Gum Disease
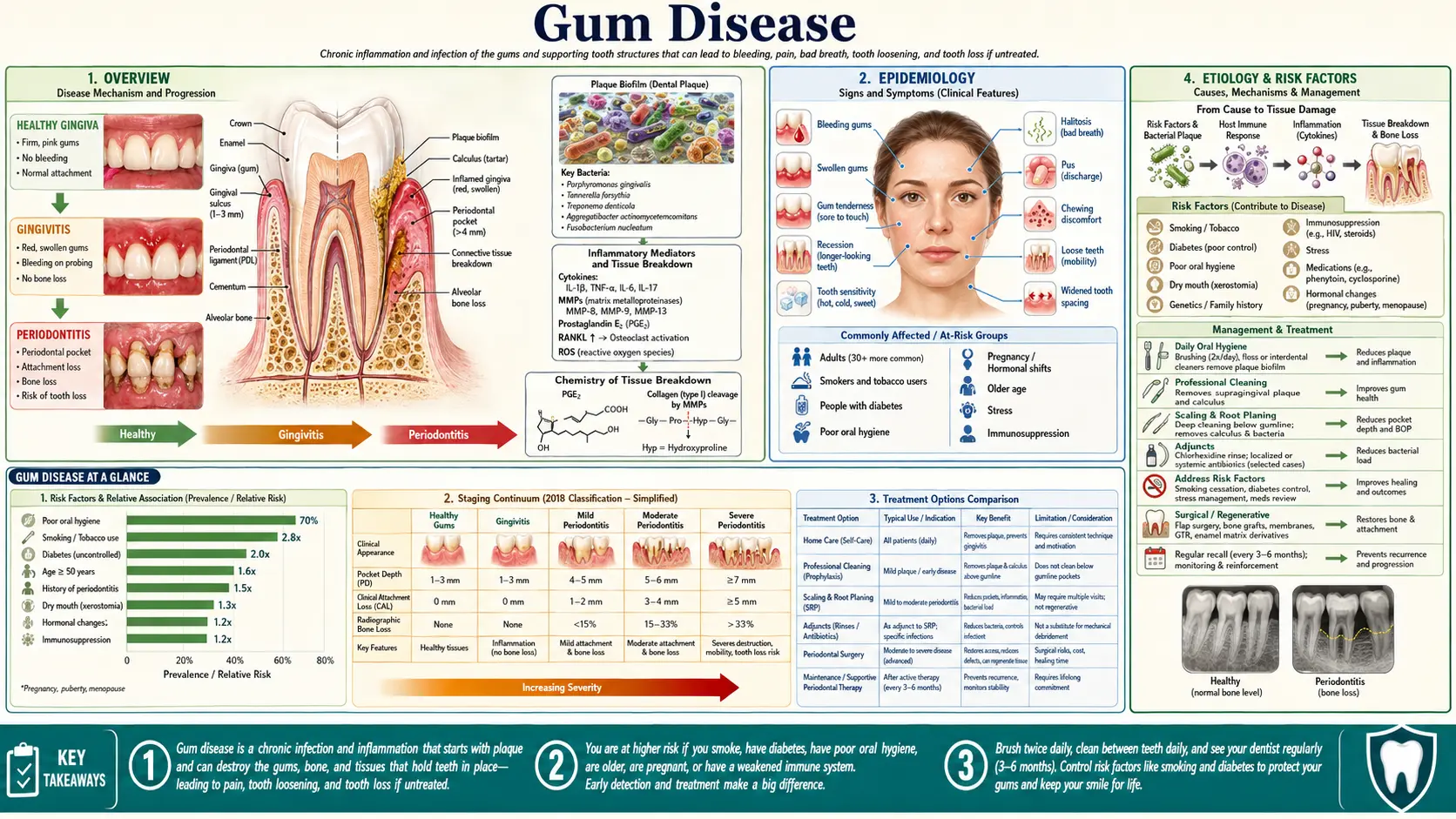
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- Diagnosis
- Treatment
- Complications
- Prognosis
- Prevention
- Recent Research and Advances
- Research Papers
- Connections
- Featured Videos
1. Overview
Gum disease — known medically as periodontal disease — is inflammation of the tissues that surround and support your teeth: the gums, the connective fibers that anchor each tooth, and the underlying jawbone. It exists on a spectrum. The mild, early, and reversible form is gingivitis — gums that are red, puffy, and bleed when you brush or floss. If the inflammation is allowed to continue, it can progress to periodontitis, in which the gum pulls away from the tooth, the supporting bone is steadily destroyed, and the tooth eventually loosens and can be lost. The bone loss of periodontitis does not grow back on its own; that is why catching the problem early matters so much.
