Vitamin E (Tocopherol): The Master Fat-Soluble Antioxidant and Cell Membrane Protector
Vitamin E is a group of eight naturally occurring, fat-soluble compounds that collectively represent the body's most important lipid-phase antioxidant system. Discovered in 1922 by Herbert Evans and Katharine Scott Bishop as a dietary factor essential for reproduction in rats, Vitamin E was initially called the "anti-sterility factor" before being named tocopherol — derived from the Greek words tokos (childbirth) and pherein (to carry), with the suffix -ol indicating its chemical nature as an alcohol. Vitamin E's biological significance, however, extends far beyond reproduction. It is the primary guardian of cell membrane integrity, the chief protector against lipid peroxidation, a critical modulator of immune function, a regulator of gene expression, and a participant in cardiovascular protection, neurological health, skin integrity, and inflammatory control. Every cell membrane in the human body contains Vitamin E molecules embedded within its phospholipid bilayer, positioned to intercept and neutralize free radicals before they can initiate the destructive chain reactions of lipid peroxidation. Without adequate Vitamin E, cell membranes become vulnerable to oxidative degradation, leading to cellular dysfunction, tissue damage, and accelerated aging across virtually every organ system.
Table of Contents
- Chemical Forms — The Eight Members of the Vitamin E Family
- Antioxidant Defense — Guardian of Cell Membranes Against Lipid Peroxidation
- Cardiovascular Health — LDL Oxidation Prevention and Vascular Protection
- Immune Function — Enhancing Adaptive and Innate Immunity
- Skin Health — UV Protection, Wound Healing, and Anti-Aging
- Neurological Protection — Defending the Brain Against Oxidative Damage
- Eye Health — Protection Against Age-Related Ocular Disease
- Anti-Inflammatory Properties — Beyond Antioxidant Activity
- Reproductive Health — Vitamin E's Original Discovery Context
- Cancer Prevention Research — Evidence and Complexity
- Synergy with Vitamin C — The Antioxidant Network
- Dietary Sources — Natural Food Sources of Vitamin E
- Deficiency — Symptoms, Causes, and Clinical Manifestations
- Recommended Daily Allowance (RDA) and Supplementation Forms
- Gene Expression and Cell Signaling — Non-Antioxidant Functions
- Special Populations and Clinical Considerations
- Absorption, Transport, and Metabolism
- Vitamin E in Pregnancy and Pediatric Health
- Historical Significance and Research Evolution
- Connections
- Featured Videos
1. Chemical Forms — The Eight Members of the Vitamin E Family
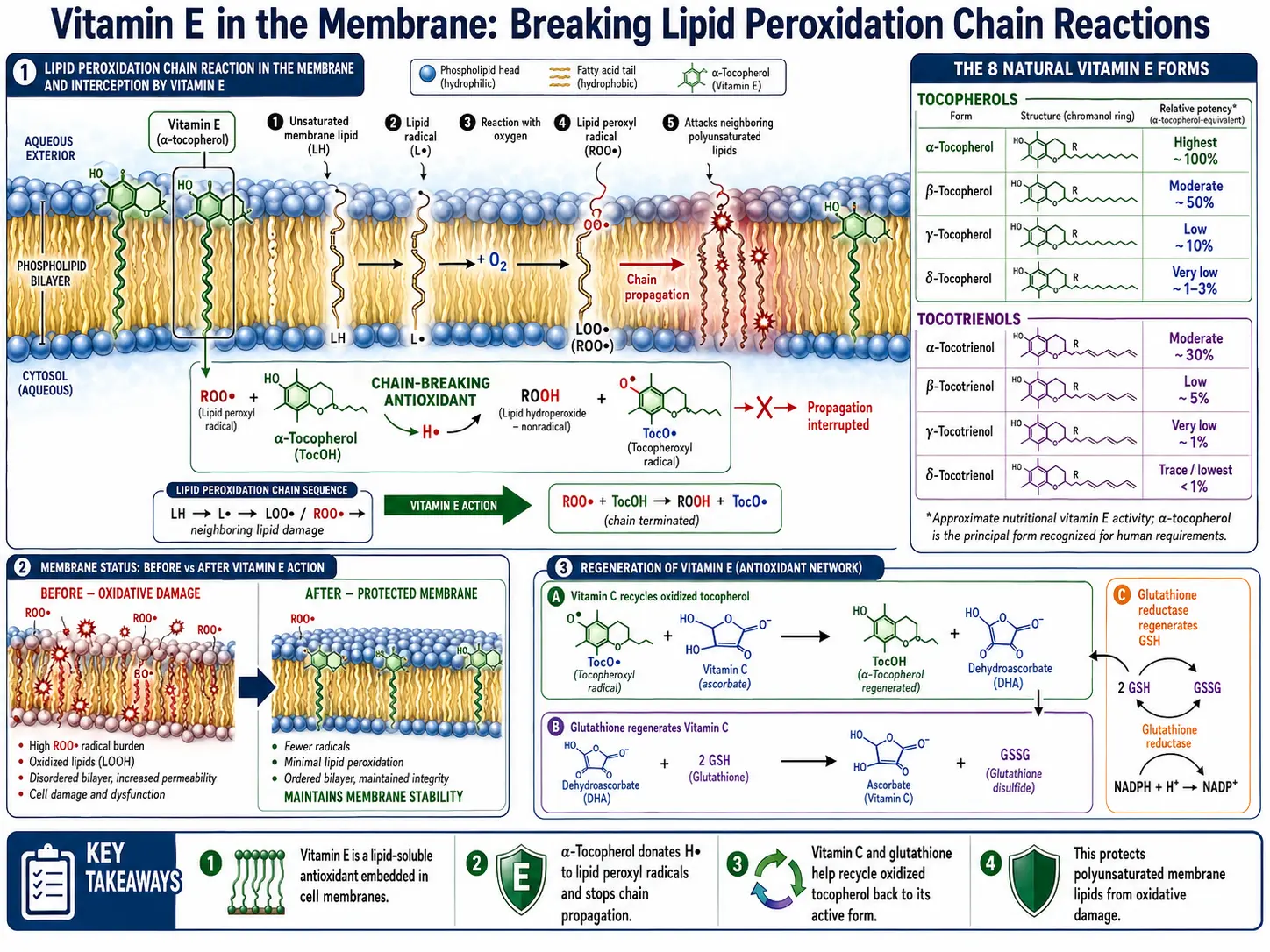
Vitamin E is not a single molecule but a family of eight structurally related compounds, each with distinct biological activities, tissue distributions, and health effects.
