Gallbladder Disease
Gallbladder disease encompasses a spectrum of pathological conditions affecting the gallbladder and biliary tract, ranging from asymptomatic cholelithiasis to life-threatening acute cholecystitis and biliary sepsis. It represents one of the most common indications for abdominal surgery worldwide and carries significant morbidity when inadequately managed.
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- Diagnosis
- Treatment
- Complications
- Prognosis
- Prevention
- Recent Research
- References
- Featured Videos
1. Overview
The gallbladder is a pear-shaped muscular sac located in a fossa on the inferior surface of the right hepatic lobe. Its primary function is the concentration and storage of bile, which it releases in response to cholecystokinin (CCK) stimulation to facilitate the emulsification and absorption of dietary fats and fat-soluble vitamins.
Gallbladder disease is a broad clinical category that includes the following principal conditions:
- Cholelithiasis: Formation and presence of gallstones within the gallbladder lumen.
- Biliary colic: Episodic visceral pain resulting from transient cystic duct obstruction by a gallstone, without overt infection or inflammation.
- Acute cholecystitis: Acute inflammation of the gallbladder wall, most commonly precipitated by sustained cystic duct obstruction.
- Chronic cholecystitis: Recurrent or persistent low-grade gallbladder inflammation, frequently associated with gallstones and a fibrotic, dysfunctional gallbladder wall.
- Acalculous cholecystitis: Gallbladder inflammation in the absence of gallstones, typically occurring in critically ill patients.
- Choledocholithiasis: Migration of gallstones into the common bile duct, with potential for biliary obstruction and cholangitis.
- Gallbladder cancer: Primary adenocarcinoma arising from the gallbladder epithelium, often associated with chronic cholelithiasis.
This article focuses predominantly on cholelithiasis, biliary colic, and acute cholecystitis, which together constitute the overwhelming majority of gallbladder disease encountered in clinical practice.
2. Epidemiology
Gallstone disease is among the most prevalent gastrointestinal disorders in developed nations. In the United States, approximately 10–15% of the adult population harbors gallstones, translating to roughly 25–30 million individuals. Annually, an estimated one million new cases of symptomatic gallstone disease are diagnosed, and cholecystectomy accounts for more than 750,000 surgical procedures per year, making it one of the most frequently performed abdominal operations.
The prevalence of cholelithiasis varies substantially across ethnic and geographic populations:
- Native American populations (particularly Pima Indians of Arizona) exhibit the highest known prevalence, with rates exceeding 70% in women over 25 years.
- Hispanic Americans have significantly higher rates than non-Hispanic whites, reflecting genetic and dietary factors.
- Northern European populations have intermediate prevalence (~15–20%).
- Sub-Saharan African and East Asian populations have historically lower cholesterol gallstone rates, though pigment stone disease is relatively more common in parts of Asia.
Gallstone prevalence increases with age in all populations. The female-to-male ratio is approximately 2:1 to 3:1 during the reproductive years, largely attributable to estrogenic effects on bile composition. After menopause, this disparity narrows substantially.
Of individuals with asymptomatic gallstones, approximately 1–2% per year will develop biliary colic or its complications. Over a 20-year period, roughly 25% of initially asymptomatic patients will develop symptoms, while the remainder maintain a benign natural course.
