Herniated Disc
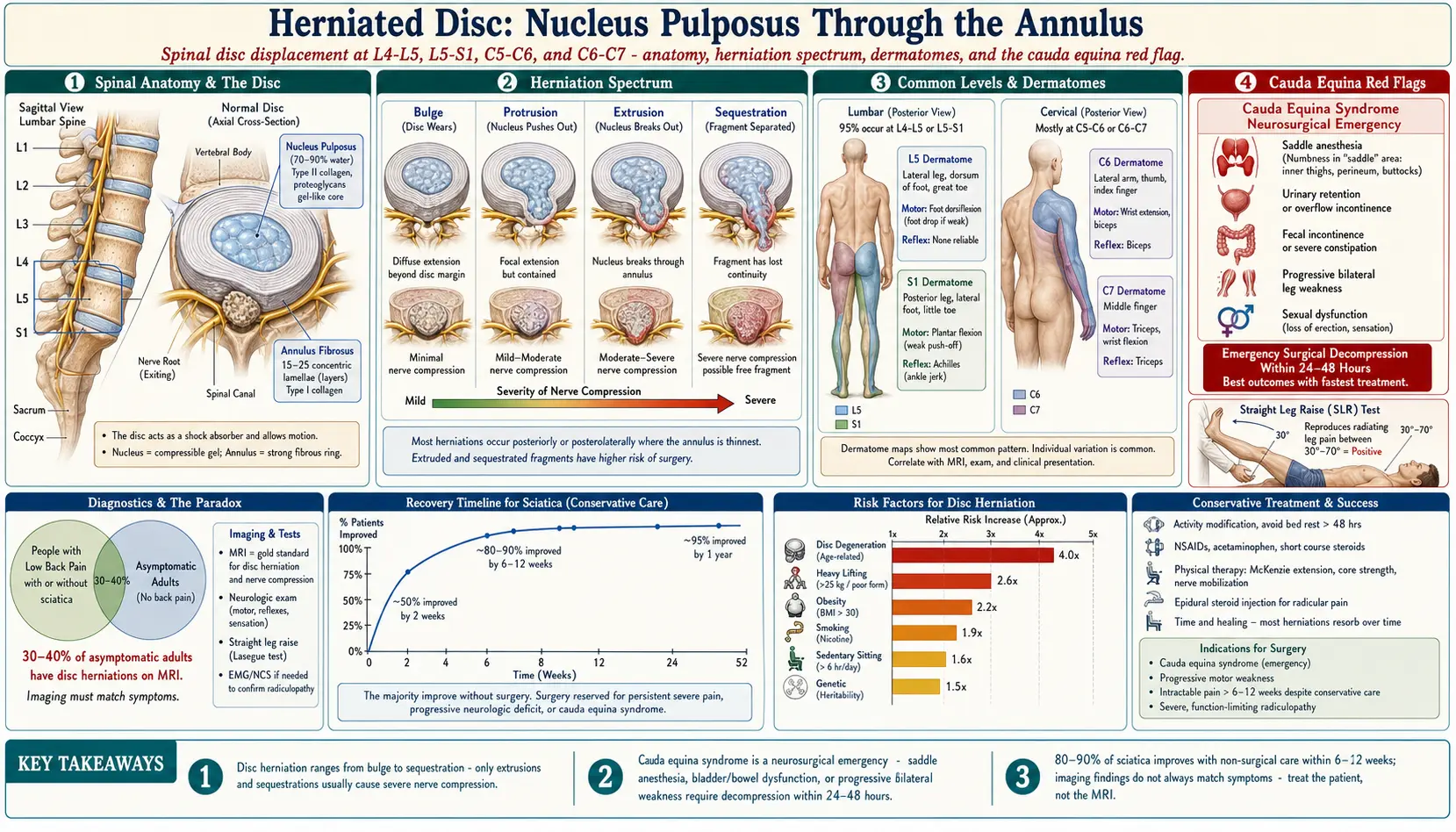
Table of Contents
- Spinal Anatomy
- What Happens in a Herniation
- Common Locations
- Sciatica and Radiculopathy
- Causes and Risk Factors
- Symptoms and Red Flags
- Diagnosis
- Conventional Treatments
- Natural and Naturopathic Approaches
- Spinal Decompression
- Exercise and Rehabilitation
- Complementary Therapies
- Important Cautions
- References & Research
- Featured Videos
Spinal Anatomy
Understanding the anatomy of the spine is essential for comprehending how disc herniations occur and cause symptoms:
- Vertebrae: The spine consists of 33 vertebrae stacked in a column: 7 cervical (neck), 12 thoracic (mid-back), 5 lumbar (lower back), 5 fused sacral, and 4 fused coccygeal. Each vertebra has a solid body anteriorly and a bony arch posteriorly that forms the spinal canal, through which the spinal cord passes.
