Low Testosterone and Testosterone Replacement Therapy (TRT): What Men Should Know
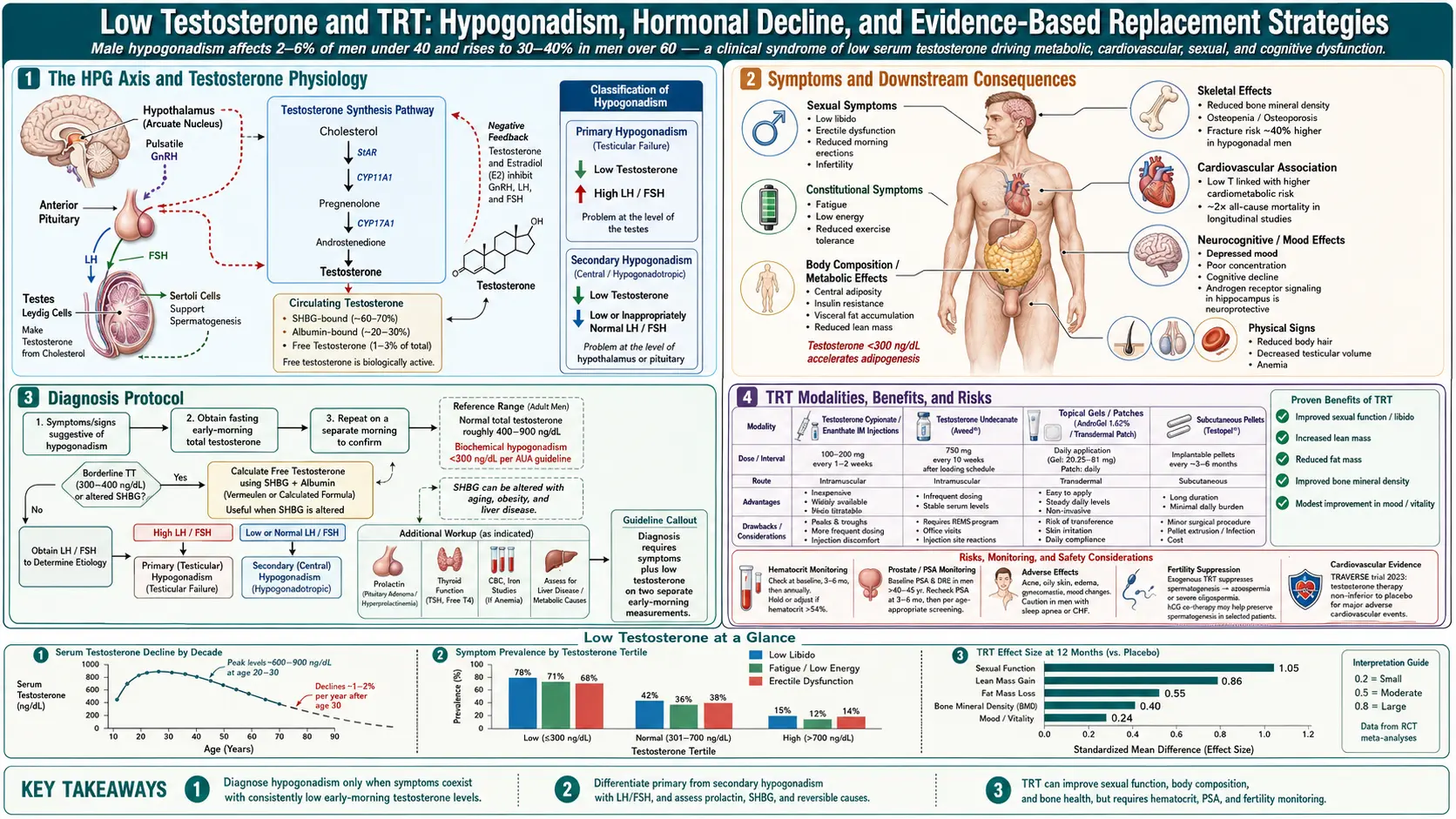
Low testosterone (also called hypogonadism, low T, or androgen deficiency) is a clinical syndrome defined by consistently low serum testosterone along with characteristic symptoms. Testosterone declines slowly and naturally with age — roughly 1% per year after age 30 — but the subset of men who develop truly symptomatic deficiency can benefit significantly from testosterone replacement therapy (TRT) when appropriately prescribed and monitored. At the same time, over-the-counter “low-T” marketing has inflated diagnosis rates beyond the population that benefits, and long-term cardiovascular and prostate safety has been extensively debated.
This article covers clinical diagnosis, the appropriate lab workup, evidence-based treatment options, monitoring, and who should approach TRT cautiously or avoid it.
Table of Contents
- What Low Testosterone Is
- Symptoms That Matter
- Causes of Low T
- Making the Diagnosis
- Forms of TRT
- Benefits of TRT
- Risks and Monitoring
- Fertility Considerations
- Alternatives to TRT
- Lifestyle Foundations
- Research Papers
- Connections
- Featured Videos
What Low Testosterone Is
Testosterone is the principal androgen in men, produced primarily in the testicular Leydig cells under the pituitary’s LH drive and the hypothalamus’s GnRH signal. It supports libido, erectile function, spermatogenesis, muscle mass, bone density, red blood cell production, mood, and cognitive function. The clinical syndrome of low testosterone requires both consistently low morning total testosterone (below the laboratory reference range on at least two early-morning, fasting measurements) and characteristic symptoms. Either alone is insufficient.