- Alpha-Tocopherol (α-Tocopherol): The most biologically active and abundant form of Vitamin E in human tissues. Alpha-tocopherol is preferentially retained in the body by the alpha-tocopherol transfer protein (α-TTP) in the liver, which selectively incorporates it into VLDL particles for distribution to tissues. It is the form that satisfies the Recommended Dietary Allowance (RDA) and the primary form measured in clinical assessments of Vitamin E status. Natural alpha-tocopherol exists as the RRR-stereoisomer (formerly called d-alpha-tocopherol), which has the highest biological activity.
- Beta-Tocopherol (β-Tocopherol): A minor form found in small quantities in foods. Beta-tocopherol has approximately 25-50% of the antioxidant activity of alpha-tocopherol and is not preferentially retained by the liver's transfer protein. It is present in some seed oils and cereal grains.
- Gamma-Tocopherol (γ-Tocopherol): The most abundant form of Vitamin E in the typical Western diet, found in high concentrations in soybean oil, corn oil, canola oil, and many nuts (especially walnuts and pecans). Gamma-tocopherol possesses unique anti-inflammatory and nitrogen-radical-scavenging properties not shared by alpha-tocopherol. It is particularly effective at trapping reactive nitrogen species (peroxynitrite, nitrogen dioxide), making it a complementary antioxidant to alpha-tocopherol. Research increasingly suggests that gamma-tocopherol has been underappreciated in its contributions to health.
- Delta-Tocopherol (δ-Tocopherol): The least methylated tocopherol, found in soybean oil and some other plant sources. Delta-tocopherol has lower antioxidant activity than alpha-tocopherol but may have unique anticancer and anti-inflammatory properties that are subjects of ongoing research.
- Alpha-Tocotrienol (α-Tocotrienol): Tocotrienols differ from tocopherols in having an unsaturated isoprenoid side chain (with three double bonds) instead of a saturated phytyl tail. Alpha-tocotrienol is found in palm oil, rice bran oil, and annatto. It has been shown to have potent neuroprotective properties, cardiovascular benefits, and anticancer effects. Tocotrienols distribute more uniformly in cell membranes due to their unsaturated tails and may recycle more efficiently than tocopherols.
- Beta-Tocotrienol (β-Tocotrienol): Found in palm oil and rice bran oil. Like other tocotrienols, it possesses antioxidant and anti-inflammatory properties, and research is exploring its role in cholesterol metabolism and neuroprotection.
- Gamma-Tocotrienol (γ-Tocotrienol): Found in palm oil, rice bran oil, and barley. Gamma-tocotrienol has demonstrated potent anti-inflammatory, anticancer (particularly against breast and pancreatic cancer cell lines), and cholesterol-lowering properties through inhibition of HMG-CoA reductase, the same enzyme targeted by statin drugs.
- Delta-Tocotrienol (δ-Tocotrienol): The most potent tocotrienol for HMG-CoA reductase inhibition and potentially the most effective anticancer tocotrienol. Delta-tocotrienol is abundant in annatto extract, which contains almost exclusively tocotrienols (predominantly delta-tocotrienol) with virtually no tocopherols.
- Synthetic vs. Natural Forms: Synthetic Vitamin E (dl-alpha-tocopherol or all-rac-alpha-tocopherol) is a mixture of eight stereoisomers, only one of which (the RRR form) is identical to natural Vitamin E. The natural form (d-alpha-tocopherol, RRR-alpha-tocopherol) has approximately twice the biological activity of the synthetic form on a weight basis, because the liver's alpha-tocopherol transfer protein preferentially binds the natural stereoisomer.
2. Antioxidant Defense — Guardian of Cell Membranes Against Lipid Peroxidation
Vitamin E's primary and most critical biological function is its role as the body's principal lipid-soluble antioxidant, protecting the polyunsaturated fatty acids (PUFAs) embedded in cell membranes, lipoproteins, and other lipid structures from oxidative destruction.
- Lipid Peroxidation Prevention: Polyunsaturated fatty acids in cell membranes are highly vulnerable to attack by free radicals. When a free radical abstracts a hydrogen atom from a PUFA, it initiates a self-propagating chain reaction of lipid peroxidation — each oxidized fatty acid generates additional radicals that attack neighboring PUFAs. A single initiating event can damage hundreds of fatty acid molecules. Vitamin E breaks this chain reaction by donating a hydrogen atom from its chromanol ring to the lipid peroxyl radical, converting it to a stable lipid hydroperoxide and terminating the chain reaction. The resulting tocopheroxyl radical is relatively stable and non-reactive.
- Cell Membrane Integrity: Every cell in the body is enclosed by a phospholipid bilayer membrane containing embedded Vitamin E molecules. These Vitamin E molecules are positioned with their chromanol ring at the membrane surface and their phytyl tail extending into the lipid interior, optimally placed to intercept radicals at the critical water-lipid interface where radical attack is most likely to originate. Without adequate Vitamin E, membranes lose fluidity, structural integrity, and function.
