Methylene Blue Drug Interactions and Serotonin Syndrome: The Critical Safety List
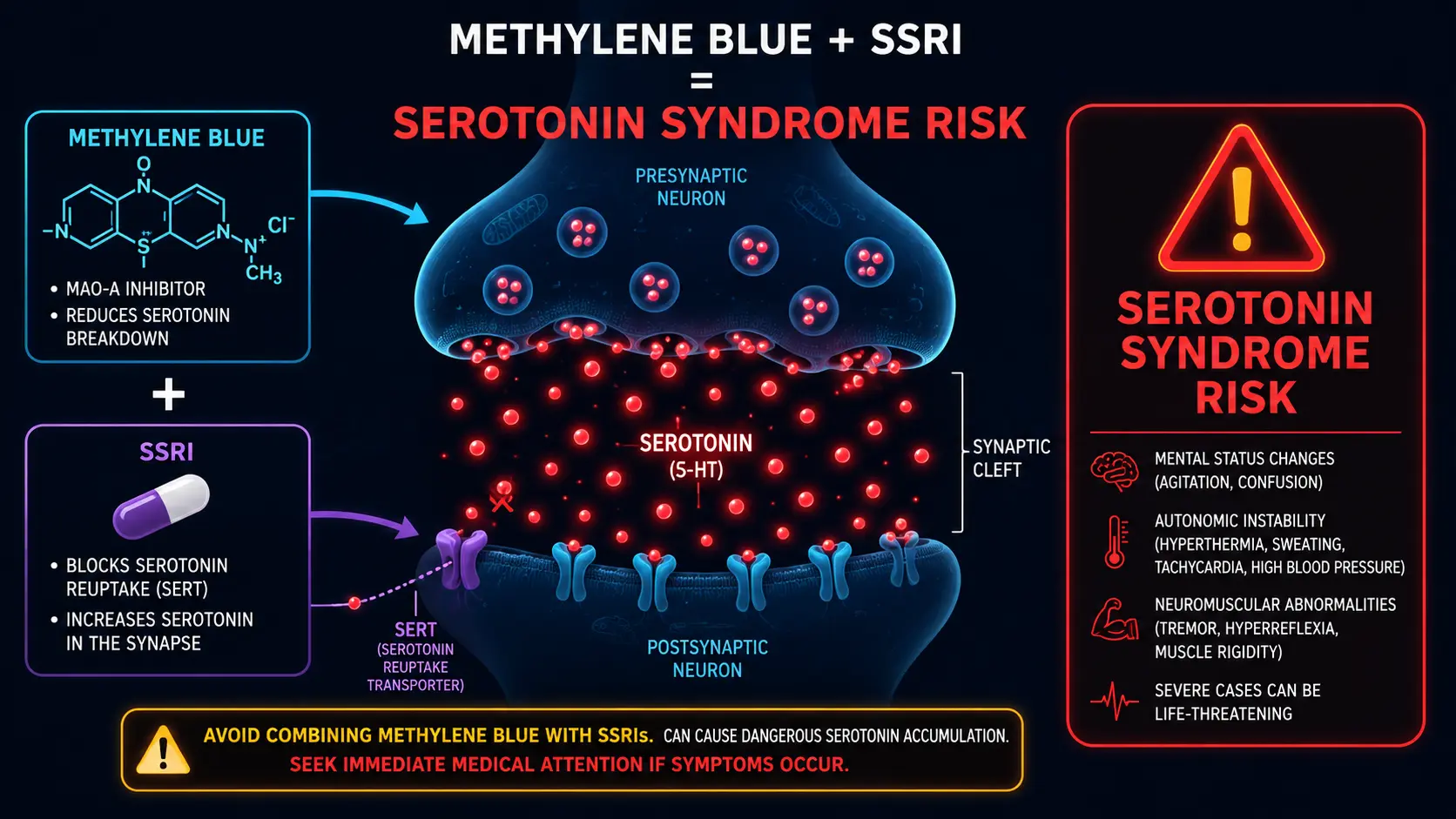
This is the most important safety topic in methylene blue therapy. Methylene blue is a potent reversible inhibitor of monoamine oxidase A (MAO-A) at clinically relevant concentrations. Combining methylene blue with serotonergic medications can precipitate serotonin syndrome — a potentially life-threatening condition characterized by altered mental status, autonomic hyperactivity, and neuromuscular abnormalities. The FDA issued a black-box warning on parenteral methylene blue specifically because of cases that occurred during routine use.
This page lists the medication classes that interact, the timing required for safe washout, the clinical features of serotonin syndrome, and the practical consequences for anyone considering methylene blue at therapeutic doses.
Table of Contents
- The MAO-A Inhibition Mechanism
- The FDA Black-Box Warning
- Absolute Contraindications
- Major Drug Interactions
- Washout Periods
- Recognizing Serotonin Syndrome
- Emergency Management
- Supplements and Foods to Watch
- Low-Dose Considerations
- Research Papers and References
- Connections
- Featured Videos
The MAO-A Inhibition Mechanism
Monoamine oxidase A (MAO-A) is the enzyme that breaks down serotonin, norepinephrine, and dopamine in the synaptic cleft. By inhibiting MAO-A, methylene blue allows these neurotransmitters to accumulate. In a healthy person without other serotonergic input, this produces a mild mood-elevation and energy effect, contributing to the nootropic profile.
The danger arises when MAO-A inhibition is combined with another drug that increases serotonin — either by blocking reuptake (SSRIs, SNRIs), by stimulating release (amphetamines, MDMA), or by providing the precursor (5-HTP, tryptophan). The result is excessive serotonin signaling at multiple sites: 5-HT1A receptors (autonomic), 5-HT2A (cortical excitation), and 5-HT3 (gut). Severe cases progress to seizures, hyperthermia, rhabdomyolysis, disseminated intravascular coagulation, and death.
Methylene blue's MAO-A inhibition is dose-dependent. Even at nootropic doses (1–2 mg/kg), the inhibition is clinically meaningful. At therapeutic doses (1–2 mg/kg IV), it is profound — on the order of selective MAO-A inhibitors like moclobemide.
The FDA Black-Box Warning
In 2011, the FDA issued a Drug Safety Communication on methylene blue and serotonin syndrome, prompted by case reports of severe serotonin syndrome (some fatal) in patients given parenteral methylene blue while on serotonergic antidepressants. The warning specifically addresses parenteral (IV) methylene blue used for parathyroid surgery, methemoglobinemia, and ifosfamide encephalopathy — situations where the drug is given in an inpatient setting at standard doses (1–2 mg/kg).
The warning's clinical translation:
- Avoid combining methylene blue with serotonergic antidepressants whenever possible
- If methylene blue is essential, stop the serotonergic drug and observe an appropriate washout period before administration
- If acute methylene blue is unavoidable (e.g., emergency methemoglobinemia), monitor for serotonin syndrome
The warning extends in spirit to off-label oral use at therapeutic doses.
Absolute Contraindications
Do not combine therapeutic doses of methylene blue with any of the following classes:
- Selective serotonin reuptake inhibitors (SSRIs) — sertraline, escitalopram, fluoxetine, paroxetine, fluvoxamine, citalopram
- Serotonin-norepinephrine reuptake inhibitors (SNRIs) — venlafaxine, desvenlafaxine, duloxetine, milnacipran
