Dizziness and Vertigo
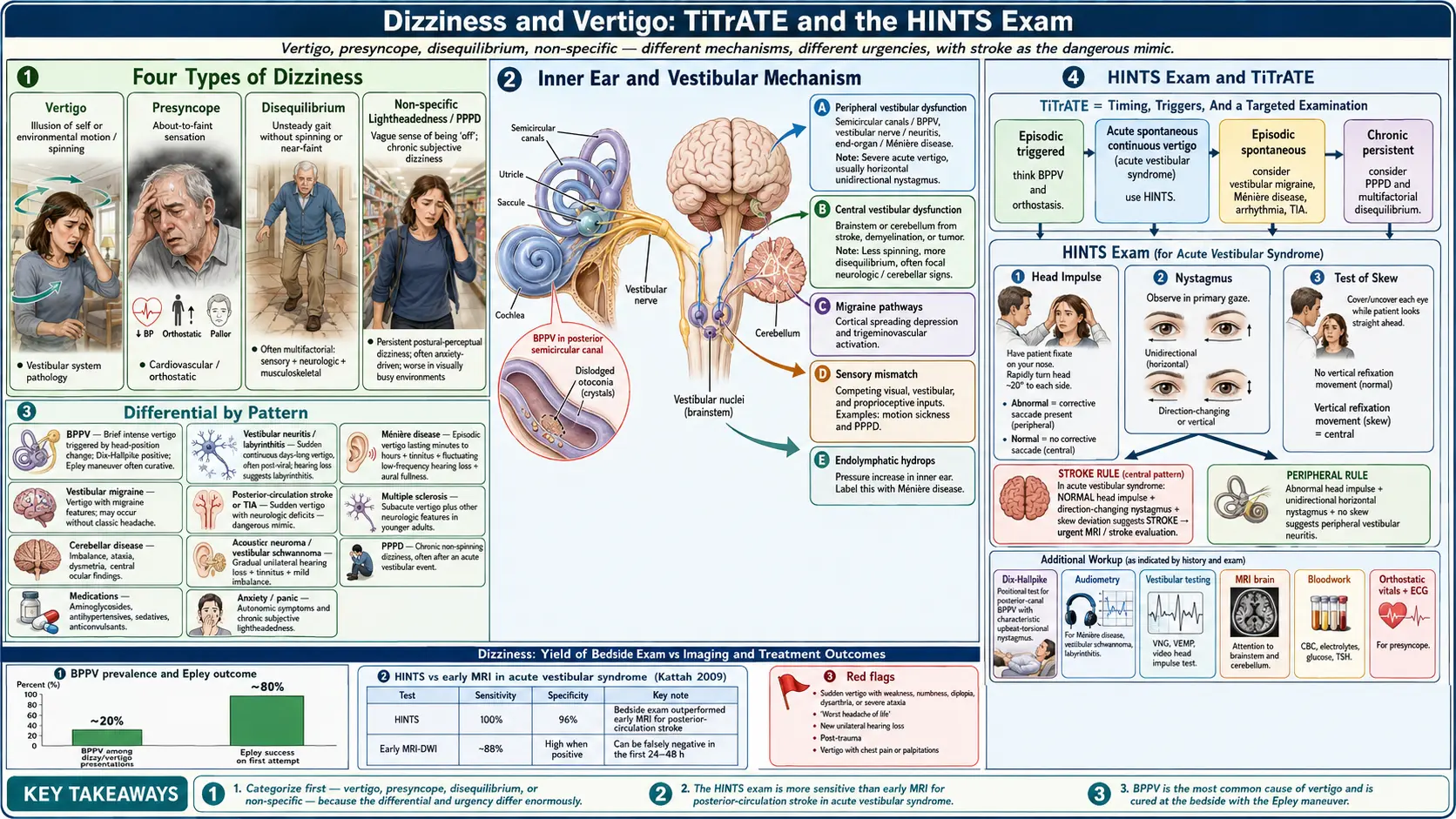


Table of Contents
- Overview
- Types of Dizziness
- Common Causes
- Mechanisms
- Evaluation
- Management
- When to Seek Medical Care
- Connections
- References & Research
- Featured Videos
Overview
Dizziness is one of the most over-used symptom words in medicine. The same complaint can mean true vertigo (illusion of motion), presyncope (about to faint), disequilibrium (unsteady gait), or a non-specific lightheadedness. The first task in any dizziness workup is to figure out which of these the patient means, because the differential diagnosis — and the urgency — differ enormously. Most acute dizziness is benign (BPPV, vestibular neuritis, vestibular migraine), but a small fraction signals posterior-circulation stroke and requires urgent imaging.