- Subcellular Membrane Protection: In addition to the plasma membrane, Vitamin E protects the membranes of mitochondria (critical for energy production and highly susceptible to oxidative damage due to the electron transport chain), the endoplasmic reticulum, lysosomes, and nuclear membranes.
- Lipoprotein Protection: Vitamin E is the primary antioxidant within LDL (low-density lipoprotein) particles, preventing the oxidation of LDL cholesterol — a process now understood as a key early event in the development of atherosclerosis. Each LDL particle typically contains 6-12 molecules of alpha-tocopherol.
- Synergy with Vitamin C: When Vitamin E donates a hydrogen atom to a lipid radical, it becomes a tocopheroxyl radical. Vitamin C (ascorbic acid), operating at the water-lipid interface, regenerates Vitamin E by donating an electron to the tocopheroxyl radical, restoring Vitamin E to its active antioxidant form. This synergistic partnership creates a seamless antioxidant network: Vitamin E protects the lipid phase, Vitamin C protects the aqueous phase, and Vitamin C recycles Vitamin E to maintain continuous lipid protection.
- Interaction with Selenium and Glutathione: Vitamin E works in concert with the selenium-dependent enzyme glutathione peroxidase, which reduces lipid hydroperoxides (the products of Vitamin E's chain-breaking action) to harmless lipid alcohols. This complementary relationship means that Vitamin E and selenium have overlapping protective functions — a deficiency of one can partially be compensated by adequate levels of the other.
- Protection of Red Blood Cells: Red blood cell membranes are especially vulnerable to oxidative damage due to their constant exposure to oxygen and their high PUFA content. Vitamin E deficiency leads to increased red blood cell fragility and hemolytic anemia, as the unprotected membranes rupture under oxidative stress.
3. Cardiovascular Health — LDL Oxidation Prevention and Vascular Protection
Vitamin E has been extensively studied for its role in cardiovascular health, with mechanisms that go beyond simple antioxidant activity to include direct vascular and anti-thrombotic effects.
- LDL Oxidation Prevention: The oxidation of LDL cholesterol is a critical initiating event in atherosclerosis. Native (unoxidized) LDL is not taken up by macrophages in arterial walls, but oxidized LDL is avidly internalized through scavenger receptors, leading to foam cell formation — the hallmark of early atherosclerotic lesions. Vitamin E, as the predominant antioxidant within LDL particles, provides the first line of defense against LDL oxidation. Laboratory studies consistently demonstrate that Vitamin E supplementation increases the resistance of LDL to oxidation.
- Endothelial Function: Vitamin E supports healthy endothelial function by reducing oxidative stress in blood vessel walls, preserving nitric oxide bioavailability, and decreasing endothelial adhesion molecule expression — steps that reduce leukocyte adhesion and the initiation of vascular inflammation.
- Anti-Platelet Effects: Vitamin E inhibits platelet aggregation through multiple mechanisms, including suppression of thromboxane A2 synthesis and protein kinase C inhibition. These anti-platelet effects may reduce the risk of thrombotic events, though they also necessitate caution with anticoagulant medications.
- Anti-Inflammatory Vascular Effects: Vitamin E reduces the expression of inflammatory adhesion molecules (VCAM-1, ICAM-1), inhibits monocyte adhesion to endothelial cells, and decreases the production of pro-inflammatory cytokines in vascular tissue — collectively reducing the inflammatory processes that drive atherosclerosis progression.
- Gamma-Tocopherol and Cardiovascular Health: Gamma-tocopherol may provide cardiovascular benefits distinct from alpha-tocopherol, particularly through its ability to scavenge reactive nitrogen species (peroxynitrite) that contribute to vascular inflammation and endothelial dysfunction. Some epidemiological studies suggest that dietary gamma-tocopherol intake is inversely associated with cardiovascular risk.
- Clinical Trial Evidence: Large-scale clinical trials have produced mixed results. The ATBC (Alpha-Tocopherol, Beta-Carotene Cancer Prevention) study showed a reduction in prostate cancer risk but no significant cardiovascular benefit. The HOPE (Heart Outcomes Prevention Evaluation) trial found no cardiovascular benefit from alpha-tocopherol supplementation in high-risk patients. However, some researchers argue that these trials used only alpha-tocopherol (which depletes gamma-tocopherol), used synthetic forms, and enrolled patients with advanced disease. The relationship between Vitamin E and cardiovascular health remains an active area of investigation.
4. Immune Function — Enhancing Adaptive and Innate Immunity
Vitamin E is a potent immunomodulator, with effects that are particularly pronounced in older adults whose immune systems are declining due to immunosenescence.
- T-Cell Enhancement: Vitamin E enhances T-cell proliferation and function by protecting T-cell membranes from oxidative damage, promoting immunological synapse formation, and modulating intracellular signaling pathways. T-cells are particularly sensitive to oxidative stress due to the high proportion of polyunsaturated fatty acids in their membranes.
- Prostaglandin E2 (PGE2) Reduction: Aging is associated with increased production of PGE2 by macrophages, which suppresses T-cell proliferation and IL-2 production. Vitamin E supplementation reduces PGE2 production, relieving this immunosuppressive effect and restoring T-cell function in elderly individuals. This mechanism is considered one of the primary pathways by which Vitamin E enhances immune function in the elderly.
- Natural Killer (NK) Cell Activity: Vitamin E supports NK cell cytotoxicity — the ability of these innate immune cells to recognize and destroy virally infected cells and cancer cells without prior sensitization.
- Respiratory Infection Protection: Several studies suggest that Vitamin E supplementation reduces the incidence and severity of upper respiratory tract infections in elderly nursing home residents, though the evidence is not entirely consistent across all trials.
