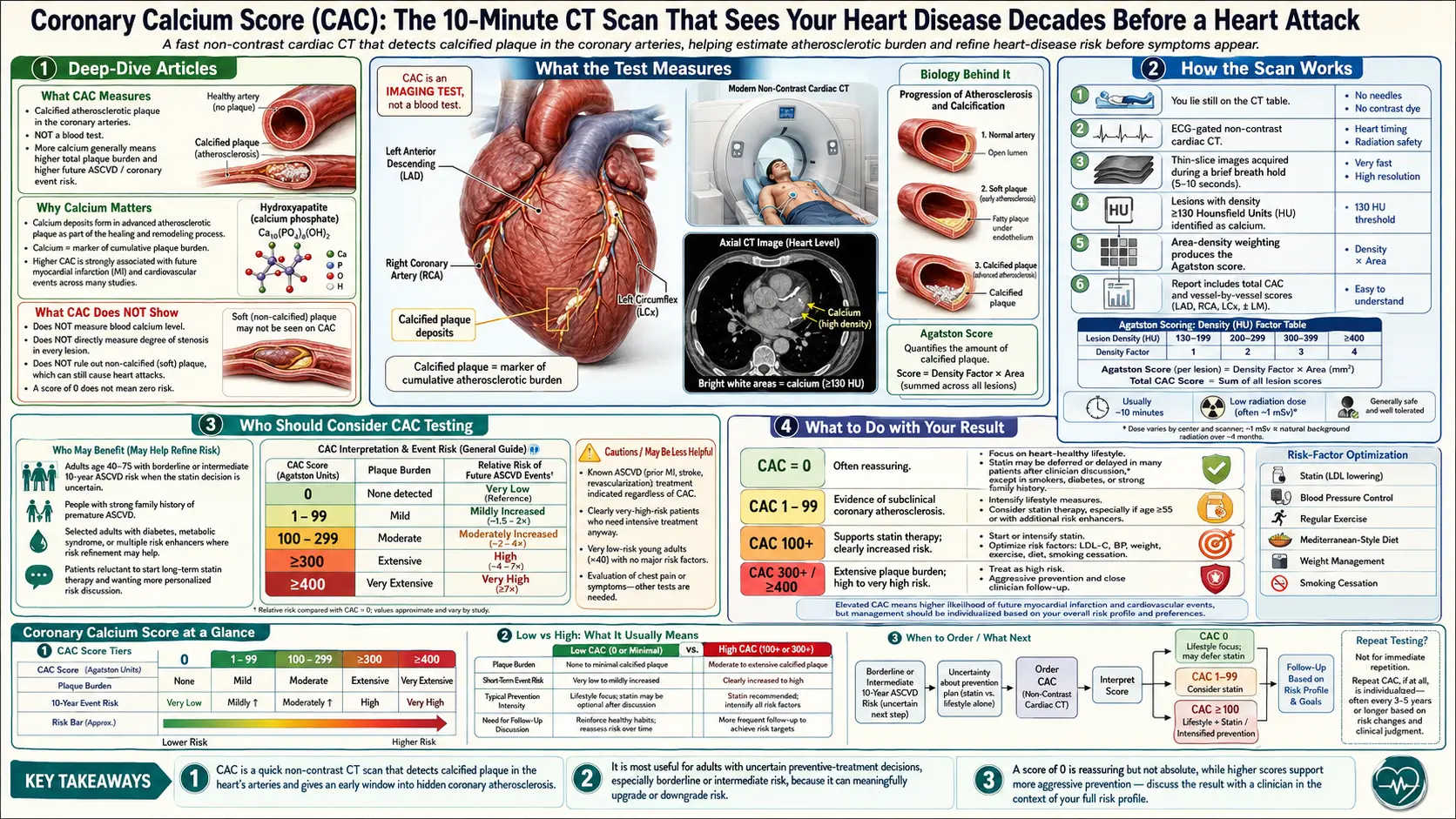
What CAC Scoring Measures
Atherosclerosis progresses through stages: lipid accumulation in the artery wall, inflammation, fibrous-cap formation, and eventually calcification. Calcium is deposited in mature plaques as a stabilization response; the total volume of coronary-artery calcium is a direct quantitative index of the total atherosclerotic burden a person has accumulated. Critically, calcification does not happen overnight — a score of zero implies no substantial atherosclerosis, while a rising score documents progression.