3. Pathophysiology
Gallstone Formation
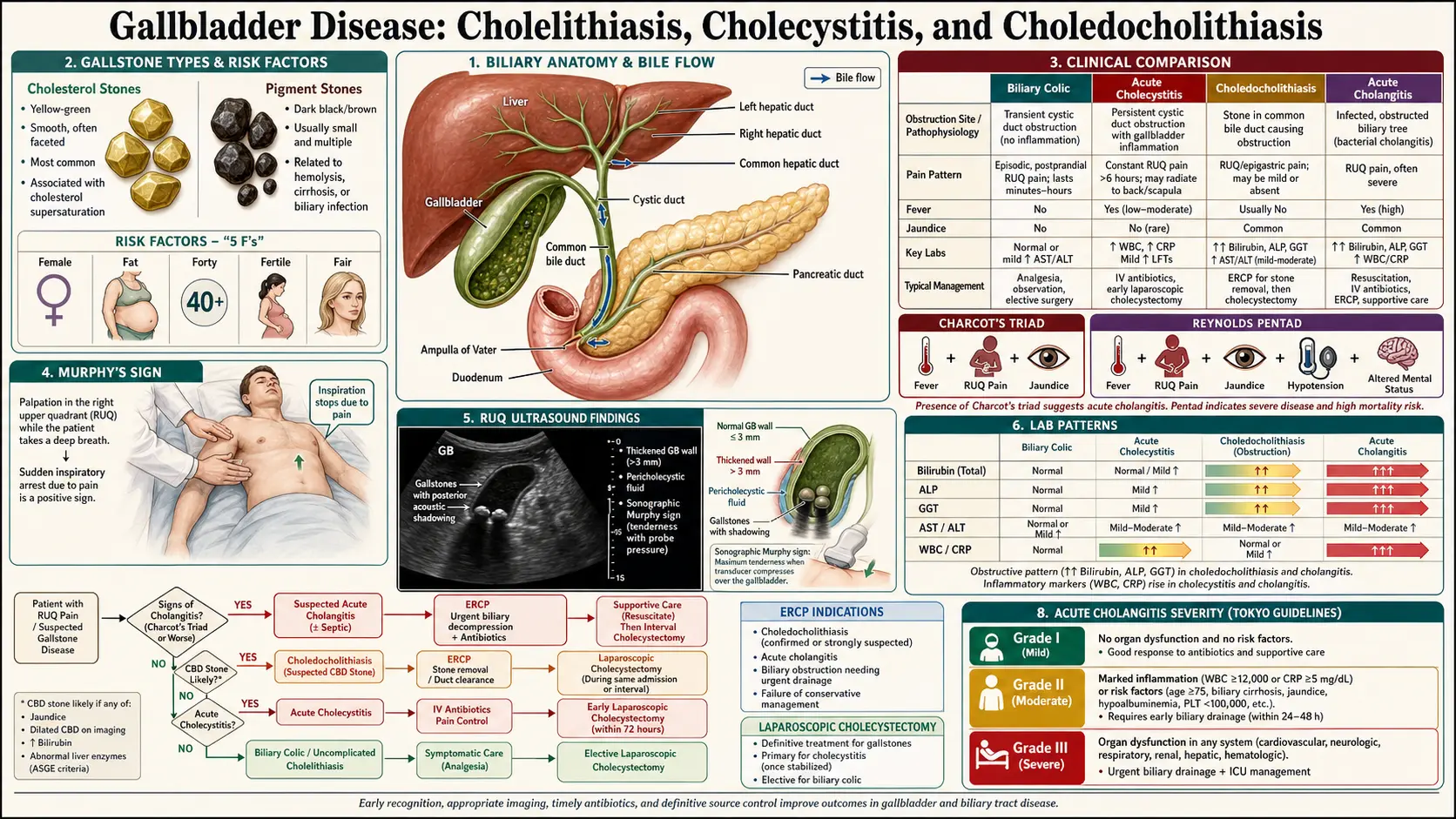
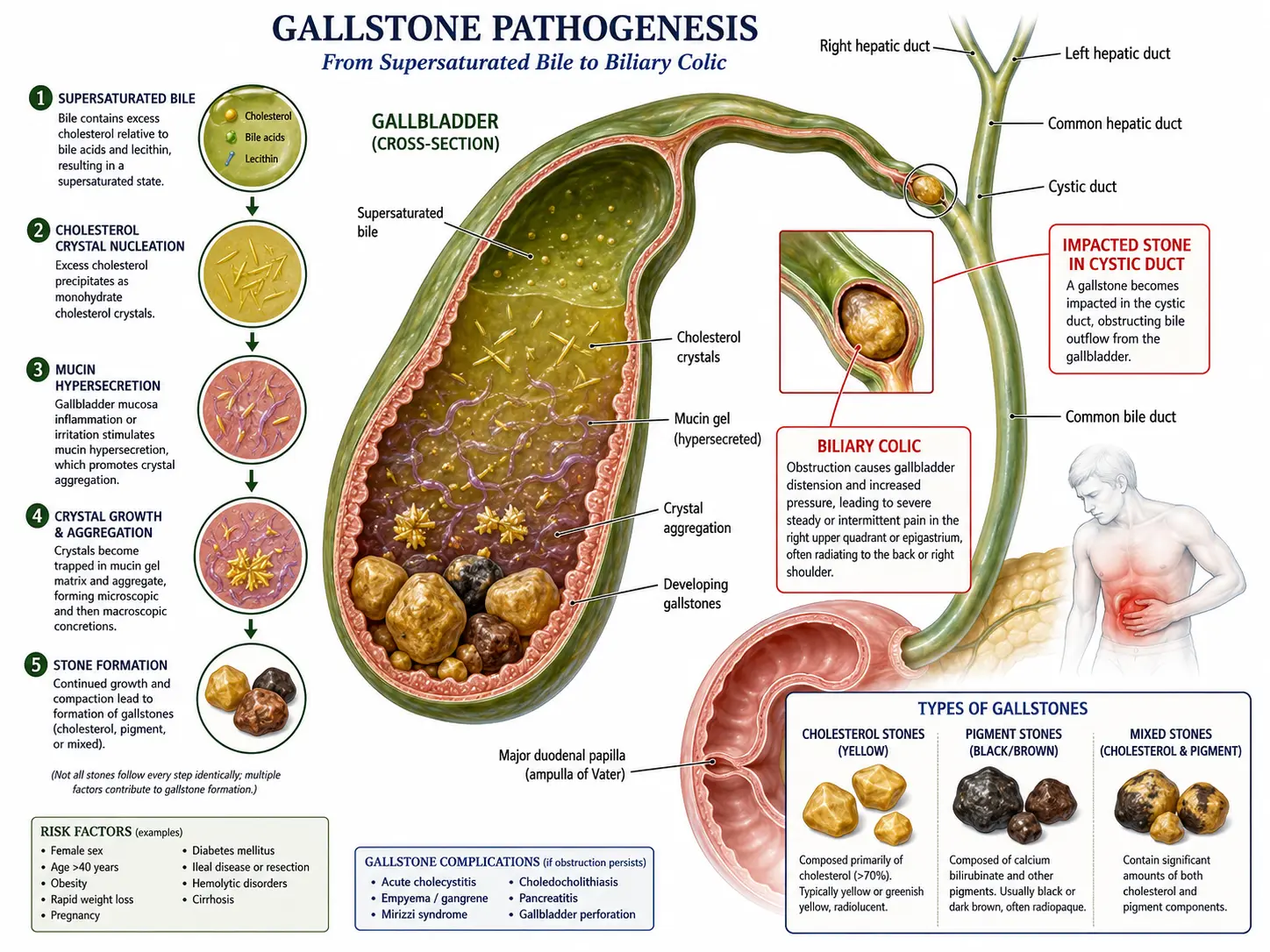
Gallstones are classified by composition into three main types: cholesterol stones (approximately 80% in Western populations), pigment stones (black and brown subtypes), and mixed stones. The pathogenesis of cholesterol gallstones involves three interacting mechanisms, often conceptualized as Admirand and Small's three-factor model: cholesterol supersaturation of bile, accelerated cholesterol crystal nucleation, and impaired gallbladder motility.
Supersaturation: Bile is a complex micellar solution containing cholesterol, phospholipids (predominantly lecithin), and bile salts. The lithogenic index quantifies the ratio of actual cholesterol concentration to the maximum solubilizing capacity of the bile salt-lecithin micellar system. When this index exceeds 1.0, bile is supersaturated and cholesterol crystals can precipitate. Increased hepatic cholesterol secretion, reduced bile salt synthesis or secretion (due to ileal disease or resection), and decreased phospholipid secretion all promote supersaturation.