- SENIEUR Study Protocol: Research conducted on immunologically healthy elderly individuals (selected by the SENIEUR protocol) has demonstrated that Vitamin E supplementation at 200 mg/day significantly enhances delayed-type hypersensitivity (DTH) responses, T-cell proliferation, and IL-2 production — markers of improved cell-mediated immunity.
5. Skin Health — UV Protection, Wound Healing, and Anti-Aging
Vitamin E plays multiple protective and restorative roles in skin health, both as a systemic nutrient and as a topically applied agent.
- UV Radiation Protection: Vitamin E in the skin absorbs UV light energy and quenches free radicals generated by UV exposure, reducing DNA damage, sunburn cell formation, and immunosuppression caused by solar radiation. It works synergistically with Vitamin C and other skin antioxidants to provide comprehensive photoprotection.
- Photoaging Prevention: Chronic UV exposure generates reactive oxygen species that degrade collagen, damage elastic fibers, and promote matrix metalloproteinase (MMP) expression — the molecular basis of photoaging (wrinkles, age spots, loss of elasticity). Vitamin E's antioxidant activity in the skin's lipid phase helps prevent these changes.
- Wound Healing: Vitamin E supports wound healing by protecting cell membranes during the inflammatory phase, supporting fibroblast proliferation, modulating collagen synthesis, and reducing excessive scar tissue formation. Adequate Vitamin E status supports all phases of wound repair.
- Scar Reduction: Topical Vitamin E has been widely used for scar reduction, though clinical evidence is mixed. Some studies suggest benefit for reducing hypertrophic scars and keloids, while others show no significant improvement. The moisturizing and anti-inflammatory effects of Vitamin E oil may contribute to improved scar appearance in some individuals.
- Moisturizing and Barrier Function: Vitamin E is a natural component of the skin's sebum and the stratum corneum lipid barrier. It helps maintain skin hydration and barrier integrity, reducing transepidermal water loss.
- Inflammatory Skin Conditions: Vitamin E may benefit inflammatory skin conditions such as eczema and psoriasis through its anti-inflammatory and antioxidant properties, though it is typically used as an adjunct rather than primary therapy.
- Synergy with Vitamin C for Skin: The combination of Vitamins C and E provides significantly greater photoprotection than either vitamin alone. Vitamin C regenerates Vitamin E after it neutralizes a radical, and the two vitamins protect complementary compartments (aqueous and lipid) of the skin. Many dermatological formulations combine both vitamins for maximal antioxidant protection.
6. Neurological Protection — Defending the Brain Against Oxidative Damage
The brain is exceptionally vulnerable to oxidative stress due to its high oxygen consumption (approximately 20% of total body oxygen), high PUFA content, relatively low antioxidant enzyme activity, and limited regenerative capacity. Vitamin E plays a critical protective role in neural tissue.
- Neuronal Membrane Protection: Neurons have extensive cell membranes (including long axonal processes) rich in polyunsaturated fatty acids, particularly DHA (docosahexaenoic acid). Vitamin E protects these lipid-rich membranes from peroxidation, preserving neuronal structure and signal transmission.
- Alzheimer's Disease: Oxidative stress is strongly implicated in the pathogenesis of Alzheimer's disease. Some clinical trials have shown that high-dose alpha-tocopherol (2000 IU/day) can slow functional decline in patients with moderate Alzheimer's disease. The TEAM-AD trial demonstrated a significant delay in clinical progression of mild-to-moderate Alzheimer's disease with Vitamin E supplementation.
- Cognitive Decline Prevention: Epidemiological studies suggest that higher dietary Vitamin E intake and higher plasma tocopherol levels are associated with a reduced risk of cognitive decline and dementia in aging populations. The protective effect appears strongest with dietary Vitamin E (which includes all forms) rather than supplemental alpha-tocopherol alone.
- Vitamin E Deficiency Neuropathy: Severe Vitamin E deficiency causes a characteristic progressive neurological syndrome called spinocerebellar ataxia with Vitamin E deficiency (AVED), characterized by peripheral neuropathy, cerebellar ataxia, loss of proprioception, areflexia, and skeletal muscle myopathy. This syndrome demonstrates unequivocally that Vitamin E is essential for neurological integrity.
- Alpha-Tocotrienol and Neuroprotection: Alpha-tocotrienol has demonstrated potent neuroprotective effects at nanomolar concentrations — far lower than those required for alpha-tocopherol — through mechanisms that include inhibition of 12-lipoxygenase, reduction of glutamate-induced neurotoxicity, and preservation of mitochondrial membrane potential.
- Parkinson's Disease: Some epidemiological evidence suggests that higher dietary Vitamin E intake may be associated with reduced Parkinson's disease risk, potentially through protection of dopaminergic neurons from oxidative damage. However, supplementation trials have not shown consistent benefits, and this remains an area of active research.
7. Eye Health — Protection Against Age-Related Ocular Disease
The eye is highly susceptible to oxidative damage due to constant light exposure, high metabolic activity, and high oxygen tension. Vitamin E contributes to the protection of multiple ocular structures.
- Age-Related Macular Degeneration (AMD): The Age-Related Eye Disease Study (AREDS) demonstrated that a combination of antioxidants including Vitamin E (400 IU), Vitamin C, beta-carotene, zinc, and copper reduced the progression of intermediate to advanced AMD by approximately 25%. Vitamin E's protection of retinal cell membranes and photoreceptor outer segments is believed to contribute to this benefit.
- Cataract Prevention: Oxidative damage to lens proteins (crystallins) causes protein aggregation and lens opacification — the molecular basis of cataracts. Vitamin E, present in both the lens and the aqueous humor, helps protect lens proteins from oxidative modification. Several epidemiological studies suggest that higher Vitamin E intake is associated with reduced cataract risk, particularly nuclear cataracts.
- Retinal Protection: The retina, particularly the photoreceptor outer segments, contains high concentrations of DHA and is continuously exposed to light energy and oxygen. Vitamin E protects these DHA-rich membranes from photooxidative damage, supporting visual function and retinal cell survival.