How the Scan Works
The patient lies on a CT scanner bed, EKG leads are placed, and the scanner acquires a few gated images timed to heart rhythm. No intravenous contrast is used. Software identifies calcified voxels in the coronary arteries and computes the Agatston score from their density and area. Total scan time is typically 10 minutes, radiation exposure is roughly 1 mSv (comparable to one year of background radiation or a mammogram).
Interpreting Your Score
- 0 — No detectable coronary calcium. Very low 10-year risk of cardiovascular events. The “warranty” may last 5–10 years before re-scanning.
- 1–99 — Mild plaque. Moderate risk; primary prevention intensifies.
- 100–299 — Moderate plaque. Strong indication for statin therapy regardless of LDL level in most guidelines.
- 300–999 — Significant disease. Aggressive risk reduction.
- ≥1000 — Extensive disease. Cardiology evaluation.
Age and Sex Percentiles
Absolute score alone can be misleading. A score of 100 in a 45-year-old (95th percentile for age) is far more alarming than the same score in a 70-year-old (below 50th percentile). Radiology reports typically include both absolute score and age/sex percentile. Percentile-based interpretation using the MESA risk-score calculator is the standard.
Who Should Consider CAC Testing
Current guidelines most clearly support CAC scoring for:
- Adults 40–75 with intermediate 10-year ASCVD risk where statin decision is uncertain.
- People with family history of premature CAD.
- People with elevated Lp(a) or elevated ApoB.
- Patients with metabolic syndrome, type 2 diabetes, or inflammatory disease.
- Asymptomatic people over 40–50 seeking to personalize prevention.
CAC scoring is not recommended as a screening tool in very young adults (it usually returns zero regardless of risk) or in patients with already established CAD (where the decision to treat is already made).
Limits — Soft Plaque Invisibility
CAC imaging visualizes only calcified plaque. Early, non-calcified “soft” plaque — which is also dangerous and can rupture — is invisible. A score of zero does not mean zero disease; it means zero calcified disease. In higher-risk patients, coronary CT angiography (CCTA) visualizes both calcified and non-calcified plaque and is increasingly used for comprehensive assessment.
What to Do with Your Result
- Score 0 and low other risk factors: Maintain lifestyle; consider re-scan in 5–10 years.
- Score 1–99: Intensify lifestyle, optimize ApoB, consider statin if other factors concerning.
- Score ≥100: Statin therapy typically indicated. Aggressive ApoB lowering. Lifestyle optimization.
- High score + symptoms (chest discomfort, unusual breathlessness): Cardiology evaluation; functional testing or CCTA may be appropriate.
Key Research Papers
Foundational and recent peer-reviewed publications on coronary artery calcium scoring, the Agatston methodology, MESA-derived risk prediction, statin decision-making, and the CAC = 0 negative-result literature. Each citation links to the full text via DOI.
- Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M Jr, Detrano R. Quantification of Coronary Artery Calcium Using Ultrafast Computed Tomography. Journal of the American College of Cardiology. 1990;15(4):827–832.
- Detrano R, Guerci AD, Carr JJ, et al. Coronary Calcium as a Predictor of Coronary Events in Four Racial or Ethnic Groups (MESA). New England Journal of Medicine. 2008;358(13):1336–1345.
- McClelland RL, Jorgensen NW, Budoff M, et al. 10-Year Coronary Heart Disease Risk Prediction Using Coronary Artery Calcium and Traditional Risk Factors: Derivation in the MESA. Journal of the American College of Cardiology. 2015;66(15):1643–1653.
- Greenland P, Blaha MJ, Budoff MJ, Erbel R, Watson KE. Coronary Calcium Score and Cardiovascular Risk. Journal of the American College of Cardiology. 2018;72(4):434–447.
- Nasir K, Bittencourt MS, Blaha MJ, et al. Implications of Coronary Artery Calcium Testing Among Statin Candidates According to American College of Cardiology/American Heart Association Cholesterol Management Guidelines. Journal of the American College of Cardiology. 2015;66(15):1657–1668.
