ADHD (Attention-Deficit/Hyperactivity Disorder)
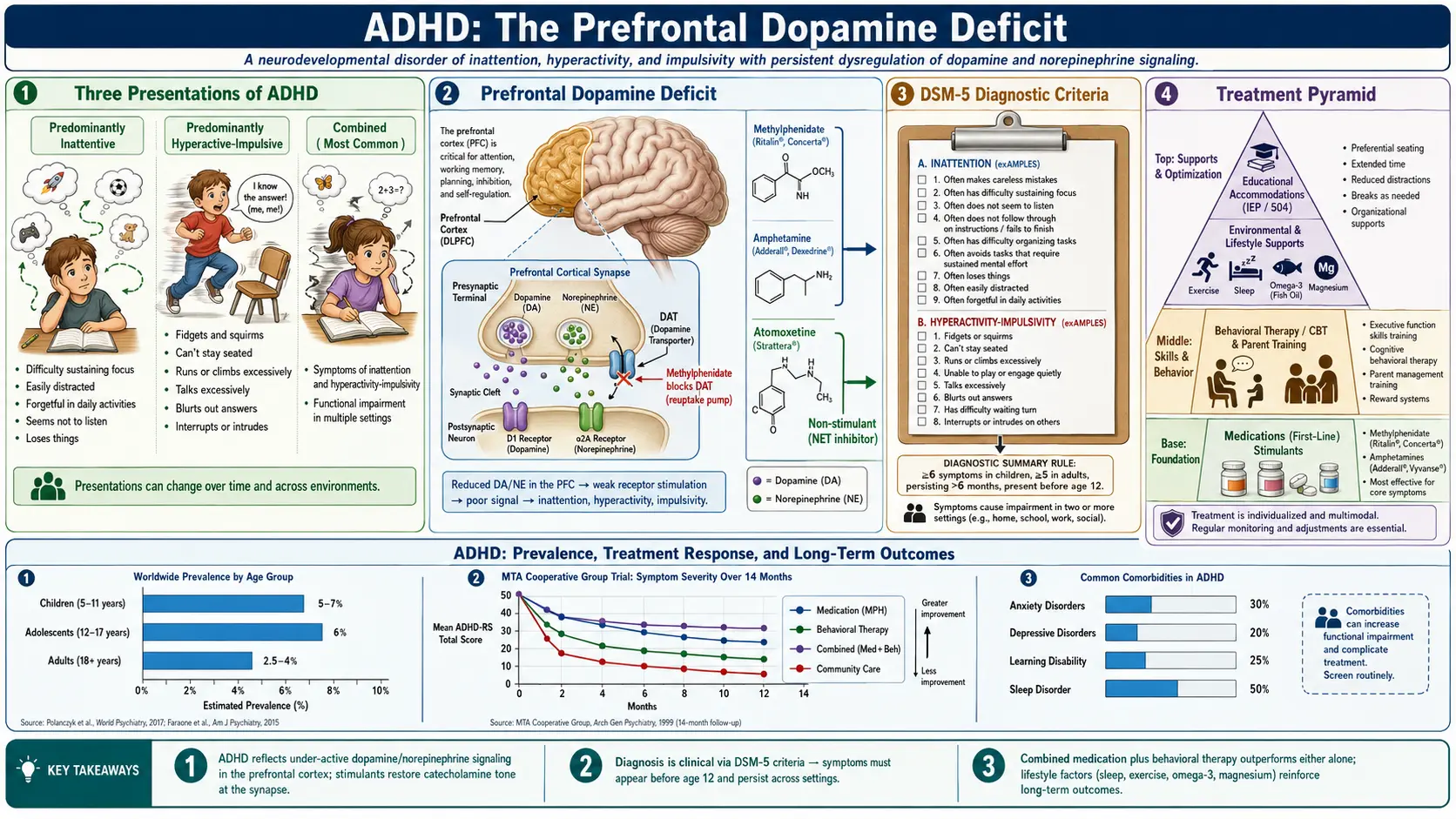
Table of Contents
- Overview
- Epidemiology
- Pathophysiology (Neurobiology)
- Etiology and Risk Factors
- DSM-5 Diagnostic Subtypes
- Clinical Presentation
- Diagnosis
- Treatment
- Comorbidities
- Complications
- Prognosis
- Research Papers and References
- Featured Videos
1. Overview
Attention-Deficit/Hyperactivity Disorder (ADHD) is the most common neurodevelopmental disorder worldwide, affecting an estimated 5–10% of children and 2.5–4% of adults. It is characterized by three core symptom domains: inattention, hyperactivity, and impulsivity — impairing functioning across school, work, relationships, and daily life. ADHD is not a character flaw or a failure of will; it is a brain-based condition with robust neurobiological and genetic foundations.