Here is the single most useful thing to know on this whole page: bleeding when you brush is not normal. Many people assume pink in the sink means they brushed too hard, but bleeding gums are the body's signal that the tissue is inflamed and infected. Healthy gums do not bleed during ordinary brushing or flossing. Treated as a warning rather than an annoyance, that small amount of blood is often your earliest — and most reversible — chance to stop the disease.
Gum disease is the most common chronic inflammatory condition in humans and a leading cause of tooth loss in adults worldwide. And yet, almost uniquely among the major chronic diseases, it is largely preventable with daily habits and routine professional care. This page explains the spectrum, the bacteria and the body's own inflammation that drive it, the honest state of the evidence linking gum health to the heart, diabetes, joints, and the brain, and what actually works to prevent and treat it.
2. Epidemiology
Gum disease is extraordinarily common. In the United States, national surveys (NHANES) estimate that roughly 42–47% of adults aged 30 and older have some form of periodontitis, and that figure climbs to about 70% of adults aged 65 and older. Gingivitis — the milder, reversible stage — is more common still, present in some form in a majority of adults at any given time. Severe periodontitis affects roughly 1 in 10 adults and is consistently ranked among the most prevalent diseases of mankind.
The burden is not evenly distributed. Rates of severe disease are higher among older adults, men, smokers, people with diabetes, and people with lower income or less access to dental care. Because much of early gum disease causes little or no pain, large numbers of people have it without knowing — one reason routine dental check-ups, where a clinician measures the gums directly, catch the problem before symptoms force the issue.
3. Pathophysiology
Gum disease begins with dental plaque — a soft, sticky film of bacteria (a biofilm) that constantly forms on teeth, especially along the gumline. Plaque itself is normal; everyone grows it. The problem starts when plaque is not removed and is allowed to mature and thicken. Over hours to days the bacterial community shifts from the relatively harmless species of a healthy mouth toward a more aggressive, inflammation-driving mix — a change called dysbiosis. If plaque is not disturbed, minerals from saliva harden it into tartar (calculus), a rough deposit that you cannot brush off and that gives still more bacteria a place to cling.
One organism, Porphyromonas gingivalis, is described by researchers as a keystone pathogen. The idea is simple: P. gingivalis does not need to be numerous to do damage. Even in small amounts it can tip the whole biofilm community out of balance and blunt the local immune defenses, allowing the entire dysbiotic community to become more harmful. It is less a single villain than a tiny ringleader that destabilizes the neighborhood.
Crucially, most of the tissue destruction in periodontitis is done not by the bacteria directly but by the body's own immune response to them. In gingivitis, the gum mounts a contained, reversible inflammatory reaction — redness, swelling, easy bleeding. In susceptible people the inflammation becomes chronic and dysregulated. Immune cells release enzymes and signaling molecules that, while trying to fight the infection, break down the collagen fibers anchoring the tooth and activate cells that resorb bone. The gum detaches from the tooth surface, forming a deepening space called a periodontal pocket that is even harder to clean — a self-feeding cycle of more bacteria, more inflammation, and more lost attachment and bone.
4. Etiology and Risk Factors
The necessary trigger is the dysbiotic plaque biofilm, but whether a given person develops mild or severe disease depends heavily on risk factors that shape the immune response:
- Poor oral hygiene — the foundational factor. Inadequate brushing and cleaning between the teeth lets plaque mature and tartar form.
- Smoking and tobacco — one of the strongest and most consistent risk factors. Smoking impairs the gum's blood supply and immune defenses, drives faster bone loss, and worsens treatment response. Disturbingly, smoking can mask the warning sign of bleeding by constricting blood vessels, so a smoker's gums may look deceptively healthy while disease advances underneath.
- Diabetes — a powerful, two-way relationship covered in detail in the Complications section. Poorly controlled blood sugar amplifies gum inflammation, and severe gum disease in turn worsens blood-sugar control.