- Intervertebral discs: Between each pair of vertebrae sits a disc that acts as a shock absorber, load distributor, and spacer allowing spinal flexibility. There are 23 intervertebral discs in the adult spine.
- Nucleus pulposus: The inner core of each disc is a gel-like substance composed primarily of water (70-90%), proteoglycans, and type II collagen. This highly hydrated center gives the disc its ability to absorb compressive forces. The water content decreases with age, reducing disc height and shock absorption capacity.
- Annulus fibrosus: The outer ring of the disc consists of 15-25 concentric layers of type I collagen fibers arranged in alternating angles. This layered design provides tremendous tensile strength and contains the nucleus pulposus under pressure. The outer annulus has nerve supply and blood supply, while the inner annulus and nucleus are avascular.
- Spinal nerves: Nerve roots exit the spinal canal through openings called foramina between each pair of vertebrae. These nerve roots can be compressed or irritated by a herniated disc, producing pain, numbness, or weakness in the areas they innervate.
What Happens in a Herniation
A herniated disc (also called a slipped disc or ruptured disc) occurs when the nucleus pulposus pushes through a weakened or torn area of the annulus fibrosus. This process exists on a spectrum of severity:
Disc Bulge
The disc extends beyond its normal boundary uniformly, like a hamburger that is too large for its bun. The annulus remains intact. Bulges are extremely common with aging and are often found incidentally on imaging in people without symptoms.
Protrusion
The nucleus pushes into the annulus, creating a focal outpouching. The outermost annular fibers remain intact, but the disc extends asymmetrically in one direction. The base of the protrusion is wider than the extension.
Extrusion
The nucleus breaks through the full thickness of the annulus but remains connected to the parent disc material. The extruded portion is narrower at its base than at its tip, often forming a mushroom shape. This stage typically produces the most significant nerve compression and symptoms.
Sequestration
A fragment of the nucleus breaks free completely from the parent disc and migrates within the spinal canal. This free fragment can travel superiorly or inferiorly and may compress nerve roots at different levels than where the original herniation occurred. Sequestered fragments may eventually be reabsorbed by the body through an inflammatory process.
Common Locations
Disc herniations occur most frequently in the regions of the spine with the greatest mobility and mechanical stress:
Lumbar Spine (Lower Back)
The lumbar spine bears the greatest compressive load and is the most common site for disc herniation. Approximately 95% of lumbar herniations occur at two levels:
- L4-L5: The most common level for lumbar disc herniation. Compression of the L5 nerve root causes pain radiating down the lateral leg to the top of the foot and big toe. Weakness in ankle dorsiflexion (foot drop) and great toe extension may occur.
- L5-S1: The second most common level. Compression of the S1 nerve root causes pain radiating down the posterior leg and into the lateral foot and sole. The ankle jerk reflex may be diminished, and weakness in plantar flexion (pushing off during walking) may develop.