The DSM-5 (2013) reclassified ADHD from the chapter on "Disorders Usually First Diagnosed in Infancy, Childhood, or Adolescence" into the new Neurodevelopmental Disorders chapter — a critical shift that acknowledges ADHD as a lifelong condition rather than a childhood problem that children outgrow. In reality, 60–70% of those diagnosed in childhood continue to meet criteria in adulthood, and millions more carry significant residual impairment even when they no longer meet full diagnostic thresholds.
A persistent myth is that ADHD primarily affects boys and resolves by adolescence. In fact, females are systematically underdiagnosed, often presenting with the predominantly inattentive subtype — characterized by daydreaming, disorganization, and forgetfulness rather than the visible hyperactivity more commonly observed in males. Girls and women frequently develop sophisticated masking behaviors that conceal their struggles, delaying diagnosis by years or decades and allowing anxiety, depression, and low self-esteem to accumulate in the interim.
With appropriate treatment — combining behavioral strategies, environmental accommodations, and when indicated, medication — individuals with ADHD can and do thrive. ADHD is associated with many strengths when well-managed, including creativity, hyperfocus on areas of deep interest, high energy, and entrepreneurial thinking.
2. Epidemiology
ADHD is one of the most studied psychiatric conditions in children. The US prevalence among children is approximately 9.4% based on CDC data from 2016, translating to roughly 6.1 million children aged 2–17. Among US adults, the 12-month prevalence is approximately 4.4% (Kessler et al., 2006), suggesting a significant treatment gap — the majority of adults with ADHD have never been diagnosed or treated.
Globally, a landmark 2007 meta-analysis by Polanczyk et al. estimated a pooled worldwide prevalence of 5.29% in children, with a 2014 update confirming stability of rates over three decades, arguing against a true epidemic — variation in prevalence across countries largely reflects differences in diagnostic criteria and assessment methods, not true biological differences in incidence.
The male-to-female ratio in diagnosed populations is approximately 2–3:1, but population-based and genetic studies suggest the true ratio is closer to 1.5:1. The diagnostic gap reflects referral bias: hyperactive boys are more likely to be brought to clinical attention. Peak age of diagnosis is 7–10 years. Significant racial and ethnic disparities exist in diagnosis rates in the United States, with Black and Hispanic children historically underdiagnosed relative to non-Hispanic white children, a gap that reflects systemic inequities in access to diagnostic evaluation rather than true differences in prevalence.
The adult treatment gap is substantial. Only about 25% of adults who meet criteria for ADHD receive treatment. Many adults are diagnosed only after their own child receives a diagnosis, prompting retrospective recognition of lifelong symptoms. Late diagnosis — while sometimes distressing — is frequently experienced as profoundly validating.
3. Pathophysiology (Neurobiology)
Dopamine and Norepinephrine Dysregulation
The core neurobiological mechanism of ADHD involves dysfunction in catecholamine signaling — specifically, dopamine (DA) and norepinephrine (NE) — within the prefrontal cortex (PFC). The PFC governs executive functions including working memory, attention regulation, response inhibition, and cognitive flexibility. As described in the seminal catecholamine theory of ADHD developed by Amy Arnsten, optimal PFC function requires a narrow range of DA and NE stimulation — too little or too much impairs the "tuning" of PFC networks, weakening signal relative to noise. In ADHD, this balance is disrupted, impairing the PFC's ability to sustain focused attention, suppress distractions, and regulate impulses.