Types of Dizziness
- Vertigo — the illusion of self- or environmental motion (spinning, tilting). Suggests vestibular system pathology.
- Presyncope — the sense of being about to faint, often with greying vision and sweating. See Lightheadedness on Standing.
- Disequilibrium — unsteadiness on standing or walking, without spinning or near-fainting. Often multifactorial in older adults (sensory + neurologic + musculoskeletal).
- Non-specific lightheadedness — a vague sense of being "off," often anxiety-driven; chronic subjective dizziness / persistent postural-perceptual dizziness (PPPD) is the formal diagnosis.
Common Causes
- Benign paroxysmal positional vertigo (BPPV) — brief intense vertigo with head position changes; the most common cause of vertigo. Caused by dislodged otoconia in the semicircular canals; treated with the Epley maneuver.
- Vestibular neuritis and labyrinthitis — sudden continuous vertigo lasting days, often after a viral illness; with hearing loss in labyrinthitis.
- Meniere's disease — episodic vertigo (minutes to hours), tinnitus, fluctuating low-frequency hearing loss, ear fullness.
- Vestibular migraine — vertigo with migraine features; often without classic headache.
- Posterior-circulation stroke or TIA — sudden vertigo with neurologic deficits; the dangerous mimicker of vestibular neuritis. The HINTS exam helps separate them.
- Multiple sclerosis — sub-acute vertigo with other neurologic features in young adults.
- Cerebellar disease — tumor, hemorrhage, demyelination, degeneration.
- Acoustic neuroma (vestibular schwannoma) — gradual unilateral hearing loss, tinnitus, mild imbalance.
- Persistent postural-perceptual dizziness (PPPD) — chronic non-spinning dizziness, often after an acute vestibular event; worse with motion and visually busy environments.
- Medications — aminoglycosides (vestibulotoxic), antihypertensives, sedatives, anticonvulsants.
- Cervicogenic dizziness — from cervical spine dysfunction; controversial but recognized.
- Anxiety and panic — common cause of chronic non-specific dizziness; often coexists with other vestibular disorders.
Mechanisms
- Peripheral vestibular dysfunction — semicircular canals (BPPV), vestibular nerve (neuritis), or end-organ (Meniere's). Tends to cause severe acute vertigo with horizontal nystagmus.
- Central vestibular dysfunction — brainstem or cerebellum (stroke, demyelination, tumor). Often less spinning and more disequilibrium, plus cranial-nerve or cerebellar signs.
- Migraine pathways — vestibular migraine involves cortical spreading depression and trigeminovascular activation in vestibular pathways.
- Sensory mismatch — competing visual, vestibular, and proprioceptive inputs produce dizziness in motion sickness, virtual environments, and PPPD.
- Endolymphatic hydrops — pressure increase in the inner ear underlies Meniere's symptoms.
Evaluation
- Categorize — vertigo, presyncope, disequilibrium, or non-specific.
- Timing and triggers (TiTrATE) — episodic vs continuous; positional vs spontaneous. This drives the differential more than the descriptor.
- HINTS exam — head impulse, nystagmus, test of skew. In acute vestibular syndrome, a normal head impulse, direction-changing nystagmus, or skew deviation suggests stroke and warrants MRI.
- Dix-Hallpike maneuver — positional test for posterior-canal BPPV.
- Audiometry — for suspected Meniere's, acoustic neuroma, labyrinthitis.
- Vestibular testing (VNG, VEMP, video head-impulse test) — for chronic or atypical cases.
- MRI brain with attention to brainstem and cerebellum — for central signs, atypical features, or first attack with unilateral hearing loss.
- Bloodwork — CBC, electrolytes, glucose, TSH; targeted infectious or autoimmune testing if indicated.
- Cardiovascular evaluation — if presyncope is the dominant feature; orthostatic vitals, ECG.
Management
- BPPV — canalith repositioning maneuvers (Epley, Semont); home maneuvers for recurrence; usually no medication needed.