Cervical Spine (Neck)
The cervical spine is the second most common location for disc herniation. The most frequently affected levels are:
- C5-C6: Compression of the C6 nerve root causes pain radiating from the neck into the biceps, lateral forearm, thumb, and index finger. The biceps reflex may be diminished, and weakness in wrist extension and biceps can occur.
- C6-C7: Compression of the C7 nerve root causes pain radiating into the triceps, posterior forearm, and middle finger. The triceps reflex may be affected, and weakness in wrist flexion, finger extension, and triceps may develop.
Thoracic Spine
Thoracic herniations are relatively rare (less than 1% of all herniations) due to the stabilizing effect of the rib cage. When they do occur, they can cause mid-back pain and, in severe cases, spinal cord compression with lower extremity weakness or myelopathy.
Sciatica and Radiculopathy
Radiculopathy refers to the constellation of symptoms (pain, numbness, tingling, weakness) that occur when a spinal nerve root is compressed or irritated. Sciatica is the specific term for radiculopathy involving the sciatic nerve, which forms from the L4-S3 nerve roots.
- Pain pattern: Sciatic pain typically radiates from the lower back or buttock down the posterior or lateral thigh, often extending below the knee into the calf, ankle, or foot. The pain is often described as sharp, burning, or electrical in nature.
- Mechanism: The herniated disc material directly compresses the nerve root and also triggers a chemical inflammatory response. The nucleus pulposus contains phospholipase A2 and other inflammatory mediators that cause nerve inflammation even without direct mechanical compression.
- Neurological symptoms: Beyond pain, nerve compression can cause numbness (in a specific dermatomal pattern), tingling or pins-and-needles sensations, and muscle weakness in the muscles supplied by the affected nerve root.
- Prognosis: The good news is that approximately 80-90% of sciatica cases from disc herniation resolve within 6-12 weeks with conservative treatment. The body's inflammatory response gradually breaks down and reabsorbs the herniated disc material, a process called phagocytic resorption.
Causes and Risk Factors
- Age-related disc degeneration: As discs lose water content with aging (beginning in the third decade of life), they become less flexible, more brittle, and more susceptible to tearing. Disc degeneration is the primary predisposing factor for herniation.
- Heavy lifting: Lifting heavy objects with improper form (bending at the waist rather than the knees, twisting while lifting) dramatically increases intradiscal pressure and can cause acute herniation. Intradiscal pressure is highest when bending forward and lifting simultaneously.
- Obesity: Excess body weight places chronic compressive stress on the lumbar discs. Every additional 10 pounds of body weight adds approximately 40 pounds of compressive force to the lumbar spine.
- Genetics: Twin studies have shown that disc degeneration and herniation have a significant genetic component, estimated at 50-70% heritability. Genes affecting collagen structure, inflammatory response, and disc metabolism play a role.
- Sedentary lifestyle: Prolonged sitting increases intradiscal pressure by 40% compared to standing and reduces nutrient delivery to the avascular disc through osmotic diffusion. Office workers and truck drivers have elevated herniation risk.
- Smoking: Nicotine reduces blood flow to the already poorly vascularized disc, accelerates degeneration, and impairs healing. Smokers have a significantly higher rate of disc herniation and worse surgical outcomes.
- Repetitive bending and twisting: Occupations requiring frequent forward bending, twisting, or vibration exposure (construction, warehouse work, driving) increase cumulative disc stress.
- Prior disc injury: Once a disc has herniated, it is more susceptible to recurrent herniation. Approximately 5-15% of surgically treated herniations recur.
Symptoms and Red Flags
Typical symptoms of a herniated disc vary based on the location and severity of the herniation:
- Localized back or neck pain: Pain at the level of the herniation, often worsened by bending, sitting, coughing, or sneezing (which increase intradiscal pressure).
- Radiating pain: Sharp or burning pain following the path of the compressed nerve (sciatica in lumbar herniations, arm pain in cervical herniations).
- Numbness and tingling: In the area supplied by the affected nerve root, following a specific dermatomal pattern.