Crystal nucleation: Even in supersaturated bile, crystallization requires nucleation — the formation of an initial crystal lattice. Mucin glycoproteins, immunoglobulins, and arachidonic acid metabolites secreted by the gallbladder mucosa act as pronucleating agents. Bile from gallstone patients demonstrates markedly shortened nucleation time compared to gallstone-free controls.
Impaired motility: Normal gallbladder contractility prevents crystal aggregation and growth by flushing nascent crystals into the duodenum. Gallbladder stasis — due to prolonged fasting, total parenteral nutrition (TPN), somatostatin analog use, or intrinsic smooth muscle dysfunction — allows crystal aggregation and stone growth. The interdigestive migrating motor complex (MMC) phase III contractions provide critical housekeeping function; disruption of the MMC is a recognized risk factor.
Black pigment stones are composed primarily of calcium bilirubinate and calcium carbonate, forming in the setting of chronic hemolysis (sickle cell disease, hereditary spherocytosis, thalassemia) or cirrhosis, where excess unconjugated bilirubin overwhelms bile's solubilizing capacity. Brown pigment stones are softer, greasier, and form primarily in the bile ducts in the setting of biliary stasis and bacterial infection (typically E. coli), which produces beta-glucuronidase that deconjugates bilirubin glucuronide.