- Genetics and susceptibility — people vary in how intensely their immune system reacts to the same plaque, which is part of why some people with mediocre hygiene keep their teeth while others lose teeth despite reasonable care.
- Age — prevalence rises steadily with age, reflecting cumulative exposure rather than aging being a direct cause.
- Dry mouth and medications — saliva washes and buffers the mouth, so reduced flow (from many common drugs, or conditions affecting the salivary glands) raises risk.
- Stress — associated with worse gum health, partly through neglected self-care and partly through effects on inflammation.
- Hormonal changes — puberty, pregnancy, and menopause can exaggerate the gum's response to plaque. Pregnancy gingivitis is common and usually reversible with good cleaning and professional care, but it should not be ignored.
5. Clinical Presentation
Gingivitis tends to be subtle. The classic signs are gums that look red or darker than the healthy pale pink, appear swollen or puffy, and bleed during brushing or flossing. There is usually no pain. Because gingivitis is reversible, recognizing these signs early is the whole game — improved daily cleaning and a professional cleaning can return the gum to health within weeks.
Periodontitis adds signs of lost support:
- Persistent bad breath or a bad taste that does not clear with brushing.
- Gum recession — teeth that look longer as the gum pulls back, sometimes with new sensitivity to hot or cold.
- Spaces opening up between teeth, or teeth that seem to be shifting or no longer meet the same way when you bite.
- Loose teeth as the supporting bone is lost.
- Pus at the gumline or a gum that is tender to touch (a sign of more active infection).
It helps to picture the two stages as a continuum rather than two separate diseases. Gingivitis is inflammation that has reached the gum but not yet the supporting structures — like a sprain that can fully heal. Periodontitis is what happens when that inflammation crosses the threshold and begins eroding the foundation — the connective fibers and bone — which is the part that does not grow back. The visible symptoms above (recession, spacing, looseness) are all downstream consequences of that quiet, ongoing loss of foundation.
A key trap: periodontitis is often painless until it is advanced. Many people do not seek care until a tooth becomes loose — by which point substantial, non-recoverable bone has already been lost. That is exactly why "no pain" is not the same as "no disease," and why the painless early bleeding deserves attention.
6. Diagnosis
Gum disease is diagnosed by direct examination, not by how the teeth feel. The core tools are:
- Periodontal probing. The clinician gently slides a thin, blunt, millimeter-marked probe into the space between gum and tooth and records the pocket depth at several points around each tooth. Healthy sites are about 1–3 mm; deeper pockets (4 mm and beyond) signal lost attachment and harder-to-clean disease. Bleeding when the probe is placed is recorded as bleeding on probing, an objective marker of active inflammation.
- Dental X-rays. Bitewing and periapical radiographs show the level of the bone supporting each tooth. Because bone loss is the irreversible hallmark of periodontitis, X-rays both confirm the diagnosis and gauge severity.
- Clinical attachment level. Combining pocket depth with how far the gum has receded gives the truest measure of how much support a tooth has actually lost.
Since 2017–2018, periodontitis has been described using a staging and grading system (from the World Workshop classification). Staging (I–IV) captures how severe and extensive the damage is — how much attachment and bone have been lost. Grading (A–C) estimates how fast it is progressing and factors in risk such as smoking and diabetes. In plain terms: staging answers "how bad is it now?" and grading answers "how quickly is it likely to get worse?" — together guiding how aggressive treatment needs to be.
7. Treatment
The goal of treatment is to disrupt and reduce the bacterial biofilm, calm the inflammation, and create a mouth that the patient can keep clean. Care is staged to severity.
For gingivitis, treatment is straightforward and usually effective: a professional cleaning to remove plaque and tartar, plus coaching on better daily home care. Because gingivitis has not yet destroyed bone, gums can fully recover.
For periodontitis, the first-line, non-surgical treatment is scaling and root planing (sometimes called a "deep cleaning"). The clinician removes plaque and tartar from above and below the gumline and smooths the root surfaces so the gum can reattach more closely and pockets can shrink. This is the workhorse of periodontal therapy and resolves or controls disease in many people.
- Good home care is half the treatment. Professional cleaning removes what has accumulated, but biofilm regrows daily. Without effective brushing and cleaning between the teeth, pockets refill within weeks. The most successful outcomes pair professional treatment with genuinely improved daily habits.