Genetic Associations
Twin studies estimate ADHD heritability at 70–80%, making it one of the most heritable psychiatric conditions. Key genetic associations include:
- DAT1 (SLC6A3) — the dopamine transporter gene; the 10-repeat VNTR allele has been among the most replicated findings
- DRD4 — dopamine receptor D4; the 7-repeat allele is associated with reduced dopamine signaling efficiency and is 2–3 times more common in ADHD
- DRD5 — dopamine receptor D5
- SNAP25 — synaptosomal-associated protein, involved in dopamine and norepinephrine vesicle release
- LPHN3 (ADGRL3) — latrophilin 3, a recently identified susceptibility gene
ADHD has a polygenic architecture; no single gene accounts for more than a small fraction of risk. Rare copy number variants (CNVs) including deletions at 22q11.2 and 16p13.11 are enriched in ADHD.
Executive Function Deficits
Neuropsychological research identifies consistent deficits in:
- Working memory — holding and manipulating information in mind over short periods
- Response inhibition — suppressing prepotent but inappropriate responses
- Cognitive flexibility — shifting attention and mental set between tasks
- Time perception and prospective memory — estimating elapsed time, remembering future intentions ("time blindness")
- Emotional regulation — modulating emotional responses, particularly frustration and disappointment
Neuroimaging Findings
The landmark Shaw et al. (2007) PNAS study using longitudinal MRI in 446 children demonstrated that ADHD is characterized by a 3–5 year delay in cortical maturation — most significantly in prefrontal regions — rather than a fixed structural deficit. This finding reframes ADHD as a developmental lag rather than a static brain difference, consistent with the clinical observation that some children do "grow out" of symptoms as their cortex catches up.
Additional structural findings include:
- Smaller caudate nucleus and prefrontal cortex volumes in childhood (these differences reduce with age and treatment)
- Reduced cerebellar volume
- Thinner cortex in prefrontal, temporal, and parietal regions
Default Mode Network Dysfunction
In individuals without ADHD, the Default Mode Network (DMN) — active during rest and self-referential thinking — is reliably suppressed when a task demands focused attention. In ADHD, this suppression fails: the DMN remains active during tasks, generating the "mind wandering" and intrusive self-referential thoughts that characterize inattentive symptoms. Abnormal DMN–task-positive network anticorrelation is among the most replicated fMRI findings in ADHD.
4. Etiology and Risk Factors
Genetic Factors
- Heritability 70–80% from twin studies; first-degree relatives have approximately 5-fold increased risk
- Polygenic inheritance; GWAS studies identify multiple common variants of small effect plus rare high-impact CNVs
- Gene-environment interaction: genetic risk is expressed and amplified by adverse environmental exposures
Prenatal Exposures
- Prenatal tobacco smoke — one of the strongest environmental risk factors; nicotine disrupts fetal dopaminergic development
- Prenatal alcohol exposure — even moderate consumption linked to increased risk; fetal alcohol spectrum disorder (FASD) overlaps significantly with ADHD
- Lead exposure — even low-level prenatal and early childhood lead exposure impairs dopaminergic circuits
- Valproate (anticonvulsant) use during pregnancy — strongly associated with ADHD, autism, and neurodevelopmental delays in offspring
- Acetaminophen (paracetamol) — epidemiological studies suggest association; causality not established
Perinatal and Early Life Factors
- Extreme prematurity (<28 weeks) and very low birth weight
- Perinatal hypoxia and birth complications
- Traumatic brain injury in childhood
- Severe early deprivation — as seen in institutional neglect (e.g., Romanian orphanages), produces an ADHD-like phenotype
Factors That Do NOT Cause ADHD
Several widely circulated myths about ADHD etiology deserve explicit correction:
- Sugar consumption does not cause ADHD — controlled studies have consistently refuted this belief
- Poor parenting or lack of discipline does not cause ADHD — though parenting stress is a consequence and can worsen outcomes
- Excessive screen time does not cause ADHD — it may temporarily worsen attention or mirror ADHD symptoms but is not a causal factor
- Vaccines do not cause ADHD
5. DSM-5 Diagnostic Subtypes
DSM-5 defines three presentations of ADHD based on the predominant symptom cluster over the past 6 months. Note that in DSM-5 terminology, these are called "presentations" rather than "subtypes" because they can shift over time.