Biliary Colic
Biliary colic occurs when a gallstone transiently impacts the cystic duct or gallbladder neck, often during a period of increased CCK-mediated gallbladder contraction postprandially. The resulting rise in intraluminal pressure produces visceral afferent pain transmitted via the celiac plexus and splanchnic nerves, perceived in the epigastrium and right upper quadrant. The stone typically dislodges spontaneously, resolving symptoms within 15 minutes to 6 hours. If obstruction is sustained beyond this window, the inflammatory cascade characteristic of acute cholecystitis is initiated.
Acute Cholecystitis
Sustained cystic duct obstruction leads to progressive distension of the gallbladder, mucosal ischemia, release of lysosomal enzymes, and activation of phospholipase A2, which converts biliary lecithin to lysophosphatidylcholine — a potent mucosal irritant. Prostaglandin E2 and I2 are released, amplifying inflammation. Secondary bacterial superinfection occurs in approximately 50–70% of cases within 24–72 hours, with Escherichia coli, Klebsiella spp., Enterococcus spp., and Bacteroides spp. most commonly identified. Perforation, pericholecystic abscess, or fistulous communication with adjacent viscera may result if the process is not interrupted.
Acalculous cholecystitis accounts for 5–10% of acute cholecystitis cases and is pathophysiologically distinct. It typically occurs in critically ill patients (ICU patients, post-major surgery, severe burns, trauma) and involves gallbladder ischemia secondary to hypoperfusion, increased bile viscosity due to dehydration or fasting, and the absence of CCK stimulation from enteral feeding. Mortality is significantly higher (up to 30%) than calculous cholecystitis due to delays in diagnosis and the underlying critical illness.
4. Etiology and Risk Factors
The classic mnemonic "5 Fs" — Fat, Female, Fertile, Forty, and Fair (of Northern European descent) — captures several major risk factors for cholesterol gallstone disease, though it incompletely reflects the multifactorial nature of cholelithiasis.
Non-modifiable Risk Factors
- Female sex: Estrogen upregulates hepatic LDL receptors, increasing cholesterol uptake and secretion into bile. Progesterone reduces gallbladder contractility. Oral contraceptives and hormone replacement therapy further elevate risk.
- Age: Cholesterol saturation of bile and gallbladder hypomotility both increase with age.
- Ethnicity: Genetic polymorphisms in ABCG5/ABCG8 (cholesterol transporters) and ABCB4 (phospholipid flippase) confer susceptibility. The ABCG8 p.D19H variant is strongly associated with gallstones in European populations.
- Family history: First-degree relatives of gallstone patients have a 2–4-fold elevated risk, reflecting shared genetic and dietary factors.
- Ileal disease or resection: Interruption of the enterohepatic circulation of bile salts (Crohn's disease, terminal ileal resection) reduces the bile salt pool and promotes lithogenesis.
- Hemolytic disorders: Chronic hemolysis (sickle cell anemia, hereditary spherocytosis, thalassemia, prosthetic heart valves) predisposes to black pigment stones.
- Cirrhosis: Impaired bile salt synthesis and secretion, combined with portal hypertension-related alterations in enterohepatic circulation, substantially increase gallstone risk. Prevalence of gallstones in cirrhosis exceeds 30%.
Modifiable Risk Factors
- Obesity: Increased hepatic cholesterol synthesis and secretion directly correlate with body mass index. Obesity also impairs gallbladder motility through altered CCK sensitivity.
- Rapid weight loss and bariatric surgery: Mobilization of adipose tissue floods the liver with fatty acids, markedly increasing cholesterol secretion. Roux-en-Y gastric bypass patients have a 30–40% risk of new gallstone formation within 6 months without prophylactic ursodeoxycholic acid (UDCA).
- Total parenteral nutrition: Absence of enteral feeding eliminates CCK stimulation, producing gallbladder stasis and biliary sludge within 3–4 weeks. Sludge may progress to frank gallstones.
- Hypertriglyceridemia and metabolic syndrome: Associated with increased cholesterol secretion and reduced bile salt synthesis, particularly in the context of insulin resistance.
- Medications: Ceftriaxone (precipitates as calcium ceftriaxone in bile), octreotide/somatostatin analogs (inhibit CCK release), thiazide diuretics, clofibrate, and estrogen-containing preparations all increase gallstone risk.