- Adjunctive antimicrobials. In selected cases, locally placed antibiotics or antiseptics in deep pockets, or short courses of systemic antibiotics for aggressive disease, can add benefit. They are an add-on to mechanical cleaning, not a replacement for it.
- Surgery and regeneration. For advanced disease, a periodontist may perform flap surgery to access and clean deep pockets, or use bone grafts and guided tissue regeneration to rebuild some lost support. Gum (soft-tissue) grafts can cover exposed roots where recession is a problem.
- Maintenance. Periodontitis is a chronic condition. After active treatment, ongoing periodontal maintenance visits (often every 3–4 months) keep the biofilm in check and catch any relapse early. Skipping maintenance is a common reason disease returns.
Home Care — What the Evidence Supports
- Brush twice a day with a fluoride toothpaste. This is the bedrock and is well supported. Spend the time to clean along the gumline, where plaque does its damage.
- Clean between your teeth daily. A toothbrush cannot reach the surfaces between teeth, and that is where much gum disease starts. The honest state of the evidence: the data for string floss reducing gum disease are weak and inconsistent — not because cleaning between teeth doesn't matter, but because flossing is hard to do well and trials are short. The stronger evidence is for interdental brushes (small bristled picks) where the gaps allow them; reviews find they reduce plaque and gingival bleeding more reliably than floss. Use whatever you will actually do consistently; for many people interdental brushes are easier and more effective.
- Electric vs. manual toothbrush. A Cochrane review found powered toothbrushes reduce plaque and gum bleeding modestly more than manual brushing, particularly oscillating-rotating types. A manual brush used well is still effective; the electric brush is a help, not a requirement.
- Chlorhexidine mouthwash — short-term only. Chlorhexidine is a genuinely effective antiseptic for short bursts (for example, after surgery or when brushing is temporarily limited). It is not for everyday long-term use because it stains teeth and alters taste. It does not replace mechanical cleaning.
- The limits of ordinary mouthwash. Cosmetic and most over-the-counter rinses freshen breath and may slightly reduce plaque, but they do not remove established plaque or tartar and are not a substitute for brushing and cleaning between teeth.
Claims That Don't Hold Up
- Oil pulling. Swishing oil is sometimes promoted as a gum-disease cure. The evidence is weak and of poor quality; trials are small and short. It is, at best, an unproven add-on and is not a substitute for brushing, cleaning between teeth, and professional care. Relying on it instead of real treatment lets disease progress.
- Charcoal toothpaste. Marketed for whitening and "detox," charcoal pastes are often abrasive and can wear down enamel and exposed root surfaces over time. They have no proven benefit for gum disease and may do harm.
Nutrition and the Gums
Diet plays a supporting, not starring, role — and the honest evidence varies by nutrient:
- Vitamin C. Severe deficiency (scurvy) classically causes swollen, bleeding gums, because vitamin C is required to build the collagen that holds gum tissue together — a vivid historical illustration of the gum-nutrition link. For most modern adults who are not deficient, however, taking extra vitamin C does not cure ordinary plaque-driven gum disease. Adequate intake matters; megadoses are not a treatment.
- Vitamin D. Has roles in immune regulation and bone, and low levels are associated with worse periodontal health in observational studies. Whether supplementing improves gum disease in people who are not deficient is not yet established.
- Sugar and the biofilm. Frequent dietary sugar feeds the bacterial biofilm and is a clear driver of tooth decay; its independent effect on periodontitis is less direct but reducing sugar supports overall oral health.
- Omega-3 fatty acids. Because much gum damage is inflammatory, omega-3s have been studied as an adjunct. Some small trials suggest modest benefit alongside scaling and root planing, but the evidence is preliminary — promising, not proven, and not a stand-alone therapy.
8. Complications
The direct complications of untreated periodontitis are local: deepening pockets, abscesses, gum recession, loosening, and ultimately tooth loss — which in turn affects chewing, nutrition, speech, and self-confidence. Beyond the mouth lies the much-discussed oral–systemic connection, which deserves to be reported carefully and honestly. Gum disease is genuinely linked to several whole-body conditions, but for most of these the evidence shows association and biological plausibility — not proof that treating gums prevents the other disease. Here is where each one actually stands.