- Budoff MJ, Young R, Burke G, et al. Ten-Year Association of Coronary Artery Calcium with Atherosclerotic Cardiovascular Disease (ASCVD) Events: The Multi-Ethnic Study of Atherosclerosis (MESA). European Heart Journal. 2018;39(25):2401–2408.
- Blaha MJ, Cainzos-Achirica M, Greenland P, et al. Role of Coronary Artery Calcium Score of Zero and Other Negative Risk Markers for Cardiovascular Disease: The Multi-Ethnic Study of Atherosclerosis (MESA). Circulation. 2016;133(9):849–858.
- Henein M, Granasen G, Wiklund U, et al. High Dose and Long-Term Statin Therapy Accelerate Coronary Artery Calcification. International Journal of Cardiology. 2015;184:581–586.
- Mortensen MB, Falk E, Li D, et al. Statin Trials, Cardiovascular Events, and Coronary Artery Calcification: Implications for a Trial-Based Approach to Statin Therapy in MESA. JACC: Cardiovascular Imaging. 2018;11(2 Pt 1):221–230.
- Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC Guideline on the Management of Blood Cholesterol. Journal of the American College of Cardiology. 2019;73(24):e285–e350.
- Erbel R, Möhlenkamp S, Moebus S, et al. Coronary Risk Stratification, Discrimination, and Reclassification Improvement Based on Quantification of Subclinical Coronary Atherosclerosis: The Heinz Nixdorf Recall Study. Journal of the American College of Cardiology. 2010;56(17):1397–1406.
- Rozanski A, Gransar H, Shaw LJ, et al. Impact of Coronary Artery Calcium Scanning on Coronary Risk Factors and Downstream Testing: The EISNER (Early Identification of Subclinical Atherosclerosis by Noninvasive Imaging Research) Prospective Randomized Trial. Journal of the American College of Cardiology. 2011;57(15):1622–1632.
- Arad Y, Goodman KJ, Roth M, Newstein D, Guerci AD. Coronary Calcification, Coronary Disease Risk Factors, C-Reactive Protein, and Atherosclerotic Cardiovascular Disease Events: The St. Francis Heart Study. Journal of the American College of Cardiology. 2005;46(1):158–165.
- Criqui MH, Denenberg JO, Ix JH, et al. Calcium Density of Coronary Artery Plaque and Risk of Incident Cardiovascular Events. JAMA. 2014;311(3):271–278.
- Hecht H, Blaha MJ, Berman DS, et al. Clinical Indications for Coronary Artery Calcium Scoring in Asymptomatic Patients: Expert Consensus Statement from the Society of Cardiovascular Computed Tomography. Journal of Cardiovascular Computed Tomography. 2017;11(2):157–168.
- Sarwar A, Shaw LJ, Shapiro MD, et al. Diagnostic and Prognostic Value of Absence of Coronary Artery Calcification. JACC: Cardiovascular Imaging. 2009;2(6):675–688.
Live PubMed Searches
Live PubMed queries that update as new papers are indexed.
- PubMed: coronary artery calcium risk stratification
- PubMed: MESA coronary calcium study
- PubMed: CAC score zero warranty
- PubMed: CAC progression and statin therapy
- PubMed: ACC/AHA CAC guidelines
- PubMed: CAC and soft plaque (CCTA)
- PubMed: CAC age and sex percentiles
- PubMed: Agatston score methodology
- PubMed: CAC and cardiovascular events
- PubMed: CAC radiation dose
External Authoritative Resources
- MedlinePlus — Laboratory Tests Reference
- Lab Tests Online — Patient-Oriented Lab Test Reference (AACC)
- StatPearls / NCBI Bookshelf — Clinical Laboratory Reference
Connections
- Agatston Score Calculation and Interpretation
- CAC vs Other Cardiac Tests
- Soft Plaque and CAC Limitations
- MESA Risk Calculator and Age Percentiles
- Reversal Plaque Stabilization and Lifestyle
- CAC Zero and the Power of Negative Result
- Insurance Cost and Access
- CAC in Women and Younger Adults
- Statin Threshold and CAC
- Atherosclerosis
- ApoB
- Lipoprotein(a)
- Lipid Panel
- Inflammatory Markers
- Full Body MRI
- Coronary Artery Disease
- Cardiovascular Disease
- Calcium