- Sedentary lifestyle: Physical activity stimulates gallbladder motility and bile turnover; inactivity is an independent risk factor.
5. Clinical Presentation
Asymptomatic Cholelithiasis
The majority (60–80%) of individuals with gallstones remain asymptomatic throughout their lives. Stones are frequently discovered incidentally on abdominal ultrasound performed for unrelated indications. These patients require no immediate intervention but warrant counseling on the symptoms that should prompt medical attention.
Biliary Colic
Biliary colic is characterized by the following features:
- Location: Constant, severe pain in the epigastrium or right upper quadrant (RUQ), often with radiation to the right subscapular region or interscapular area.
- Onset: Typically begins 30–60 minutes after a fatty meal but may occur at any time, including at rest or nocturnally.
- Duration: Episodes last 15 minutes to 6 hours and then resolve spontaneously. Persistence beyond 6 hours should raise concern for acute cholecystitis.
- Character: Despite the term "colic," the pain is typically constant rather than truly colicky (waxing and waning), reflecting sustained visceral distension rather than peristaltic cramping.
- Associated symptoms: Nausea, vomiting, and diaphoresis are common. Jaundice is absent unless a stone has migrated to the common bile duct.
- Physical examination: Notably benign between and during uncomplicated episodes; the abdomen is soft, and there is no guarding or peritoneal signs.
Acute Cholecystitis
Acute cholecystitis presents with more sustained and severe symptoms than biliary colic:
- Pain: Persistent RUQ or epigastric pain lasting more than 6 hours, often with radiation to the right shoulder (phrenic nerve irritation from peritoneal inflammation).
- Fever: Low-grade to moderate fever (38–38.5°C) is typical; high fever (>39°C) or rigors suggest complications (gangrenous cholecystitis, perforation, ascending cholangitis).
- Nausea and vomiting: Nearly universal.
- Murphy's sign: A cardinal clinical finding — inspiratory arrest on deep palpation of the RUQ at the costal margin during deep inspiration. The examiner applies steady pressure in the RUQ and asks the patient to inhale deeply; as the inflamed gallbladder descends into the examining fingers, pain causes the patient to halt inspiration abruptly. Sensitivity is approximately 65%, specificity 87% for acute cholecystitis. Murphy's sign may be diminished or absent in elderly patients, those on analgesia, or in the setting of acalculous cholecystitis.
- Sonographic Murphy's sign: Pain elicited by the ultrasound transducer directly over the gallbladder; reported sensitivity of up to 90% for acute cholecystitis.
- Peritoneal signs: Local guarding and rebound tenderness in the RUQ are present in more severe cases. Diffuse peritonitis indicates perforation.
Choledocholithiasis and Cholangitis
Choledocholithiasis (common bile duct stones) may be asymptomatic or may present with:
- Charcot's triad: RUQ pain, fever, and jaundice — present in approximately 50–75% of acute cholangitis cases.
- Reynolds' pentad: Charcot's triad plus altered mental status and septic shock — present in severe suppurative cholangitis and associated with high mortality.
- Biochemical profile: Elevated serum bilirubin, alkaline phosphatase, and gamma-glutamyltransferase (GGT), with transaminase elevation possible in the acute phase.
6. Diagnosis
Laboratory Investigations
In uncomplicated biliary colic, laboratory studies are typically normal. In acute cholecystitis, the following abnormalities are frequently observed:
- Complete blood count (CBC): Leukocytosis (12,000–15,000 cells/mm³) with neutrophilia is typical. Counts exceeding 20,000 cells/mm³ raise concern for gangrenous or emphysematous cholecystitis or perforation.
- C-reactive protein (CRP): Elevated; CRP >3 mg/dL correlates with severe cholecystitis in the Tokyo Guidelines severity grading.
- Liver function tests (LFTs): Mild transaminase elevation may occur due to hepatic inflammation or biliary hypertension. Significant hyperbilirubinemia and alkaline phosphatase elevation suggest choledocholithiasis or Mirizzi syndrome.
- Lipase and amylase: Elevated when gallstone pancreatitis is present (biliary pancreatitis).
- Blood cultures: Obtained in febrile patients; positive in 20–30% of acute cholangitis cases.