Symptoms That Matter
- Reduced libido and sexual thoughts
- Decreased spontaneous morning erections
- Erectile dysfunction
- Fatigue and reduced vigor
- Loss of muscle mass and strength
- Increased body fat, particularly visceral
- Depressed mood
- Poor concentration
- Hot flashes or sweats (in severe deficiency)
- Anemia
- Reduced body hair and beard growth over time
Causes of Low T
Causes fall into two anatomical categories:
- Primary hypogonadism — testicular failure. LH rises. Causes: Klinefelter syndrome, prior chemotherapy or radiation, mumps orchitis, trauma, aging.
- Secondary hypogonadism — pituitary or hypothalamic cause. LH is low or normal. Causes: pituitary tumor, infiltrative disease, obstructive sleep apnea, opioid use, glucocorticoid use, severe obesity, hemochromatosis, anabolic-steroid suppression.
Making the Diagnosis
- Two early-morning (7–10 AM), fasting total testosterone measurements — levels pulse diurnally; evening measurements are unreliable.
- Free testosterone, SHBG when total is borderline or SHBG is expected to be abnormal.
- LH, FSH, prolactin to distinguish primary vs secondary.
- Estradiol, PSA, hematocrit, lipid panel, ferritin, fasting glucose, A1c as part of baseline work-up.
- Pituitary MRI if secondary hypogonadism without explanation, particularly with very low testosterone or hyperprolactinemia.
Forms of TRT
- Intramuscular injections — testosterone cypionate or enanthate, typically every 7–14 days; cheapest and widely used.
- Subcutaneous injections — smaller volume, more physiologic steady state, twice weekly.
- Transdermal gels — daily application to shoulders, upper arms, or thighs; risk of transfer to partners or children.
- Transdermal patches — less commonly used due to skin reactions.
- Long-acting pellets — implanted every 3–6 months.
- Nasal gel (Natesto) — three times daily; preserves fertility better because it avoids full suppression of the HPG axis.
- Oral (Jatenzo, Tlando, Kyzatrex) — testosterone undecanoate; requires twice-daily dosing with fatty meals; hepatic safety improved over older 17-alpha-alkylated oral androgens.
Benefits of TRT
In men with confirmed deficiency, TRT has been shown to:
- Improve sexual function, libido, and spontaneous erections.
- Increase lean body mass and reduce fat mass.
- Improve mood and, in some analyses, reduce depressive symptoms.
- Improve bone density.
- Correct anemia of hypogonadism.
- Modestly improve insulin sensitivity.
- Reduce fatigue and improve vitality.
The TRAVERSE trial (2023) — the largest cardiovascular safety trial of TRT to date — showed no increased risk of major adverse cardiovascular events over roughly 3 years in middle-aged and older men with hypogonadism and cardiovascular-disease risk. It did show increased risk of atrial fibrillation, pulmonary embolism, and kidney injury.
Risks and Monitoring
- Erythrocytosis. Raised hematocrit; monitor — if >54%, dose reduction, longer dosing intervals, or therapeutic phlebotomy.
- Atrial fibrillation. Modest increased risk in TRAVERSE.
- Venous thromboembolism. Small increased risk.
- Obstructive sleep apnea exacerbation.
- Suppressed spermatogenesis and infertility. TRT suppresses intratesticular testosterone and can cause reversible infertility; see below.
- Gynecomastia from aromatization to estradiol; manage by estradiol monitoring, dose adjustment, or aromatase inhibitor if severe.
- Prostate monitoring. Regular PSA and digital rectal examination. TRT does not cause prostate cancer but can exacerbate known disease.
- Skin reactions from gels or patches.
Fertility Considerations
Exogenous testosterone suppresses pituitary LH and FSH, shutting down intratesticular testosterone (which is 100-fold higher than serum) and suppressing sperm production — often to azoospermia. Men who wish to preserve fertility while on treatment can use clomiphene citrate or enclomiphene (selective estrogen receptor modulators that raise endogenous testosterone production through the hypothalamic-pituitary-gonadal axis), hCG added to TRT to maintain intratesticular testosterone, or the intranasal testosterone formulation which minimally suppresses the HPG axis. Fertility return after TRT cessation averages 6–12 months but is not universal.
Alternatives to TRT
- Clomiphene/enclomiphene for secondary hypogonadism — preserves fertility.
- hCG monotherapy — stimulates Leydig cells directly.
- Weight loss in obese men — even modest loss raises testosterone.
- Treatment of sleep apnea.
- Opioid tapering in opioid-induced hypogonadism.
Lifestyle Foundations
- Sleep 7–9 hours. Sleep deprivation sharply lowers testosterone.
- Resistance training.
- Healthy body composition — excess adiposity aromatizes testosterone to estradiol.
- Adequate micronutrients — zinc, magnesium, vitamin D; deficiency impairs testosterone production.
- Moderate alcohol.
- Stress management — chronic cortisol elevation suppresses GnRH.
Research Papers
- Clinical trials on testosterone replacement therapy — PubMed search
- TRAVERSE trial and cardiovascular safety of TRT — PubMed search
- Clomiphene / enclomiphene for secondary hypogonadism — PubMed search
- Testosterone therapy and prostate cancer risk — PubMed search
- TRT-induced erythrocytosis — PubMed search
- Weight loss and endogenous testosterone — PubMed search
- hCG for fertility preservation in TRT — PubMed search
- Testosterone and bone mineral density — PubMed search
Connections
- Erectile Dysfunction
- Testosterone Test
- Zinc
- Obstructive Sleep Apnea
- Magnesium
- Obesity
- Benign Prostatic Hyperplasia
- PSA Test
- Vitamin D3
- Hormone Panel
- Fasting
- Anemia
- Infertility
- Prostate Conditions
- Saw Palmetto
- Prostate Cancer