Predominantly Inattentive Presentation (ADHD-PI)
Requires 6 or more of the following inattention symptoms (5 for adults age 17 and older):
- Often fails to give close attention to details or makes careless mistakes in schoolwork, work, or other activities
- Often has difficulty sustaining attention in tasks or play activities
- Often does not seem to listen when spoken to directly
- Often does not follow through on instructions and fails to finish schoolwork or chores
- Often has difficulty organizing tasks and activities
- Often avoids, dislikes, or is reluctant to engage in tasks that require sustained mental effort
- Often loses things necessary for tasks or activities (e.g., school materials, keys, wallet)
- Is often easily distracted by extraneous stimuli
- Is often forgetful in daily activities
Predominantly Hyperactive-Impulsive Presentation (ADHD-PHI)
Requires 6 or more of the following hyperactivity-impulsivity symptoms (5 for adults age 17 and older):
- Often fidgets with or taps hands or feet, or squirms in seat
- Often leaves seat in situations when remaining seated is expected
- Often runs about or climbs in situations where it is inappropriate (in adolescents/adults: may be limited to feeling restless)
- Often unable to play or engage in leisure activities quietly
- Is often "on the go," acting as if "driven by a motor"
- Often talks excessively
- Often blurts out an answer before a question has been completed
- Often has difficulty waiting his or her turn
- Often interrupts or intrudes on others (e.g., butts into conversations or games)
Combined Presentation (ADHD-C)
Requires 6 or more symptoms from both inattention and hyperactivity-impulsivity lists. This is the most common presentation in children referred to clinical settings.
Cross-Cutting Diagnostic Requirements
- Symptoms present before age 12 (changed from age 7 in DSM-IV)
- Symptoms present in 2 or more settings (home, school, work, social situations)
- Symptoms cause clinically significant impairment in social, academic, or occupational functioning
- Symptoms not better explained by another mental disorder
Severity Specifiers
- Mild — few symptoms beyond minimum threshold; minor functional impairment
- Moderate — symptoms and impairment between mild and severe
- Severe — many symptoms beyond threshold; marked impairment in multiple settings
6. Clinical Presentation
Children
In school-age children, ADHD commonly presents with:
- Academic underperformance despite adequate intelligence — inconsistent effort, unfinished work, poor organization
- Classroom behavior problems — calling out, leaving seat, difficulty waiting turns, disrupting others
- Peer relationship difficulties — impulsive social behavior, emotional reactivity, difficulty reading social cues
- Emotional dysregulation — intense, rapidly shifting emotions; low frustration tolerance; frequent meltdowns disproportionate to trigger
- Sleep difficulties — trouble falling asleep at night (common in ADHD independent of stimulant medication); daytime fatigue
Girls and Women
Females with ADHD are disproportionately diagnosed with the predominantly inattentive presentation and often go unrecognized because they do not display the overt hyperactivity that triggers referrals in boys. Key features include:
- Internalizing symptoms — anxiety, low self-esteem, depression more prominent than externalizing behavior
- Masking and camouflaging — learned compensatory behaviors (excessive lists, over-preparation) that hide struggles at the cost of significant mental energy
- Social sensitivity — heightened emotional reactivity in relationships; friendship difficulties
- Later diagnosis — average age of diagnosis often 5–10 years later than males, frequently triggered by increased demands in college or early adulthood
Adults
In adults, hyperactivity becomes more internalized ("inner restlessness"), and the clinical picture often centers on:
- Time blindness — profound difficulty estimating how long tasks take; chronic lateness; missing deadlines despite awareness of their importance
- Working memory failures — forgetting appointments, conversations, tasks mid-completion; losing objects daily
- Hyperfocus — paradoxical ability to lock onto highly stimulating or novel activities for hours while being unable to sustain routine tasks; often misunderstood as proof that the person "can focus when they want to"
- Rejection Sensitive Dysphoria (RSD) — intense, rapid emotional pain triggered by perceived or actual rejection or criticism; not in DSM-5 but widely recognized clinically and by patients as one of the most impairing features
- Occupational instability — job changes, conflict with supervisors, underemployment relative to intellectual ability
- Relationship difficulties — forgotten tasks, interrupted conversations, impulsive spending; intimate partners frequently misinterpret ADHD symptoms as lack of care
- ADHD tax — the cumulative financial and practical cost of the disorder: late fees, lost items requiring replacement, impulsive purchases, missed appointments, traffic tickets
- Higher motor vehicle accident rates — 3–4 times the accident rate of non-ADHD drivers
7. Diagnosis
Clinical Assessment
ADHD is a clinical diagnosis based on a comprehensive evaluation. There is no definitive biomarker, blood test, or brain scan that diagnoses ADHD. The evaluation should include a structured psychiatric interview, review of developmental history, reports from multiple informants (parent, teacher, partner), and validated rating scales.