Imaging
Transabdominal Ultrasound (US) is the first-line imaging modality for suspected gallbladder disease, with sensitivity of 84–97% and specificity of 95–99% for gallstones. Ultrasound findings in acute cholecystitis include:
- Gallstones (echogenic foci with posterior acoustic shadowing)
- Pericholecystic fluid
- Gallbladder wall thickening (>4 mm)
- Gallbladder distension (>5 cm transverse diameter)
- Positive sonographic Murphy's sign
- Biliary sludge (echogenic material without acoustic shadowing)
Computed Tomography (CT) of the abdomen with intravenous contrast is not the preferred modality for gallstone detection (sensitivity approximately 75% for stones) but is invaluable for evaluating complications: gangrenous cholecystitis (intraluminal membranes, wall irregularity), emphysematous cholecystitis (intramural or intraluminal gas), perforation (pericholecystic abscess, pneumoperitoneum), and for surgical planning. CT is superior to ultrasound for evaluating the extrahepatic bile ducts and for assessing cholangitis.
Hepatobiliary Iminodiacetic Acid (HIDA) Scan (cholescintigraphy) is the most accurate imaging test for acute cholecystitis, with sensitivity of 95–97% and specificity of 85–90%. After intravenous injection of a technetium-99m-labeled iminodiacetic acid derivative, the radiopharmaceutical is excreted by hepatocytes into bile and normally concentrates in the gallbladder within 30–60 minutes. In acute cholecystitis, cystic duct obstruction prevents gallbladder filling — non-visualization of the gallbladder at 60 minutes (or at 4 hours after morphine augmentation) is diagnostic. HIDA scan is particularly useful when ultrasound is equivocal and when acalculous cholecystitis is suspected. Morphine augmentation (0.04 mg/kg IV) increases sphincter of Oddi tone, improving sensitivity by directing more radiotracer toward the gallbladder when the cystic duct is patent.
Magnetic Resonance Cholangiopancreatography (MRCP) is the investigation of choice for suspected choledocholithiasis and for delineating complex biliary anatomy, with sensitivity and specificity exceeding 90% for common bile duct stones. MRCP is non-invasive and avoids radiation, making it preferred over diagnostic endoscopic retrograde cholangiopancreatography (ERCP) when therapeutic intervention is not immediately planned.
Endoscopic Ultrasound (EUS) offers high sensitivity (97%) for choledocholithiasis, particularly for small stones (<5 mm) that may be missed on MRCP. It is increasingly used when MRCP findings are equivocal and therapeutic ERCP is being considered.
Tokyo Guidelines Severity Grading (TG18/TG13)
The Tokyo Guidelines, originally published in 2007 and updated in 2013 (TG13) and 2018 (TG18), provide internationally adopted diagnostic criteria and severity grading for acute cholecystitis. The TG18 diagnostic criteria require:
- Local signs of inflammation: Murphy's sign, RUQ mass/pain/tenderness
- Systemic signs of inflammation: Fever, elevated CRP, elevated WBC
- Imaging findings: Characteristic ultrasound or CT findings of acute cholecystitis
Suspected diagnosis requires one local sign plus one systemic sign. Definitive diagnosis requires imaging confirmation.
Severity is graded as follows:
- Grade I (Mild): Acute cholecystitis in otherwise healthy patients without organ dysfunction; inflammatory changes limited to the gallbladder. Responds to conservative management and elective surgery.
- Grade II (Moderate): Presence of one of the following: WBC >18,000/mm³, palpable tender RUQ mass, duration of complaints >72 hours, marked local inflammation (gangrenous cholecystitis, pericholecystic abscess, hepatic abscess, biliary peritonitis, emphysematous cholecystitis). Requires early laparoscopic cholecystectomy or biliary drainage.
- Grade III (Severe): Associated organ dysfunction — cardiovascular (hypotension requiring vasopressors), neurological (decreased consciousness), respiratory (PaO2/FiO2 <300), renal (oliguria, creatinine >2.0 mg/dL), hepatic (INR >1.5), hematological (platelet count <100,000/mm³). Requires immediate organ support and biliary drainage; surgery is deferred until stabilized.
7. Treatment
Asymptomatic Cholelithiasis
The current consensus, supported by long-term natural history data, is that prophylactic cholecystectomy is not indicated for the majority of asymptomatic gallstone patients. The annual risk of developing symptoms (<2%) and serious complications (biliary pancreatitis, cholangitis) does not justify the risks of surgery in most cases.