- Muscle weakness: In the muscles innervated by the compressed nerve. This may manifest as foot drop (L5), difficulty pushing off (S1), or grip weakness (C7).
- Pain worsened by certain positions: Sitting and forward bending typically worsen lumbar disc symptoms; standing and walking often provide relief.
Red Flags Requiring Immediate Medical Attention
Cauda equina syndrome is a rare but serious surgical emergency that occurs when a large disc herniation compresses the cauda equina (the bundle of nerve roots at the base of the spinal cord). Symptoms requiring immediate emergency evaluation include:
- Saddle anesthesia: Numbness in the inner thighs, buttocks, and perineal region (the area that would contact a saddle).
- Bowel or bladder dysfunction: Inability to urinate, loss of bowel control, or inability to sense when the bladder is full.
- Progressive bilateral leg weakness: Rapidly worsening weakness in both legs.
- Sexual dysfunction: Sudden onset of erectile dysfunction or loss of sensation.
Cauda equina syndrome requires emergency surgical decompression within 24-48 hours to prevent permanent neurological damage. If you experience these symptoms, seek immediate emergency medical care.
Diagnosis
Diagnosis of a herniated disc involves clinical evaluation and, when indicated, advanced imaging:
- Physical examination: Includes a neurological exam assessing sensation, reflexes, and muscle strength. Provocative tests such as the straight leg raise (Lasegue's test) can reproduce sciatic pain by stretching the affected nerve root. A positive test at 30-70 degrees of hip flexion is highly suggestive of lumbar disc herniation.
- MRI (Magnetic Resonance Imaging): The gold standard for visualizing disc herniations, as it provides excellent soft tissue contrast without radiation. MRI can identify the size, location, and type of herniation and assess nerve root compression. Important note: MRI findings must be correlated with clinical symptoms, as studies show that 30-40% of asymptomatic adults have disc herniations on MRI.
- CT scan: Provides excellent bony detail and can identify herniations, though with less soft tissue contrast than MRI. CT myelography (CT performed after contrast injection into the spinal canal) is used when MRI is contraindicated.
- Electromyography (EMG) and nerve conduction studies: Can help identify which nerve root is affected and assess the severity of nerve damage. Particularly useful when clinical findings and imaging are discordant.
Conventional Treatments
Physical Therapy
The first-line treatment for most disc herniations. A physical therapist uses a combination of manual therapy, directional preference exercises (such as the McKenzie method), core stabilization training, and nerve mobilization techniques. Multiple high-quality studies demonstrate that physical therapy outcomes are comparable to surgery for most herniations at 1-2 year follow-up.
Epidural Steroid Injections
Corticosteroids injected into the epidural space around the compressed nerve root can reduce inflammation and provide significant pain relief. Performed under fluoroscopic guidance for accuracy, epidural injections can provide weeks to months of relief and serve as a bridge to allow participation in physical therapy. Typically limited to 3 injections per year due to potential systemic effects of corticosteroids.
Surgical Options
Surgery is typically reserved for patients who fail 6-12 weeks of conservative treatment or who have progressive neurological deficits:
- Microdiscectomy: The gold standard surgical procedure for lumbar disc herniation. Through a small incision (1-2 inches), the surgeon removes the herniated portion of the disc that is compressing the nerve root while preserving the remainder of the disc. Success rates are approximately 85-90%, with most patients experiencing rapid relief of leg pain. Recovery time is typically 4-6 weeks.
- Anterior cervical discectomy and fusion (ACDF): The standard surgical approach for cervical disc herniation. The disc is accessed through a small incision in the front of the neck, the herniated material is removed, and the adjacent vertebrae are fused together with a bone graft and plate.
- Artificial disc replacement: An alternative to fusion for select cervical and lumbar herniations. The damaged disc is replaced with an artificial device that preserves motion at the treated level.