Cardiovascular Disease
This is the best-studied link. People with periodontitis have a higher rate of atherosclerotic cardiovascular disease, and the association persists after adjusting for shared risks like smoking. There is real biological plausibility: P. gingivalis and other oral bacteria have been detected within atherosclerotic plaques, and chronic gum inflammation raises systemic inflammatory markers. In a landmark randomized trial, Tonetti and colleagues (NEJM, 2007) showed that intensive periodontal treatment improved endothelial function (a measure of blood-vessel health) within months — striking evidence that treating the gums affects the vasculature. The crucial caveat: no trial has yet proven that treating gum disease prevents heart attacks or strokes. Consensus reports describe the relationship as a strong, plausible association warranting attention, while stopping short of declaring gum disease a proven cause of heart disease.
Diabetes (a two-way street)
The diabetes link is the most firmly established and is bidirectional. Poorly controlled diabetes worsens gum disease by amplifying inflammation and impairing healing; in turn, the chronic inflammation of severe periodontitis can worsen blood-sugar control. Encouragingly, the evidence here goes beyond association: treating periodontitis produces a modest improvement in HbA1c (long-term blood sugar) in people with type 2 diabetes — on the order of a few tenths of a percentage point in meta-analyses, a small but real metabolic benefit. For people with diabetes, gum care is part of diabetes care.
Rheumatoid Arthritis
Periodontitis and rheumatoid arthritis (RA) share inflammatory pathways and frequently co-occur. A specific mechanistic thread has drawn intense interest: certain oral bacteria can drive citrullination — a protein modification that, in RA, becomes a target of the autoimmune attack (anti-citrullinated protein antibodies). P. gingivalis uniquely produces an enzyme that citrullinates proteins, and other oral bacteria can induce host citrullination, offering a plausible route by which gum infection could prime the autoimmunity of RA. This remains an active, exciting research link rather than settled cause-and-effect; see the Rheumatoid Arthritis page.
Adverse Pregnancy Outcomes
Periodontitis has been associated with preterm birth and low birth weight. The association is real, but trials of treating gum disease during pregnancy have generally not shown that it prevents these outcomes. The practical message is unchanged: good gum care is safe and worthwhile in pregnancy, but it should not be sold as a guaranteed way to prevent preterm birth.
Alzheimer's Disease — intriguing, not established
A widely publicized 2019 study (Dominy et al., Science Advances) reported finding P. gingivalis and its toxic enzymes (gingipains) in the brains of people with Alzheimer's disease, and showed that small-molecule inhibitors of those enzymes reduced bacterial load and neurodegeneration in mice. It is a fascinating hypothesis that a gum pathogen might contribute to Alzheimer's. But it is essential to be honest: this does not establish that gum disease causes Alzheimer's. Finding a bacterium in diseased brain tissue does not prove it started the disease, the human evidence is still observational, and a drug trial targeting this pathway did not succeed. Treat it as a genuinely interesting line of research — not as a reason for fear, and not as proof. The take-home is the same one good evidence already supports: keep your gums healthy for your gums' sake.
9. Prognosis
The outlook depends almost entirely on the stage at which it is caught and on the patient's ongoing habits. Gingivitis is fully reversible — with better cleaning and a professional scaling, inflamed gums return to health, usually within weeks, with no lasting damage. This is the great window of opportunity, and it is why responding to bleeding gums early is so valuable.
Periodontitis cannot be cured in the sense of regrowing lost bone, but it can be controlled and stabilized very effectively. With proper treatment and — this is the deciding factor — consistent home care and regular maintenance visits, most people can halt the disease, keep their teeth for life, and avoid further bone loss. Outcomes are clearly worse in people who continue to smoke or whose diabetes is poorly controlled, both of which are modifiable. The disease's tendency to relapse if maintenance lapses is why periodontitis is best thought of as a chronic condition to manage, much like blood pressure, rather than a one-time infection to clear.
10. Prevention
Gum disease is one of the most preventable of the common chronic diseases. The essentials:
- Brush twice daily with a fluoride toothpaste, taking care along the gumline.
- Clean between your teeth every day — interdental brushes where they fit, floss where they don't. Consistency matters more than the tool.
- See a dentist or hygienist regularly so that plaque and tartar are removed professionally and any early disease is caught while it is still reversible.
- Don't smoke — and if you do, quitting is one of the most powerful things you can do for your gums (and your whole body).
- Control diabetes — stable blood sugar protects the gums, and healthy gums help blood sugar.