Exceptions where prophylactic cholecystectomy may be considered include:
- Porcelain gallbladder (certain subtypes with mucosal calcification associated with increased cancer risk)
- Gallstones >3 cm diameter (associated with increased gallbladder cancer risk)
- Gallbladder polyps >1 cm or rapidly growing polyps
- Anomalous pancreaticobiliary duct junction
- Patients undergoing bariatric surgery (concurrent cholecystectomy or prophylactic UDCA)
- Patients scheduled for organ transplantation
- Sickle cell anemia patients with cholelithiasis (given high risk of crisis and diagnostic uncertainty with abdominal pain)
Biliary Colic
Acute management consists of analgesics (NSAIDs are first-line as they also reduce prostaglandin-mediated gallbladder spasm; opioids such as ketorolac or meperidine are used when NSAIDs are contraindicated), antiemetics, and hydration. Patients who have experienced a symptomatic episode have a high rate of recurrence (70% within 2 years) and should be offered elective laparoscopic cholecystectomy, ideally within 6–8 weeks of the acute episode.
Acute Cholecystitis — Surgical Management
Laparoscopic cholecystectomy is the definitive and preferred treatment for acute cholecystitis. The timing of surgery is guided by the Tokyo Guidelines:
- Grade I: Early laparoscopic cholecystectomy within 72 hours of symptom onset or during the index hospitalization is recommended and associated with shorter hospital stay, lower conversion rates, and equivalent or superior outcomes compared to delayed surgery.
- Grade II: Early laparoscopic cholecystectomy is recommended in experienced centers. Biliary drainage (percutaneous transhepatic cholecystostomy or endoscopic transpapillary gallbladder drainage) is an alternative in patients not fit for immediate surgery.
- Grade III: Urgent biliary drainage (percutaneous cholecystostomy preferred) with immediate intensive care support; cholecystectomy is deferred until organ dysfunction resolves.
Conversion from laparoscopic to open cholecystectomy occurs in approximately 5–10% of elective cases and 10–20% of acute cases, most commonly due to dense adhesions, unclear anatomy (Calot's triangle obscured), or hemorrhage. The Critical View of Safety (CVS), described by Strasberg, mandates identification of the cystic duct and cystic artery as two structures entering the gallbladder before any clipping or division, and is the standard of care for prevention of bile duct injury.
Antibiotic Therapy
Antibiotic use in gallbladder disease follows the severity grade:
- Uncomplicated biliary colic: No antibiotics required.
- Grade I acute cholecystitis: Prophylactic antibiotics (single preoperative dose) are sufficient; postoperative antibiotics are not required in uncomplicated cases.
- Grade II/III acute cholecystitis: Empirical antibiotic therapy targeting gram-negative enteric organisms and anaerobes is indicated. Preferred regimens include cefazolin or ceftriaxone for mild-moderate community-acquired infection; piperacillin-tazobactam, ampicillin-sulbactam, or a carbapenem for healthcare-associated or severe infections. Duration is typically 4–7 days or until clinical resolution.
Non-surgical Management
Ursodeoxycholic acid (UDCA) at 10–15 mg/kg/day can dissolve small (<5 mm), radiolucent (cholesterol) gallstones in patients with a functioning gallbladder, but requires 6–24 months of therapy and stones recur in 50% within 5 years. Its primary role today is prophylaxis against gallstone formation in high-risk situations (rapid weight loss, bariatric surgery).
Extracorporeal shock wave lithotripsy (ESWL) combined with oral bile acid therapy was used historically for selected patients but has been largely supplanted by laparoscopic cholecystectomy and is rarely employed in current practice.
Percutaneous cholecystostomy involves ultrasound- or CT-guided placement of a drain into the gallbladder lumen and provides rapid decompression and drainage in critically ill patients who cannot tolerate general anesthesia. It is a temporizing measure; interval cholecystectomy is performed once the patient has recovered, or the drain may remain permanently in patients deemed too high-risk for surgery.
ERCP and Choledocholithiasis
Endoscopic retrograde cholangiopancreatography (ERCP) with endoscopic sphincterotomy (ES) and stone extraction is the preferred treatment for symptomatic choledocholithiasis. Success rates for stone clearance exceed 85–90% for stones <1 cm. Mechanical lithotripsy, electrohydraulic lithotripsy (EHL), or laser lithotripsy (cholangioscopy-guided) are employed for large or impacted stones. Following successful ERCP and stone clearance, interval laparoscopic cholecystectomy is recommended to prevent recurrence. Single-stage laparoscopic common bile duct exploration with cholecystectomy is an alternative in expert centers.