Validated Rating Scales
- Conners-3 (Conners Third Edition) — comprehensive parent/teacher/self-report; widely used in children and adolescents; norm-referenced
- Vanderbilt ADHD Diagnostic Rating Scale — free, validated for pediatric primary care; parent and teacher versions; screens for comorbidities
- ASRS-v1.1 (Adult ADHD Self-Report Scale) — 18-item WHO-developed self-report screening tool for adults; a 6-item screener version is highly sensitive
- CAARS (Conners Adult ADHD Rating Scales) — comprehensive adult assessment; self-report and observer forms
- Brown ADD Rating Scales — emphasizes executive function impairment across 6 clusters; adult and child versions
Differential Diagnosis and Rule-Outs
Multiple conditions can mimic or co-occur with ADHD and must be assessed:
- Thyroid disorders — both hypothyroidism (fatigue, poor concentration) and hyperthyroidism (restlessness, inattention) can mimic ADHD
- Sleep disorders — obstructive sleep apnea and inadequate sleep produce inattention and hyperactivity identical to ADHD; polysomnography if suspected
- Vision and hearing impairments — should be screened in all children before ADHD diagnosis
- Learning disabilities (dyslexia, dyscalculia) — co-occur in 30–50%; specific academic testing required if suspected
- Anxiety disorders — anxiety produces inattention (mind preoccupied with worry) that closely mimics ADHD-PI; careful history distinguishes ego-syntonic worry from ADHD restlessness
- Depression — poor concentration, psychomotor slowing, and low energy can mimic inattentive ADHD
- PTSD and complex trauma — hypervigilance, concentration problems, emotional dysregulation can be indistinguishable from ADHD on rating scales; trauma history essential
- Autism Spectrum Disorder (ASD) — ADHD-like symptoms common in ASD; DSM-5 now permits dual diagnosis
- Bipolar disorder — particularly in the context of childhood-onset disinhibition; careful longitudinal assessment required
- Iron deficiency anemia — ferritin levels below 20–30 ng/mL associated with worse ADHD symptoms
Adjunctive Diagnostic Tools
- QBTEST (Quantitative Behavioral Test) — FDA-authorized computer-based test measuring inattention and hyperactivity via infrared motion tracking and continuous performance task; approved as an adjunct to, not replacement for, clinical evaluation
- Neuropsychological testing — indicated when learning disabilities or intellectual concerns are present; tests working memory, processing speed, and executive functions
- IQ testing — not required for ADHD diagnosis but valuable when learning disability is suspected or when the clinical picture is atypical
8. Treatment
Behavioral Therapy First (Children Under 6)
The American Academy of Pediatrics (AAP) 2019 Clinical Practice Guideline recommends behavior therapy as the first-line treatment for children under 6, before considering medication. Parent Training in Behavior Management (PTBM) is the most evidence-based approach — parents learn contingency management techniques, consistent limit-setting, and positive reinforcement strategies. Preschool-age children are particularly responsive to behavioral interventions and at greater risk of stimulant side effects.
For children aged 6 and older, and adolescents and adults, the guidelines recommend a combined behavioral + pharmacological approach as most effective, with either alone being superior to no treatment.
Stimulant Medications (First-Line for Age 6+)
Stimulants are the most extensively studied medications in child psychiatry. They are effective in approximately 70–80% of children and produce large effect sizes (Cohen's d approximately 0.8–1.0) in reducing core ADHD symptoms.