- Vestibular neuritis — short course of vestibular suppressants (meclizine, dimenhydrinate) for 2–3 days, then early vestibular rehabilitation.
- Meniere's disease — low-salt diet, diuretics, betahistine (in some countries), intratympanic corticosteroids or gentamicin, surgery for refractory cases.
- Vestibular migraine — migraine prevention and acute treatment; trigger avoidance.
- PPPD — SSRIs / SNRIs, vestibular rehabilitation, cognitive-behavioral therapy.
- Vestibular rehabilitation therapy — habituation, gaze stabilization, and balance training; effective in most chronic vestibular disorders.
- Treat central causes — stroke pathway for posterior-circulation stroke; immunomodulation for MS; surgery or radiation for tumors.
- Avoid prolonged vestibular suppressants — they delay central compensation in chronic disease.
When to Seek Medical Care
- Sudden vertigo with weakness, numbness, double vision, dysarthria, dysphagia, or imbalance preventing standing — call 911 for possible posterior-circulation stroke.
- Severe headache with new vertigo, especially "worst headache of life."
- New unilateral hearing loss with vertigo.
- Vertigo after head trauma.
- Recurrent or persistent vertigo affecting daily function.
- Vertigo with chest pain, palpitations, or near-fainting (consider cardiac).
- Progressive disequilibrium with cognitive change.
Connections
- Lightheadedness
- Multiple Sclerosis
- Headache
- Stroke
- Migraine
- Tinnitus
- Vertigo / Menière's Disease
- Numbness & Tingling
- POTS
- Vestibular Migraine
- Anxiety
- Depression
- Chest Pain
- Magnesium
- Nausea Vomiting
- Acesulfame Potassium
- Epilepsy
- Ginkgo Biloba
References & Research
Historical Background
Robert Bárány earned the 1914 Nobel Prize for caloric testing and the physiology of the vestibular system. The 1980 Epley maneuver transformed BPPV from a chronic burden into a 5-minute office cure. The HINTS exam (Kattah, 2009) gave clinicians a bedside tool with sensitivity exceeding early MRI for posterior-circulation stroke. Vestibular migraine was formally codified in 2012 by the Bárány Society and the International Headache Society.
Key Research Papers
- Kattah JC, Talkad AV, Wang DZ, Hsieh YH, Newman-Toker DE. HINTS to diagnose stroke in the acute vestibular syndrome: three-step bedside oculomotor examination more sensitive than early MRI diffusion-weighted imaging. Stroke. 2009;40(11):3504-3510.
- Furman JM, Cass SP. Benign paroxysmal positional vertigo. New England Journal of Medicine. 1999;341(21):1590-1596.
- Bhattacharyya N, Gubbels SP, Schwartz SR, et al. Clinical practice guideline: benign paroxysmal positional vertigo (update). Otolaryngology — Head and Neck Surgery. 2017;156(3 Suppl):S1-S47.
- Lempert T, Olesen J, Furman J, et al. Vestibular migraine: diagnostic criteria. Journal of Vestibular Research. 2012;22(4):167-172.
- Staab JP, Eckhardt-Henn A, Horii A, et al. Diagnostic criteria for persistent postural-perceptual dizziness (PPPD). Journal of Vestibular Research. 2017;27(4):191-208.
- Sajjadi H, Paparella MM. Meniere's disease. The Lancet. 2008;372(9636):406-414.
- Hain TC. Treatment of vertigo. Mayo Clinic Proceedings. 2003;78(11):1399-1409.
- Newman-Toker DE, Edlow JA. TiTrATE: a novel approach to diagnosing acute dizziness and vertigo. Neurologic Clinics. 2015;33(3):577-599.
- McDonnell MN, Hillier SL. Vestibular rehabilitation for unilateral peripheral vestibular dysfunction. Cochrane Database of Systematic Reviews. 2015;(1):CD005397.
- Kim JS, Zee DS. Benign paroxysmal positional vertigo. New England Journal of Medicine. 2014;370(12):1138-1147.
PubMed Topic Searches
- BPPV and the Epley maneuver
- HINTS exam for vestibular stroke
- Meniere's disease treatment
- Vestibular migraine
- Persistent postural-perceptual dizziness (PPPD)
- Vestibular rehabilitation