- Tricyclic antidepressants with significant serotonergic effect — clomipramine, imipramine, amitriptyline
- MAOIs — phenelzine, tranylcypromine, isocarboxazid, selegiline (high-dose), rasagiline, moclobemide
- Other serotonergic antidepressants — vilazodone, vortioxetine, trazodone (high-dose), nefazodone
- Triptans for migraine — sumatriptan, rizatriptan, zolmitriptan, eletriptan, naratriptan, frovatriptan, almotriptan
- Tramadol — serotonergic opioid
- Fentanyl and methadone — significant serotonergic activity
- Meperidine (Demerol) — classic interaction
- Dextromethorphan (DXM, in many cough preparations)
- Linezolid — antibiotic with MAOI activity; severe risk in combination
- Buspirone
- 5-HTP, L-tryptophan, St. John's Wort — OTC supplements with significant serotonergic effect
Major Drug Interactions (Caution Even at Low Doses)
- Lithium — serotonin syndrome reported; case-by-case decision
- Bupropion (Wellbutrin) — not classically serotonergic but can lower seizure threshold; caution at higher MB doses
- Stimulant ADHD medications — amphetamines, methylphenidate; hypertensive crisis possible
- Anticonvulsants — especially valproate; multiple potential interactions
- Sympathomimetics — pseudoephedrine, phenylephrine; hypertension
- Tyramine-rich foods — aged cheeses, fermented meats, fava beans (classic MAOI dietary issue, less severe with MB but still relevant at higher doses)
- Antipsychotics — some have serotonergic effects; consult clinician
Washout Periods
Before initiating therapeutic methylene blue (above ~1 mg/kg), the serotonergic drug must be withdrawn and time allowed for clearance:
- Most SSRIs and SNRIs: 5 half-lives = 5–7 days (e.g., sertraline, escitalopram, venlafaxine)
- Fluoxetine: 5 weeks — the long half-life of norfluoxetine extends the washout dramatically
- Paroxetine: 2 weeks (short half-life but withdrawal complications)
- Tramadol, fentanyl, methadone: at least 24–48 hours after the last dose, longer if significant accumulation
- MAOIs: 14 days minimum (irreversible MAOIs require enzyme regeneration)
- 5-HTP, L-tryptophan, St. John's Wort: 3–5 days
- After methylene blue: 24 hours minimum before resuming a serotonergic medication; longer for therapeutic IV doses
Stopping antidepressants abruptly carries its own risk — depression recurrence, suicidal ideation, withdrawal symptoms. Discontinuation should be supervised by the prescribing clinician.
Recognizing Serotonin Syndrome
Serotonin syndrome typically develops within hours of the offending combination. Sterner-Hunter criteria require the presence of one of:
- Spontaneous clonus
- Inducible clonus + agitation or diaphoresis
- Ocular clonus + agitation or diaphoresis
- Tremor + hyperreflexia
- Hypertonia + temperature > 38°C + ocular or inducible clonus
Clinical features cluster into three categories:
- Mental status changes — agitation, anxiety, confusion, restlessness, hallucinations, seizures, coma
- Autonomic hyperactivity — tachycardia, hypertension, hyperthermia, diaphoresis, dilated pupils, flushing, mucous membranes wet (vs. dry in anticholinergic syndrome)
- Neuromuscular abnormalities — tremor, clonus (especially lower extremity), hyperreflexia, rigidity (lower > upper extremities), akathisia, myoclonus
The combination of lower-extremity-predominant clonus and autonomic hyperactivity shortly after starting (or increasing) a serotonergic agent is the hallmark.
Emergency Management
Suspected serotonin syndrome is a medical emergency. Outside a clinical setting:
- Discontinue any potentially causative medications immediately
- Call emergency services (911 in the US) for any altered mental status, hyperthermia, or sustained tachycardia