- Don't ignore bleeding gums. Bleeding is the early, reversible warning. Acting on it is the cheapest and most effective treatment there is.
A Simple Daily Routine That Works
You do not need an elaborate regimen — you need a consistent one. A practical, evidence-aligned routine looks like this:
- Morning and night, brush for two minutes with a fluoride toothpaste, angling the bristles slightly toward the gumline so you clean the exact spot where disease begins. A soft brush is gentle enough; you do not need to scrub hard — aggressive brushing can cause recession without removing more plaque.
- Once a day, clean between every tooth with an interdental brush sized to each gap, or with floss where the brush won't fit. Doing this at night, before brushing, means the toothpaste's fluoride then reaches the freshly cleaned surfaces.
- Don't rinse the toothpaste away with a big swish of water right after brushing — spitting and leaving a thin film lets the fluoride keep working.
- Replace your brush head roughly every three months, or sooner once the bristles splay.
- Keep your dental check-ups on the schedule your dentist recommends. Professional cleaning removes the hardened tartar that no home tool can.
The reason this matters is biological: plaque biofilm fully re-establishes itself within about a day, which is why the disease is controlled by what you do daily, not by any occasional deep effort. The classic "experimental gingivitis" studies showed exactly this — when healthy volunteers stopped cleaning their teeth, gum inflammation reliably appeared within days and reliably resolved once cleaning resumed. Daily consistency is the whole mechanism.
11. Recent Research and Advances
Periodontal science has moved decisively from a "bad bacteria" model to a more sophisticated host-response and dysbiosis model: it is the interaction between an imbalanced biofilm and a dysregulated immune system — not any single germ — that destroys tissue. This has reframed gum disease as fundamentally an inflammatory disease, opening interest in host-modulation therapies that calm the destructive immune response rather than only attacking bacteria.
The 2017–2018 World Workshop classification, with its staging-and-grading framework, standardized how clinicians describe disease severity and risk, improving consistency of diagnosis and research. The oral–systemic field remains the most active and most scrutinized frontier: the diabetes link is now solid enough to shape clinical guidelines, the cardiovascular link is strong and plausible but unproven as causal, and the Alzheimer's and rheumatoid-arthritis links are genuinely intriguing mechanistic leads that the field is careful not to overstate. Researchers continue to test adjuncts — locally delivered antimicrobials, probiotics, and omega-3 / resolvin pathways — layered onto the proven foundation of mechanical biofilm removal. Across all of it, one practical message has only gotten stronger: daily plaque control plus regular professional care prevents most of this disease.
12. References & Research
Historical Background
Awareness of diseased gums is ancient — descriptions of gum inflammation and loose teeth appear in early Egyptian, Greek, and Roman writings, and the swollen, bleeding gums of scurvy were a notorious affliction of sailors centuries before vitamin C was identified, providing one of history's clearest demonstrations that nutrition and gum health are connected. In the early twentieth century the "focal infection" theory held that oral infections seeded disease throughout the body, prompting an era of overzealous tooth extraction; the theory was largely discredited and abandoned by mid-century as an overreach. Modern, evidence-based oral–systemic medicine has since revisited the connection on firmer ground, distinguishing genuine inflammatory links (notably diabetes and cardiovascular disease) from unproven causal claims. The 2017 World Workshop, jointly convened by the American Academy of Periodontology and the European Federation of Periodontology, produced the current staging-and-grading classification that frames how gum disease is diagnosed and described today.
Key Research Papers
- Tonetti MS, D'Aiuto F, Nibali L, et al. Treatment of periodontitis and endothelial function. New England Journal of Medicine. 2007;356(9):911-920.
- Pihlstrom BL, Michalowicz BS, Johnson NW. Periodontal diseases. The Lancet. 2005;366(9499):1809-1820.
- Tonetti MS, Jepsen S, Jin L, Otomo-Corgel J. Impact of the global burden of periodontal diseases on health, nutrition and wellbeing of mankind: A call for global action. Journal of Clinical Periodontology. 2017;44(5):456-462.
- Caton JG, Armitage G, Berglundh T, et al. A new classification scheme for periodontal and peri-implant diseases and conditions — Introduction and key changes from the 1999 classification. Journal of Periodontology. 2018;89(S1):S1-S8.
- Hajishengallis G, Chavakis T. Local and systemic mechanisms linking periodontal disease and inflammatory comorbidities. Nature Reviews Immunology. 2021;21(7):426-440.