- Diabetic Retinopathy: Oxidative stress plays a role in the microvascular damage of diabetic retinopathy. Some research suggests that Vitamin E supplementation may reduce markers of retinal oxidative stress in diabetic patients, though clinical evidence of disease prevention remains limited.
8. Anti-Inflammatory Properties — Beyond Antioxidant Activity
Vitamin E possesses anti-inflammatory effects that are mechanistically distinct from and complementary to its antioxidant activity.
- Cyclooxygenase-2 (COX-2) Inhibition: Vitamin E, particularly gamma-tocopherol and delta-tocopherol, inhibits cyclooxygenase-2 activity and reduces prostaglandin E2 synthesis — effects that parallel those of non-steroidal anti-inflammatory drugs (NSAIDs) but without their gastrointestinal side effects.
- 5-Lipoxygenase (5-LOX) Inhibition: Gamma-tocopherol and tocotrienols inhibit 5-lipoxygenase, reducing the synthesis of pro-inflammatory leukotrienes. This dual inhibition of both COX-2 and 5-LOX distinguishes gamma-tocopherol from alpha-tocopherol in its anti-inflammatory profile.
- NF-kB Pathway Modulation: Vitamin E inhibits the activation of nuclear factor kappa-B (NF-kB), a master transcription factor that drives the expression of numerous pro-inflammatory genes, including cytokines (TNF-alpha, IL-1, IL-6), adhesion molecules, and inflammatory enzymes.
- C-Reactive Protein Reduction: Some studies demonstrate that Vitamin E supplementation reduces serum C-reactive protein (CRP) levels, a systemic marker of inflammation associated with cardiovascular disease risk.
- Reactive Nitrogen Species Scavenging: Gamma-tocopherol uniquely traps reactive nitrogen species such as peroxynitrite and nitrogen dioxide, which are potent mediators of inflammatory tissue damage. This property is not shared to the same degree by alpha-tocopherol, highlighting the importance of gamma-tocopherol in the body's anti-inflammatory defense.
9. Reproductive Health — Vitamin E's Original Discovery Context
Vitamin E was originally identified as a factor essential for reproduction, and its roles in reproductive health remain significant.
- Male Fertility: Vitamin E protects sperm cell membranes from oxidative damage, preserving sperm motility, morphology, and DNA integrity. Oxidative stress is a significant contributor to male infertility, and several studies demonstrate that Vitamin E supplementation (alone or combined with selenium or Vitamin C) can improve semen quality parameters and pregnancy rates in subfertile men.
- Female Reproductive Health: Vitamin E supports endometrial health, embryo implantation, and placental function. Some studies suggest that Vitamin E supplementation may increase endometrial thickness in women undergoing fertility treatment and may reduce the risk of preeclampsia, though evidence remains mixed.
- Pregnancy Outcomes: Adequate Vitamin E status during pregnancy supports fetal development, particularly the development of the nervous system and lungs. However, high-dose supplementation during pregnancy is not recommended without medical guidance due to potential risks.
- Dysmenorrhea: Several clinical trials have demonstrated that Vitamin E supplementation (200-500 IU/day) starting before and continuing through menstruation significantly reduces the severity of primary dysmenorrhea (menstrual pain), likely through inhibition of prostaglandin synthesis.
10. Cancer Prevention Research — Evidence and Complexity
The relationship between Vitamin E and cancer is complex, with different forms showing distinct effects across different cancer types.
- Prostate Cancer: The ATBC study initially found a 32% reduction in prostate cancer incidence with alpha-tocopherol supplementation. However, the SELECT (Selenium and Vitamin E Cancer Prevention Trial) later found a statistically significant 17% increase in prostate cancer risk with alpha-tocopherol supplementation alone. This discrepancy may relate to differences in the study populations, the form and dose of Vitamin E used, and the baseline Vitamin E status of participants.
- Gamma-Tocopherol and Cancer: In vitro and animal studies suggest that gamma-tocopherol and its metabolite gamma-CEHC have anticancer properties, including induction of apoptosis, inhibition of cell proliferation, and anti-inflammatory effects. Some researchers argue that supplementation with alpha-tocopherol alone depletes gamma-tocopherol (by competing for the alpha-TTP), potentially explaining the disappointing results of alpha-tocopherol-only cancer prevention trials.
- Tocotrienols and Cancer: Tocotrienols, particularly gamma- and delta-tocotrienols, have demonstrated potent anticancer effects in preclinical studies across multiple cancer types, including breast, pancreatic, liver, colon, and prostate cancer. Mechanisms include apoptosis induction, NF-kB inhibition, angiogenesis suppression, and immune modulation. Clinical trials of tocotrienols in cancer are in early stages.
- Colorectal Cancer: Some epidemiological studies suggest an inverse association between Vitamin E intake and colorectal cancer risk, possibly mediated through anti-inflammatory and antioxidant mechanisms in the colonic epithelium.
- Mixed-Tocopherol Supplementation: Emerging research suggests that supplementation with a mixture of tocopherols (alpha, gamma, and delta) may be more effective for cancer prevention than alpha-tocopherol alone, reflecting the complementary anticancer mechanisms of the different forms.
11. Synergy with Vitamin C — The Antioxidant Network
The partnership between Vitamins E and C represents one of the most elegant examples of biochemical synergy in human physiology.
- Vitamin E Regeneration: When Vitamin E neutralizes a lipid peroxyl radical in the cell membrane, it becomes a tocopheroxyl radical. Vitamin C, operating at the water-lipid interface, donates an electron to regenerate Vitamin E to its active antioxidant form. This recycling mechanism dramatically extends the effective antioxidant life of each Vitamin E molecule.