- Do not "ride out" the symptoms; severe cases progress rapidly to rhabdomyolysis and DIC
In hospital, supportive care includes IV fluids, benzodiazepines for agitation and clonus, active cooling for hyperthermia, and cyproheptadine (a 5-HT2A antagonist) as a specific antidote. ICU admission is typical for moderate-to-severe cases.
Supplements and Foods to Watch
Common supplements with serotonergic effect:
- St. John's Wort — significant SSRI-like activity; absolute avoid
- 5-HTP — direct serotonin precursor; avoid
- L-tryptophan — same; avoid
- SAMe — modest serotonergic; caution
- Rhodiola, Ginseng — mild MAOI activity reported; caution at higher MB doses
- Kratom — serotonergic at higher doses; avoid combination
- Yohimbine — sympathomimetic; hypertensive risk
Tyramine-rich foods (aged cheeses, soy sauce, sauerkraut, cured meats, fava beans, certain wines) can cause hypertensive episodes with MAO inhibitors. The risk with methylene blue is lower than with classic MAOIs but worth being aware of, especially at higher doses.
Low-Dose Considerations
An honest question: are interactions still relevant at microdoses (0.5 mg/kg or less)?
The published cases of MB-induced serotonin syndrome have generally involved standard or high doses (typically 1–5 mg/kg IV). At microdoses, MAO-A inhibition is partial and reversible, and the absolute risk of serotonin syndrome in an SSRI-treated patient is unclear — reports exist but are uncommon.
That said, the risk is real even if the probability is low, and the consequences are severe. The conservative position — avoid combination at any dose — is the right starting point. If a patient on a serotonergic medication is determined to use methylene blue, the conversation should happen with the prescribing clinician and ideally with the medication tapered off first.
Research Papers and References
- MB and serotonin syndrome — PubMed search
- MB and MAO-A inhibition — PubMed search
- FDA MB safety warning — PubMed search
- Sterner-Hunter criteria — PubMed search
- Cyproheptadine treatment — PubMed search
- Fluoxetine washout for MAOIs — PubMed search
External Authoritative Resources
Connections
- Methylene Blue
- Dosing Guide
- Methemoglobinemia and G6PD Deficiency
- Pharmaceutical Grade vs Industrial Dye
- Mitochondrial Mechanism and Bioenergetics
- Cognitive Enhancement and ADHD
- Methylene Blue and Long COVID
- Photodynamic Therapy and Cancer Research
- Depression
- ADHD
- Tryptophan
- Anxiety
- Natural Anxiety Relief
- Hypertension
- Longevity Protocols
- History Ehrlich Phenothiazines
Featured Videos

The Hidden DANGERS of Methylene Blue (How to Use It Safely)

Methylene Blue Benefits: Boost Brain Energy, Fight Aging & Support Mitochondria

Methylene Blue: Medicine, Poison, or Biohacker Trap?

Blue Brains? Dr. Scott Breaks Down Paul Saladino’s Methylene Blue Claims

Why I'm using Methylene Blue for my metabolism

Methylene Blue Explained — Benefits, Risks, and What Clinicians Need to Know

Methylene Blue and ADHD

94% of Adults Have Mitochondrial Dysfunction — How Methylene Blue Restores Energy | Dr. Scott Sherr

Hydroxocobalamin and Methylene Blue in Septic Shock

Methylene Blue: Why This Changes Everything For Fatigue

Methylene Blue’s Shocking Drug Interactions — What Doctors Don’t Warn You About

Methylene Blue Revealed The Memory Hack Everyone Uses

E54: Why Methylene Blue is the Ultimate Biohack for Brain and Body Optimization

Methylene Blue: Ancient Dye, Modern Nootropic?

Is Methylene Blue REALLY Worth The Hype?

Can Methylene Blue Actually Give You Serotonin Syndrome? Combining With SSRIs