Natural and Naturopathic Approaches
A naturopathic approach to herniated disc management focuses on reducing inflammation through natural pathways, supporting nerve healing, and creating optimal conditions for the body to reabsorb the herniated material:
Anti-Inflammatory Diet
An anti-inflammatory eating pattern is foundational. Emphasize omega-3-rich fish (salmon, sardines, mackerel), colorful vegetables and berries (rich in polyphenols and anthocyanins), olive oil, nuts, seeds, and anti-inflammatory spices (turmeric, ginger). Minimize refined sugars, processed foods, seed oils high in omega-6, and alcohol, all of which promote inflammatory pathways.
Omega-3 Fatty Acids
High-dose fish oil (3-4 grams daily of combined EPA and DHA) provides potent anti-inflammatory effects comparable to NSAIDs in some studies. EPA and DHA are converted to resolvins and protectins that actively resolve inflammation without suppressing tissue healing. Several clinical trials have demonstrated that omega-3 supplementation can reduce discogenic pain.
Turmeric and Curcumin
Curcumin inhibits NF-kB (a master inflammatory transcription factor), COX-2, and inflammatory cytokines including TNF-alpha and IL-6, all of which are elevated in disc herniation. Use a bioavailable form (500-1000 mg curcuminoids daily with piperine or as a phospholipid complex). Research suggests curcumin may also inhibit disc degeneration at the cellular level.
Proteolytic Enzymes
Systemic enzyme therapy using serrapeptase (120,000-240,000 SPU daily) or bromelain (2000-4000 GDU daily) taken on an empty stomach can help break down fibrin and inflammatory debris around the herniation site. Proteolytic enzymes may reduce edema and improve circulation to the compressed nerve root. The enzyme chymopapain (from papaya) was historically injected directly into herniated discs to dissolve the nucleus pulposus, demonstrating the principle of enzymatic disc resorption.
Magnesium
Magnesium (400-600 mg daily as glycinate or malate) helps relax the paraspinal muscle spasms that commonly accompany disc herniation. Muscle guarding and spasm can perpetuate pain and limit mobility. Magnesium also has mild analgesic properties and supports nerve function.
B Vitamins for Nerve Healing
B vitamins are essential for nerve repair and myelin maintenance:
- Vitamin B12 (methylcobalamin): Critical for nerve regeneration and myelin sheath repair. Methylcobalamin (the active form) at 1000-5000 mcg daily supports nerve healing. Studies show improved pain and neurological recovery with B12 supplementation in radiculopathy.
- Vitamin B6 (pyridoxal-5-phosphate): Supports neurotransmitter synthesis and nerve function. Dosing of 50-100 mg daily. Do not exceed 200 mg daily due to risk of peripheral neuropathy with chronic high-dose use.
- Vitamin B1 (benfotiamine): A fat-soluble form of thiamine with superior bioavailability that supports nerve energy metabolism and has demonstrated neuroprotective effects at 300-600 mg daily.
- Methylfolate (5-MTHF): Supports methylation pathways involved in nerve repair. Particularly important for individuals with MTHFR polymorphisms who cannot efficiently convert folic acid to its active form.
Spinal Decompression
Non-surgical spinal decompression therapy uses a motorized traction table to gently stretch the spine, creating negative intradiscal pressure that may help retract herniated disc material and promote nutrient flow into the disc:
- Mechanism: By creating controlled distraction forces, decompression therapy generates negative pressure within the disc (up to -150 mmHg in some protocols). This vacuum effect may draw the herniated nucleus pulposus back toward the center of the disc and facilitate the influx of oxygen, water, and nutrients needed for healing.
- Protocol: Typical treatment involves 15-30 sessions over 4-8 weeks, with each session lasting 20-45 minutes. The traction force is applied cyclically (alternating between distraction and partial relaxation) to prevent muscle guarding.
- Evidence: While some clinical trials have shown benefit, the evidence base is mixed. Spinal decompression may be most effective for contained herniations (protrusions) rather than extruded or sequestered fragments.