- Complementary Compartment Protection: Vitamin E protects the lipid-soluble compartments (cell membranes, lipoproteins) while Vitamin C protects the aqueous compartments (cytoplasm, extracellular fluid, blood plasma). Together, they provide comprehensive antioxidant coverage across both phases of cellular and tissue biology.
- Enhanced Photoprotection: The combination of topical Vitamins C and E provides significantly greater protection against UV-induced skin damage than either vitamin alone, as they protect complementary targets (lipid and aqueous) within the skin.
- LDL Protection: Vitamin C in plasma regenerates Vitamin E within LDL particles, extending the antioxidant protection of LDL against oxidation — a mechanism relevant to cardiovascular disease prevention.
- Further Network Connections: The antioxidant network extends beyond Vitamins C and E. Glutathione recycles oxidized Vitamin C (dehydroascorbic acid) back to ascorbic acid. Selenium-dependent glutathione peroxidase reduces the lipid hydroperoxides produced by Vitamin E's chain-breaking activity. Alpha-lipoic acid can regenerate both Vitamin C and glutathione. Coenzyme Q10 works alongside Vitamin E in the mitochondrial membrane. This interconnected network underscores the importance of broad antioxidant nutrition rather than reliance on a single supplement.
12. Dietary Sources — Natural Food Sources of Vitamin E
Vitamin E is found primarily in plant-based oils, nuts, seeds, and some vegetables. Different food sources provide different proportions of the various Vitamin E forms.
- Wheat Germ Oil: The single richest natural source of alpha-tocopherol, providing approximately 20 mg per tablespoon. Wheat germ oil also contains other tocopherols and is one of the most concentrated dietary sources of total Vitamin E.
- Sunflower Seeds and Oil: Excellent sources of alpha-tocopherol. A 1-ounce serving of sunflower seeds provides approximately 7.4 mg of alpha-tocopherol (nearly 50% of the RDA).
- Almonds: One of the best nut sources of alpha-tocopherol, providing approximately 7.3 mg per 1-ounce serving. Almond butter and almond milk also contribute meaningful amounts.
- Hazelnuts: Provide approximately 4.3 mg of alpha-tocopherol per ounce, along with other beneficial nutrients including manganese, copper, and phytosterols.
- Soybean and Corn Oil: Rich sources of gamma-tocopherol. While often cited as Vitamin E sources, these oils provide predominantly gamma-tocopherol rather than alpha-tocopherol.
- Peanuts and Peanut Butter: Good sources of alpha- and gamma-tocopherol, providing approximately 2.4 mg of alpha-tocopherol per ounce of peanuts.
- Spinach and Broccoli: Among the best vegetable sources of alpha-tocopherol, providing approximately 1.9 mg per cooked cup (spinach) and 1.2 mg per cup (broccoli).
- Avocados: Provide approximately 2.7 mg of alpha-tocopherol per whole avocado, along with healthy monounsaturated fats that enhance Vitamin E absorption.
- Palm Oil and Rice Bran Oil: Rich sources of tocotrienols, particularly alpha- and gamma-tocotrienols. Palm oil is one of the most concentrated natural sources of the tocotrienol family.
- Annatto Seeds: The richest known source of delta-tocotrienol, containing almost exclusively tocotrienols with virtually no tocopherols. Annatto-derived supplements provide a unique tocotrienol profile.
- Olive Oil: Provides modest amounts of alpha-tocopherol along with its well-known polyphenol antioxidants, contributing to the overall antioxidant profile of the Mediterranean diet.
13. Deficiency — Symptoms, Causes, and Clinical Manifestations
Vitamin E deficiency is uncommon in healthy people eating a normal diet, but it can develop in fat-malabsorption conditions (cystic fibrosis, celiac and Crohn's disease, cholestatic liver disease), in rare genetic disorders (abetalipoproteinemia, ataxia with vitamin E deficiency), and in premature infants — and when it does, the consequences can be serious, including progressive ataxia, peripheral neuropathy, muscle weakness, and hemolytic anemia. At the opposite extreme, very high supplemental doses carry their own risks, chiefly increased bleeding. For a full, patient-friendly guide to the symptoms, causes, and treatment of both, see Vitamin E Deficiency and Vitamin E Toxicity.
14. Recommended Daily Allowance (RDA) and Supplementation Forms
Understanding Vitamin E dosing, units of measurement, and supplementation forms is essential for appropriate use.
- RDA for Adults: The RDA for Vitamin E is 15 mg/day (22.4 IU) of alpha-tocopherol for adults of both sexes. This applies specifically to alpha-tocopherol (from food or supplements in the RRR form or the 2R forms).
- Lactation: The RDA increases to 19 mg/day during breastfeeding to account for Vitamin E secreted in breast milk.
- Tolerable Upper Intake Level (UL): The UL for supplemental alpha-tocopherol is 1000 mg/day (1500 IU of natural or 1100 IU of synthetic) for adults. This limit was established based on the potential for increased hemorrhagic risk at very high doses due to Vitamin E's anti-platelet and anticoagulant effects.
- Unit Conversions: 1 mg of natural (RRR) alpha-tocopherol = 1.49 IU. 1 mg of synthetic (all-rac) alpha-tocopherol = 1.10 IU. The newer convention uses mg of alpha-tocopherol rather than IU, but both systems remain in common use.
- Natural vs. Synthetic Supplements: Natural Vitamin E (d-alpha-tocopherol, RRR-alpha-tocopherol) has approximately twice the biological activity of synthetic Vitamin E (dl-alpha-tocopherol, all-rac-alpha-tocopherol). Product labels can be distinguished by the "d-" (natural) vs. "dl-" (synthetic) prefix.
- Mixed Tocopherol Supplements: Supplements providing a combination of alpha-, gamma-, and delta-tocopherols more closely mimic the natural dietary intake of Vitamin E and may provide broader antioxidant and anti-inflammatory coverage than alpha-tocopherol alone.