Methylphenidate-Based Stimulants
- Mechanism: Blocks reuptake of dopamine and norepinephrine transporters (DAT/NET), increasing synaptic catecholamine levels
- Ritalin (methylphenidate IR) — 4–6 hour duration; allows flexible dosing; useful for initial titration
- Concerta (methylphenidate OROS) — 10–12 hour duration; osmotic release system delivers pulsatile dose
- Daytrana (methylphenidate transdermal patch) — applied 9 hours before desired offset; option for those unable to swallow pills
- Jornay PM (methylphenidate delayed-release) — taken at bedtime; releases medication in the morning; addresses morning routine impairment
Amphetamine-Based Stimulants
- Mechanism: Blocks DAT/NET reuptake AND promotes active dopamine/norepinephrine release from vesicles; generally more potent than methylphenidate
- Adderall (mixed amphetamine salts IR) — 4–6 hour duration; 75% d-amphetamine, 25% l-amphetamine
- Adderall XR (mixed salts ER) — 10–12 hour duration
- Vyvanse (lisdexamfetamine) — prodrug: requires enzymatic cleavage in red blood cells to release active d-amphetamine; 12–14 hour duration; lower abuse and diversion potential due to prodrug mechanism; FDA-approved for ADHD and binge eating disorder
Common stimulant side effects: decreased appetite (especially at lunchtime), delayed sleep onset, increased heart rate and blood pressure, mild growth suppression (1–2 cm over years), rebound irritability as medication wears off. Side effects are generally dose-dependent and manageable with timing adjustments or dose reduction.
Non-Stimulant Medications
Non-stimulants are slower-onset (weeks to reach full effect) and generally have smaller effect sizes than stimulants, but are valuable for patients who do not tolerate stimulants, have significant anxiety, cardiovascular concerns, or substance abuse history, or who require 24-hour coverage without stimulant rebound.
- Atomoxetine (Strattera) — selective norepinephrine reuptake inhibitor (SNRI); takes 4–6 weeks for full benefit; non-scheduled (not a controlled substance); FDA-approved for ADHD in children, adolescents, and adults; also helpful for comorbid anxiety
- Guanfacine ER (Intuniv) — selective alpha-2A adrenergic agonist; improves PFC signal-to-noise ratio; particularly effective for emotional dysregulation, tics, and anxiety comorbid with ADHD; FDA-approved for children and adolescents aged 6–17; sedation is the main side effect
- Clonidine ER (Kapvay) — alpha-2 adrenergic agonist; broader receptor profile than guanfacine; FDA-approved for ADHD adjunct; also useful for sleep and tics
- Viloxazine ER (Qelbree) — serotonin-norepinephrine modulating agent; FDA-approved in 2021 for children 6–17, 2022 for adults; non-stimulant, non-scheduled; mechanism distinct from atomoxetine
- Bupropion (Wellbutrin) — dopamine/norepinephrine reuptake inhibitor; FDA-approved for depression; used off-label for ADHD; useful when comorbid depression is present; moderate evidence for ADHD efficacy
Behavioral and Psychosocial Treatments
- Parent Training in Behavior Management (PTBM) — teaching contingency management, consistent routines, praise and reward strategies
- Cognitive Behavioral Therapy (CBT) — for adolescents and adults; targets disorganization, procrastination, emotional dysregulation, and negative self-beliefs secondary to ADHD
- ADHD Coaching — practical, goal-oriented support for organization, time management, and daily functioning; not psychotherapy
- Exercise — acute aerobic exercise produces immediate, transient improvements in executive function, attention, and mood in ADHD; regular exercise is associated with structural brain changes in prefrontal regions; strong evidence base
- Mindfulness-Based Therapies — moderate evidence for attention regulation and emotional dysregulation in ADHD adults
Educational Accommodations
- IEP (Individualized Education Program) — for students whose ADHD substantially impairs educational performance; legally enforceable under IDEA
- 504 Plan — civil rights accommodation plan for students who don't qualify for special education but need support; common accommodations: extended time, preferential seating, reduced distraction testing environment, homework modifications, movement breaks
- College accommodations — extended time on exams, note-taking assistance, reduced distraction testing, priority registration
- Workplace accommodations — flexible scheduling, written instructions, noise-canceling headphones, task management software
9. Comorbidities
ADHD rarely presents in isolation. The majority of individuals with ADHD have at least one comorbid condition, with many carrying two or more. Comorbidities are not complications of ADHD per se but reflect shared neurobiological substrates and the psychological burden of living with an unmanaged condition.