- Tonetti MS, Van Dyke TE. Periodontitis and atherosclerotic cardiovascular disease: consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. Journal of Periodontology. 2013;84(4-S):S24-S29.
- Sanz M, Marco del Castillo A, Jepsen S, et al. Periodontitis and cardiovascular diseases: Consensus report. Journal of Clinical Periodontology. 2020;47(3):268-288.
- Preshaw PM, Alba AL, Herrera D, et al. Periodontitis and diabetes: a two-way relationship. Diabetologia. 2011;55(1):21-31.
- Lalla E, Papapanou PN. Diabetes mellitus and periodontitis: a tale of two common interrelated diseases. Nature Reviews Endocrinology. 2011;7(12):738-748.
- Sanz M, Ceriello A, Buysschaert M, et al. Scientific evidence on the links between periodontal diseases and diabetes: Consensus report and guidelines of the joint workshop by the IDF and EFP. Journal of Clinical Periodontology. 2017;45(2):138-149.
- Simpson TC, Weldon JC, Worthington HV, et al. Treatment of periodontal disease for glycaemic control in people with diabetes mellitus. Cochrane Database of Systematic Reviews. 2015;(11):CD004714.
- Konig MF, Abusleme L, Reinholdt J, et al. Aggregatibacter actinomycetemcomitans-induced hypercitrullination links periodontal infection to autoimmunity in rheumatoid arthritis. Science Translational Medicine. 2016;8(369):369ra176.
- Dominy SS, Lynch C, Ermini F, et al. Porphyromonas gingivalis in Alzheimer's disease brains: Evidence for disease causation and treatment with small-molecule inhibitors. Science Advances. 2019;5(1):eaau3333.
- Worthington HV, MacDonald L, Poklepovic Pericic T, et al. Home use of interdental cleaning devices, in addition to toothbrushing, for preventing and controlling periodontal diseases and dental caries. Cochrane Database of Systematic Reviews. 2019;(4):CD012018.
- Yaacob M, Worthington HV, Deacon SA, et al. Powered versus manual toothbrushing for oral health. Cochrane Database of Systematic Reviews. 2014;(6):CD002281.
- Chapple ILC, Bouchard P, Cagetti MG, et al. Interaction of lifestyle, behaviour or systemic diseases with dental caries and periodontal diseases: consensus report of group 2 of the joint EFP/ORCA workshop. Journal of Clinical Periodontology. 2017;44(S18):S39-S51.
Research Papers
Explore the current peer-reviewed literature on gum disease and its links to whole-body health through these live PubMed searches. Each opens a continuously updated list of studies in a new tab.
- Periodontitis pathogenesis
- Gingivitis treatment
- P. gingivalis keystone pathogen
- Periodontitis and cardiovascular disease
- Periodontitis and glycemic control
- Periodontitis and rheumatoid arthritis
- Periodontal disease and Alzheimer's
- Scaling and root planing outcomes
- Interdental cleaning and bleeding
- Smoking and periodontal disease
- Periodontitis staging and grading
- Omega-3 fatty acids and periodontitis
Connections
- Cardiovascular Disease — periodontitis is associated with vascular disease; treating gums improves endothelial function.
- Atherosclerosis — oral bacteria have been detected within atherosclerotic plaques.
- Endocarditis — oral bacteria entering the bloodstream can seed infection of the heart valves.
- Diabetes — a firmly established two-way relationship with gum disease.
- Insulin Resistance — chronic inflammation links metabolic and periodontal health.
- Rheumatoid Arthritis — shared inflammation and the citrullination hypothesis.
- Alzheimer's Disease — an intriguing but unproven P. gingivalis link.
- Dementia — oral health and cognitive decline are an active research area.
- Gastroesophageal Reflux Disease — acid exposure and dry mouth affect oral tissues.
- Vitamin C — essential for gum collagen; deficiency causes scurvy's bleeding gums.
- Vitamin D3 — immune and bone roles relevant to periodontal health.
- Vitamin K — supports bone metabolism and calcium regulation.
- Calcium — a building block of the jawbone that supports the teeth.
- Magnesium — involved in bone health and inflammation balance.
- Omega-3 Fatty Acids — studied as an anti-inflammatory adjunct in periodontal care.
- ENT — the head-and-neck specialty section.