- Tocotrienol Supplements: Available as palm tocotrienol complex or annatto-derived tocotrienol (predominantly delta-tocotrienol). These supplements provide the tocotrienol forms increasingly recognized for their unique biological activities. Some formulations are tocopherol-free, as alpha-tocopherol at high doses can interfere with tocotrienol absorption and activity.
- Ester Forms: Vitamin E is often formulated as alpha-tocopheryl acetate or alpha-tocopheryl succinate for supplement stability. These ester forms are hydrolyzed in the gut to release free alpha-tocopherol for absorption. The acetate and succinate esters have no antioxidant activity until converted to free tocopherol, making them unsuitable for topical antioxidant protection (the ester must be cleaved before the vitamin is active).
- Absorption Enhancement: Vitamin E absorption requires dietary fat. Taking Vitamin E supplements with a meal containing fat significantly enhances absorption compared to taking them on an empty stomach.
- Drug Interactions: Vitamin E at high doses may enhance the anticoagulant effect of warfarin and other blood-thinning medications. It may also interact with statin drugs, chemotherapy agents, and radiation therapy. Patients on anticoagulant therapy or undergoing surgery should inform their healthcare providers about Vitamin E supplementation.
15. Gene Expression and Cell Signaling — Non-Antioxidant Functions
Beyond its well-known antioxidant role, Vitamin E directly regulates gene expression and modulates cell signaling pathways in ways that are independent of its radical-scavenging activity.
- Protein Kinase C (PKC) Inhibition: Alpha-tocopherol inhibits protein kinase C activity in a manner that is independent of its antioxidant function. PKC inhibition by Vitamin E reduces smooth muscle cell proliferation, platelet aggregation, and monocyte adhesion — effects directly relevant to cardiovascular protection.
- Gene Regulation: Vitamin E modulates the expression of genes involved in inflammation, cell proliferation, apoptosis, and extracellular matrix remodeling. It upregulates the expression of alpha-tropomyosin (a tumor suppressor protein) and connective tissue growth factor, while downregulating genes involved in inflammation and cell proliferation.
- Phospholipase A2 Inhibition: Alpha-tocopherol inhibits phospholipase A2, reducing the release of arachidonic acid from membrane phospholipids and thereby decreasing the substrate available for prostaglandin and leukotriene synthesis.
- Scavenger Receptor Regulation: Vitamin E downregulates the expression of scavenger receptors (CD36 and SR-A) on macrophages, reducing the uptake of oxidized LDL and foam cell formation — a direct anti-atherogenic mechanism independent of LDL oxidation prevention.
- PPAR-gamma Activation: Some Vitamin E metabolites activate peroxisome proliferator-activated receptor gamma (PPAR-gamma), a nuclear receptor involved in anti-inflammatory responses, glucose metabolism, and lipid homeostasis.
- Tocotrienol-Specific Signaling: Tocotrienols activate signaling pathways not significantly affected by tocopherols, including inhibition of HMG-CoA reductase (the cholesterol synthesis rate-limiting enzyme), activation of caspases for apoptosis induction in cancer cells, and modulation of the mevalonate pathway. These unique signaling effects contribute to the distinct biological profile of tocotrienols.
16. Special Populations and Clinical Considerations
Certain populations have unique Vitamin E requirements or considerations that warrant specific attention.
- Elderly Individuals: Aging is associated with increased oxidative stress, declining immune function, and increased risk of neurodegenerative disease. Vitamin E supplementation at moderate doses (200 IU/day) has shown consistent benefits for immune function in the elderly and may support cognitive maintenance.
- Patients with Metabolic Syndrome: Individuals with metabolic syndrome, obesity, and type 2 diabetes have increased oxidative stress and may benefit from Vitamin E's antioxidant and anti-inflammatory effects. Some studies suggest that Vitamin E supplementation improves insulin sensitivity and reduces markers of oxidative stress in these populations.
- Non-Alcoholic Fatty Liver Disease (NAFLD): High-dose Vitamin E (800 IU/day) has shown significant benefit for non-alcoholic steatohepatitis (NASH) in the PIVENS trial, improving liver histology and reducing inflammation. It is currently recommended as a treatment option for non-diabetic adults with biopsy-proven NASH.
- Athletes: Intense exercise generates substantial oxidative stress. While moderate Vitamin E intake supports exercise recovery, high-dose supplementation may blunt beneficial training adaptations by suppressing the reactive oxygen species signaling that drives mitochondrial biogenesis and other favorable exercise responses.
- Smokers: Cigarette smoke depletes Vitamin E through direct oxidative consumption. Smokers have lower plasma Vitamin E levels and higher Vitamin E turnover, potentially benefiting from increased intake. However, the ATBC study findings regarding lung cancer risk with beta-carotene (not Vitamin E) supplementation in smokers underscore the complexity of antioxidant supplementation in this population.
- Surgical Patients: Due to Vitamin E's anti-platelet effects, some surgeons recommend discontinuing high-dose Vitamin E supplements 2-4 weeks before elective surgery to reduce bleeding risk. This should be discussed with the surgical team on an individual basis.
17. Absorption, Transport, and Metabolism
Understanding how Vitamin E is absorbed, transported, and metabolized is essential for optimizing its nutritional benefit.
- Intestinal Absorption: Vitamin E is absorbed in the small intestine along with dietary fats, requiring bile salts for micelle formation and pancreatic lipase for fat digestion. Absorption efficiency varies from approximately 20-80% depending on the amount consumed, the form of Vitamin E, and the amount of dietary fat present. Absorption is enhanced when Vitamin E is consumed with a meal containing at least 3-5 grams of fat.