- Oppositional Defiant Disorder (ODD) — present in 50–65% of children with ADHD; characterized by persistent angry/irritable mood, argumentativeness, and vindictiveness; not a failure of discipline
- Conduct Disorder (CD) — 15–25%; more severe disruptive behavior involving rights violations; presence requires careful differentiation from ADHD symptoms alone
- Anxiety Disorders — comorbid in 25–50% of children and adults with ADHD; anxiety can worsen ADHD symptoms and complicate treatment (stimulants may worsen anxiety in some)
- Major Depressive Disorder — 20–30%; often secondary to the cumulative failure and frustration of unmanaged ADHD; also shares neurobiological underpinnings
- Learning Disabilities — 30–50%; dyslexia and dyscalculia most common; ADHD and LD are independent conditions that frequently co-occur
- Tic Disorders and Tourette Syndrome — tics present in approximately 20% of children with ADHD; stimulants do not reliably worsen tics despite historical concern; guanfacine preferred when tics are present
- Sleep Disorders — 25–50%; delayed sleep phase is particularly common; sleep deprivation exacerbates all ADHD symptoms and must be addressed as part of treatment
- Substance Use Disorder (SUD) — ADHD increases SUD risk; critically, stimulant treatment initiated in childhood reduces the risk of later SUD (likely by reducing the drive for self-medication); untreated ADHD is the risk factor, not treatment
- Autism Spectrum Disorder (ASD) — DSM-5 now permits dual diagnosis (previously prohibited); overlap increasingly recognized; distinct needs require tailored treatment
- Bipolar Disorder — diagnosis in children is controversial; overlapping symptoms (impulsivity, distractibility, emotional dysregulation) require careful longitudinal evaluation; true bipolar disorder requires mood episode criteria beyond ADHD symptoms
10. Complications
- Academic underachievement — individuals with ADHD are significantly underrepresented in post-secondary education relative to their cognitive ability; this gap is largely preventable with appropriate support
- Occupational instability — higher job turnover, more disciplinary actions, lower income, greater underemployment relative to intellectual potential
- Relationship difficulties — higher divorce rates; ADHD symptoms frequently misinterpreted as lack of care or respect by partners unfamiliar with the condition
- Higher accident rates — 3–4 times elevated motor vehicle accident rate; higher rates of accidental injury throughout life
- Substance Use Disorder — 2–3 times elevated lifetime risk in untreated individuals; alcohol, cannabis, and stimulant misuse most common
- Increased suicidality — ADHD is associated with approximately doubled suicide attempt risk; comorbid depression and impulsivity are key contributing factors
- Lower socioeconomic outcomes — population studies demonstrate lower lifetime earnings and higher rates of financial difficulty
- Criminal justice involvement — a landmark 2012 NEJM study by Lichtenstein et al. demonstrated that periods of stimulant medication use were associated with significantly reduced criminal convictions in the same individuals, underscoring the public health importance of treatment
- Financial hardship — the cumulative "ADHD tax" of late fees, impulsive purchases, missed bills, and lost items represents a substantial hidden economic burden
- Chronic low self-esteem and shame — years of criticism, underperformance, and perceived laziness cause lasting psychological damage, particularly in those diagnosed late
11. Prognosis
ADHD is a lifelong condition for the majority of those diagnosed in childhood. 60–70% of children with ADHD continue to meet full diagnostic criteria in adulthood, and an additional 10–15% carry significant residual impairment below the diagnostic threshold. The functional trajectory is strongly modulated by whether and when treatment is received.
With treatment, outcomes are substantially improved across all domains: academic achievement, employment stability, relationship quality, reduced accident rates, and lower rates of substance abuse. Multimodal treatment — combining behavioral interventions, appropriate pharmacotherapy, and educational accommodations — produces the best outcomes. The landmark MTA (Multimodal Treatment Study of Children with ADHD) demonstrated that combined treatment produced superior outcomes to behavioral therapy alone and to medication alone in short-term follow-up.
Without treatment, the cumulative toll is significant. Adults with untreated ADHD have higher rates of unemployment, divorce, substance abuse, incarceration, accidental injury, and premature death. They are also more likely to have multiple failed treatment attempts for depression or anxiety that were actually manifestations of unrecognized ADHD.