- Inversion therapy: A simpler at-home approach using an inversion table to partially reverse gravitational compression on the spine. Using a 60-degree angle for 3-5 minutes, 2-3 times daily, may provide mild decompressive benefit. Full inversion is not necessary and is contraindicated in patients with hypertension, glaucoma, or cardiovascular disease.
Exercise and Rehabilitation
McKenzie Method (Mechanical Diagnosis and Therapy)
The McKenzie method is one of the most well-studied and effective exercise approaches for disc herniation. It is based on the principle of directional preference: specific spinal movements that reduce or centralize symptoms:
- Extension exercises: For most posterior disc herniations, repeated lumbar extension (press-ups, prone lying) helps push the nucleus pulposus anteriorly, away from the nerve root. The hallmark of a positive response is "centralization" of pain, meaning radiating leg pain retreats toward the spine.
- Progression: Exercises are progressed from prone lying, to prone press-ups, to standing extension, based on symptom response.
- Self-treatment: A key advantage is that once the directional preference is identified, patients can perform exercises independently throughout the day to manage symptoms.
Core Strengthening
A strong, stable core protects the lumbar spine from excessive loading and recurrent injury:
- Transversus abdominis activation: The deepest abdominal muscle that acts as a natural corset. Isolated training through "drawing in" exercises creates a protective cylinder of support around the lumbar spine.
- Multifidus strengthening: The deep spinal stabilizer muscles that atrophy rapidly after disc herniation. Bird-dog exercises and quadruped arm/leg lifts target these muscles specifically.
- Plank progressions: Gradual progression from modified planks to full planks builds endurance in the entire core stabilizing system. McGill's "Big Three" exercises (curl-up, side bridge, bird-dog) provide a safe and effective core program for disc patients.
- Avoid exercises that increase intradiscal pressure: Traditional sit-ups, crunches, and straight-leg raises significantly load the lumbar disc and should be avoided during recovery.
Complementary Therapies
Chiropractic Care
Spinal manipulation and mobilization performed by a qualified chiropractor can improve spinal mechanics, reduce muscle spasm, and decrease pain. Flexion-distraction technique is a specific chiropractic approach designed for disc herniations that uses a specialized table to gently decompress the affected segment. Studies support the safety and efficacy of chiropractic care for lumbar disc herniation when performed by experienced practitioners using appropriate techniques.
Acupuncture
Traditional Chinese acupuncture and electroacupuncture have demonstrated efficacy for disc-related pain in multiple clinical trials. Acupuncture stimulates the release of endogenous opioids (endorphins, enkephalins), modulates the descending pain inhibition system, reduces local inflammation, and relaxes paraspinal muscle spasm. A typical treatment course involves 2 sessions per week for 6-8 weeks. Points commonly used include BL23, BL25, BL40, GB30, and GB34 for lumbar herniations.
Massage Therapy
Therapeutic massage reduces paraspinal muscle tension and spasm, improves local blood flow, and can decrease pain through gate control theory mechanisms. Techniques such as myofascial release, trigger point therapy, and neuromuscular therapy can address the secondary muscle tension and guarding that accompany disc herniation.
Important Cautions
- Cauda equina syndrome is a surgical emergency. If you experience saddle numbness, loss of bowel or bladder control, or progressive bilateral leg weakness, seek emergency medical care immediately. Delay in surgical decompression can result in permanent neurological damage.
- Progressive neurological deficit (worsening weakness or numbness despite conservative treatment) should prompt urgent surgical consultation, as prolonged nerve compression can cause irreversible damage.
- Do not attempt aggressive spinal manipulation on an acute disc herniation. High-velocity rotational manipulation is contraindicated and may worsen the herniation. Only gentle, directional techniques performed by qualified practitioners should be used.
- Avoid prolonged bed rest. While short-term rest (1-2 days) may be necessary for severe acute pain, extended bed rest leads to deconditioning, muscle atrophy, bone loss, and worse long-term outcomes. Early, gentle movement is strongly recommended.