- Chylomicron Transport: After absorption, Vitamin E is incorporated into chylomicrons in intestinal enterocytes and transported via the lymphatic system to the bloodstream. During chylomicron catabolism by lipoprotein lipase in peripheral tissues, some Vitamin E is transferred to peripheral cells, while the chylomicron remnants deliver the remaining Vitamin E to the liver.
- Alpha-Tocopherol Transfer Protein (α-TTP): In the liver, the alpha-tocopherol transfer protein selectively binds RRR-alpha-tocopherol and incorporates it into nascent VLDL particles for redistribution to tissues throughout the body. This preferential binding is why alpha-tocopherol is the predominant form in human plasma and tissues — the liver actively retains and redistributes alpha-tocopherol while allowing other forms to be metabolized and excreted.
- Tissue Distribution: After secretion from the liver in VLDL, Vitamin E distributes to all tissues as lipoproteins are metabolized. Tissues with high lipid content or high oxidative stress tend to accumulate more Vitamin E. Adipose tissue serves as a large storage reservoir, while the adrenal glands, testes, platelets, and brain contain relatively high concentrations on a per-weight basis.
- Metabolism and Excretion: Non-alpha-tocopherol forms are preferentially metabolized by the cytochrome P450 enzyme CYP4F2 through omega-hydroxylation and subsequent beta-oxidation of the side chain, producing water-soluble carboxychromanol metabolites (CEHCs — carboxyethyl hydroxychromans) that are excreted in urine and bile. Alpha-tocopherol is metabolized by the same pathway but at a much lower rate due to its protection by alpha-TTP.
- Gamma-CEHC: The major urinary metabolite of gamma-tocopherol, gamma-CEHC (2,7,8-trimethyl-2-(beta-carboxyethyl)-6-hydroxychroman), has been found to possess natriuretic (sodium-excreting) activity and anti-inflammatory properties. This metabolite may contribute to some of gamma-tocopherol's unique biological effects, including potential blood pressure regulation.
- Bioavailability Factors: Several factors affect Vitamin E bioavailability: (1) dietary fat content enhances absorption, (2) fiber may reduce absorption, (3) mineral oil and fat substitutes (olestra) impair absorption, (4) medium-chain triglycerides may reduce Vitamin E absorption compared to long-chain triglycerides, and (5) genetic polymorphisms in alpha-TTP and CYP4F2 can affect individual Vitamin E status and requirements.
18. Vitamin E in Pregnancy and Pediatric Health
Vitamin E plays specific roles during pregnancy and in pediatric development that merit distinct consideration.
- Pregnancy Requirements: The RDA during pregnancy is 15 mg/day of alpha-tocopherol — the same as for non-pregnant women. However, Vitamin E demands increase during pregnancy due to fetal growth, placental development, and increased oxidative stress. Maternal plasma Vitamin E levels typically rise during pregnancy in parallel with increasing lipid levels.
- Preeclampsia Research: Oxidative stress is implicated in the pathogenesis of preeclampsia. Some studies have explored whether Vitamin E (often combined with Vitamin C) supplementation might prevent preeclampsia, but large randomized trials (VIP trial, WHO trial) have not demonstrated significant benefit. Current evidence does not support routine Vitamin E supplementation for preeclampsia prevention.
- Fetal Development: Vitamin E crosses the placenta, though less efficiently in early pregnancy than in late pregnancy. The fetus accumulates significant Vitamin E stores primarily during the third trimester, which is why premature infants are born with very low Vitamin E status and are at risk for deficiency-related complications.
- Premature Infant Supplementation: Premature infants may benefit from Vitamin E supplementation to prevent or reduce the severity of retinopathy of prematurity, bronchopulmonary dysplasia, and intraventricular hemorrhage, though optimal dosing and the balance between benefits and risks (potential increased infection risk at very high doses) remain subjects of ongoing research.
- Breast Milk Vitamin E: Breast milk provides Vitamin E to the nursing infant, with colostrum (early breast milk) containing particularly high concentrations. The RDA for lactating women is 19 mg/day to ensure adequate milk Vitamin E content. Maternal Vitamin E supplementation can increase breast milk Vitamin E levels.
- Childhood Cystic Fibrosis: Children with cystic fibrosis are at high risk for Vitamin E deficiency due to pancreatic insufficiency and fat malabsorption. Routine Vitamin E supplementation is recommended for all cystic fibrosis patients, and water-miscible forms of Vitamin E (TPGS — tocopheryl polyethylene glycol succinate) are often used to improve absorption in these patients.
19. Historical Significance and Research Evolution
Vitamin E was discovered in 1922 by Herbert McLean Evans and Katharine Scott Bishop at the University of California, Berkeley, as a fat-soluble "factor X" essential for reproduction in rats; it was soon named tocopherol, isolated in pure form from wheat-germ oil in 1936, and had its structure determined (Erhard Fernholz) and first synthesis achieved (Paul Karrer) in 1938. From that fertility puzzle, vitamin E grew into one of the most studied nutrients in the world — a family of antioxidant compounds central to cell-membrane protection, later tested in large and famously mixed clinical trials. The fuller story is told in the dedicated History & Discovery article.
Connections
- Deep Dives: Benefits Hub · Heart Health · Immune Function · Skin Health · Tocotrienols
- Vitamin E Deficiency
- Vitamin E Toxicity
- Vitamin C
- Vitamin A
- Vitamin D3
- Vitamin K
- Selenium
- Selenium and Cancer Prevention — selenoprotein biology, the NPC and SELECT trials, evidence across prostate/colorectal/lung cancers, and the U-shaped dose-response curve.
- Copper
- Alzheimer's Disease
- Cancer
- Atherosclerosis
- Cardiovascular Disease
- Cataracts
- Macular Degeneration
- Peripheral Neuropathy
- Oxidative Stress
- Glutathione
- Almonds
- Walnuts