Predictors of poorer outcome include: comorbid conduct disorder, lower socioeconomic status, high family conflict, early-onset substance use, and failure to receive adequate treatment. Predictors of better outcome include: above-average intelligence, good family support, access to behavioral therapy and school accommodations, appropriate stimulant treatment, and early diagnosis.
A critical public health message is that stimulant treatment in childhood does not cause later substance abuse — the evidence consistently shows the opposite: stimulant-treated individuals have lower rates of adult SUD than untreated ADHD controls. This myth deters many families from pursuing treatment, resulting in preventable harm.
Females diagnosed and treated late face a particularly important prognostic consideration: by the time of diagnosis, many have accumulated years of secondary anxiety, depression, and self-blame. These conditions require treatment in their own right; ADHD treatment alone may not fully reverse the psychological damage of late recognition.
12. Research Papers and References
Key Research Papers
- Faraone SV, et al. Attention-deficit/hyperactivity disorder. Nat Rev Dis Primers. 2021;7(1):2. PMID: 33479224. DOI: 10.1038/s41572-021-00260-3
- Polanczyk GV, et al. ADHD prevalence estimates across three decades: an updated systematic review. Int J Epidemiol. 2014;43(2):434–442. PMID: 24464188. DOI: 10.1093/ije/dyt261
- Shaw P, et al. Attention-deficit/hyperactivity disorder is characterized by a delay in cortical maturation. PNAS. 2007;104(49):19649–19654. PMID: 18024590. DOI: 10.1073/pnas.0707741104
- Arnsten AF. Catecholamine influences on dorsolateral prefrontal cortical networks. Biol Psychiatry. 2011;69(12):e89–99. PMID: 21489408. DOI: 10.1016/j.biopsych.2011.01.027
- Biederman J, Faraone SV. Attention-deficit hyperactivity disorder. Lancet. 2005;366(9481):237–248. PMID: 16023516. DOI: 10.1016/S0140-6736(05)66915-2
- Willcutt EG. The prevalence of DSM-IV attention-deficit/hyperactivity disorder: a meta-analytic review. Neurotherapeutics. 2012;9(3):490–499. PMID: 22976615. DOI: 10.1007/s13311-012-0135-8
- American Academy of Pediatrics. ADHD: Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of Attention-Deficit/Hyperactivity Disorder in Children and Adolescents. Pediatrics. 2019;144(4):e20192528. PMID: 31570648. DOI: 10.1542/peds.2019-2528
- Cortese S, et al. Comparative efficacy and tolerability of medications for attention-deficit hyperactivity disorder in children, adolescents, and adults: a systematic review and network meta-analysis. Lancet Psychiatry. 2018;5(9):727–738. PMID: 30097390. DOI: 10.1016/S2215-0366(18)30269-4
- Kessler RC, et al. The prevalence and correlates of adult ADHD in the United States. Am J Psychiatry. 2006;163(4):716–723. PMID: 16585449. DOI: 10.1176/appi.ajp.163.4.716
- Molina BS, et al. The MTA at 8 years: prospective follow-up of children treated for combined-type ADHD in a multisite study. J Am Acad Child Adolesc Psychiatry. 2009;48(5):484–500. PMID: 19318991. DOI: 10.1097/CHI.0b013e31819c23d0
- Franke B, et al. The genetics of attention deficit/hyperactivity disorder in adults, a review. Mol Psychiatry. 2012;17(10):960–987. PMID: 22105624. DOI: 10.1038/mp.2011.138
- Lichtenstein P, et al. Medication for attention deficit–hyperactivity disorder and criminality. NEJM. 2012;367(21):2006–2014. PMID: 23171097. DOI: 10.1056/NEJMoa1203241
PubMed Topic Searches
- PubMed: ADHD children treatment methylphenidate
- PubMed: ADHD adults prevalence
- PubMed: ADHD genetics dopamine
- PubMed: ADHD neurobiology prefrontal cortex
- PubMed: ADHD behavioral therapy
- PubMed: ADHD comorbidity anxiety depression
Connections
- Autism Spectrum Disorder
- OCD
- Anxiety
- Depression
- Insomnia
- Bipolar Disorder
- Tic Disorders
- Tourette Syndrome
- Magnesium
- Vitamin B6
- Tyrosine
- Ginkgo Biloba