- MRI findings must be correlated with symptoms. Many disc herniations visible on MRI are asymptomatic. Surgery should only be considered when imaging findings match the clinical presentation, and conservative measures have been given adequate time.
- Proteolytic enzymes and omega-3 fatty acids have mild blood-thinning effects. Discontinue before any surgical procedures and use with caution if taking anticoagulant medications.
- Inversion therapy is contraindicated for individuals with uncontrolled hypertension, glaucoma, retinal detachment, cardiovascular disease, pregnancy, or recent stroke.
- Do not exceed 200 mg daily of vitamin B6 for prolonged periods, as chronic high-dose use can paradoxically cause peripheral neuropathy.
- Consult a qualified healthcare provider before beginning any new supplement or exercise regimen, especially if you have a diagnosed disc herniation with neurological symptoms.
14. References & Research
Historical Background
The concept of disc herniation was first clearly described by Walter Dandy in 1929 and independently by William Jason Mixter and Joseph Barr in their landmark 1934 paper, which established that ruptured intervertebral discs were a primary cause of sciatica. Their work at Massachusetts General Hospital fundamentally changed the understanding and surgical treatment of back pain. Robin McKenzie developed his mechanical diagnosis and therapy method in 1981.
Key Research Papers
- Mixter WJ, Barr JS. Rupture of the intervertebral disc with involvement of the spinal canal. New England Journal of Medicine. 1934;211(5):210-215.
- Weinstein JN, et al. Surgical vs nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT). JAMA. 2006;296(20):2441-2450.
- Jensen MC, et al. Magnetic resonance imaging of the lumbar spine in people without back pain. New England Journal of Medicine. 1994;331(2):69-73.
- Peul WC, et al. Surgery versus prolonged conservative treatment for sciatica. New England Journal of Medicine. 2007;356(22):2245-2256.
- Saal JA, Saal JS. Nonoperative treatment of herniated lumbar intervertebral disc with radiculopathy: an outcome study. Spine. 1989;14(4):431-437.
- Komori H, et al. The natural history of herniated nucleus pulposus with radiculopathy. Spine. 1996;21(2):225-229.
- Lurie JD, et al. Surgical versus nonoperative treatment for lumbar disc herniation: eight-year results for the SPORT. Spine. 2014;39(1):3-16.
- Atlas SJ, et al. Long-term outcomes of surgical and nonsurgical management of sciatica secondary to a lumbar disc herniation: 10 year results from the Maine Lumbar Spine Study. Spine. 2005;30(8):927-935.
- Battie MC, et al. The role of spinal flexibility in back pain: the Twin Spine Study. Spine. 1995;20(24):2731-2737.
- McGill SM. Low back stability: from formal description to issues for performance and rehabilitation. Exercise and Sport Sciences Reviews. 2001;29(1):26-31.
- Chou R, et al. Diagnosis and treatment of low back pain: a joint clinical practice guideline. Annals of Internal Medicine. 2007;147(7):478-491.
- Kreiner DS, et al. An evidence-based clinical guideline for the diagnosis and treatment of lumbar disc herniation with radiculopathy. The Spine Journal. 2014;14(1):180-191.
Research Papers
- Clinical trials on herniated disc — PubMed search
- Systematic reviews of herniated disc — PubMed search
- Meta-analyses on herniated disc — PubMed search
- Treatment research on herniated disc — PubMed search
- Mechanism studies of herniated disc — PubMed search
- Epidemiology of herniated disc — PubMed search
Connections
- Sciatica
- Magnesium
- Turmeric
- Collagen
- Anti-Inflammatory Diet
- Tendinitis
- Carpal Tunnel Syndrome
- Full Body MRI
- Peripheral Neuropathy
- Omega-3 Fatty Acids
- Vitamin B6
- Numbness and Tingling
- Fibromyalgia
- Chronic Pain
- Obesity
- Osteoarthritis
- Low Back Pain