8. Complications
Gangrenous Cholecystitis
Occurs in 2–30% of acute cholecystitis cases, particularly in elderly, diabetic, and immunocompromised patients. Transmural ischemia and necrosis of the gallbladder wall result from sustained intraluminal pressure and vascular occlusion. CT demonstrates intraluminal membranes, discontinuous or irregular wall enhancement, and striated wall thickening. Gangrenous cholecystitis is associated with high rates of perforation and requires urgent surgical intervention. Murphy's sign may paradoxically be absent due to denervation of the necrotic gallbladder wall.
Emphysematous Cholecystitis
A rare (approximately 1% of acute cholecystitis) but life-threatening variant characterized by gas-forming organisms (Clostridium perfringens, E. coli, Klebsiella) within the gallbladder wall or lumen. More common in diabetic men. CT or plain radiograph reveals intramural or intraluminal gas. Mortality approaches 15–25%. Requires emergency cholecystectomy and broad-spectrum antibiotics including anaerobic coverage.
Gallbladder Perforation
Niemeier classification distinguishes: Type I (free perforation with bile peritonitis — most severe, mortality ~30%), Type II (pericholecystic abscess — localized), and Type III (cholecystoenteric fistula). Free perforation requires emergency surgery. Pericholecystic abscesses may initially be managed with percutaneous drainage.
Mirizzi Syndrome
External compression of the common hepatic duct by a large stone impacted in the cystic duct or Hartmann's pouch, causing obstructive jaundice. McSherry classification (Types I–V) guides surgical management, ranging from simple cholecystectomy (Type I) to hepaticojejunostomy for complex fistulas (Types III–V). MRCP or ERCP establishes the diagnosis.
Gallstone Ileus
A rare (0.3–0.5% of intestinal obstructions) but serious complication in which a large gallstone erodes through a cholecystoenteric fistula (most commonly cholecystoduodenal) and impacts at the terminal ileum (Bouveret syndrome when impacted in the duodenum). Rigler's triad on plain radiograph: pneumobilia, small bowel obstruction, and ectopic gallstone. Treatment is surgical enterolithotomy; management of the fistula is individualized.
Acute Gallstone Pancreatitis
Gallstones are the most common cause of acute pancreatitis in developed nations (~40%). Migration of a stone through the ampulla of Vater causes transient ampullary obstruction, pancreatic ductal hypertension, and activation of pancreatic proenzymes. ERCP with sphincterotomy within 24–72 hours is indicated for severe acute biliary pancreatitis with concurrent cholangitis or biliary obstruction. Cholecystectomy should be performed during the index hospitalization for mild biliary pancreatitis to prevent recurrence (25–30% risk without definitive treatment within weeks).
Gallbladder Cancer
Gallbladder adenocarcinoma is the most common biliary tract malignancy and is strongly associated with chronic cholelithiasis, porcelain gallbladder (selective subtypes), gallbladder polyps, anomalous pancreaticobiliary junction, and chronic Salmonella typhi infection. The 5-year overall survival remains poor (~5–15%) due to late-stage presentation. Incidental gallbladder carcinoma found at cholecystectomy for presumed benign disease has a more favorable prognosis, with T1a lesions (lamina propria invasion) cured by simple cholecystectomy alone.
Postcholecystectomy Syndrome
A heterogeneous entity in which patients continue to experience biliary-type symptoms following cholecystectomy. Causes include sphincter of Oddi dysfunction (SOD), retained common bile duct stones, bile duct stricture, cystic duct remnant syndrome, and non-biliary diagnoses (irritable bowel syndrome, peptic ulcer disease) that were pre-existing and not addressed by cholecystectomy. Manometry-documented SOD Types I and II respond to endoscopic sphincterotomy.
9. Prognosis
The prognosis for uncomplicated gallstone disease treated with cholecystectomy is excellent. Laparoscopic cholecystectomy carries a mortality of <0.1% in elective settings. The overall bile duct injury rate is 0.3–0.5% for laparoscopic procedures, compared to 0.1–0.2% for open surgery. Major bile duct injuries require hepaticojejunostomy or hepaticojejunostomy with Roux-en-Y reconstruction and are associated with significant long-term morbidity including recurrent cholangitis, secondary biliary cirrhosis, and reduced quality of life.
Acute cholecystitis without complications carries a low mortality (<1%) in otherwise healthy adults. Grade III acute cholecystitis with multi-organ dysfunction has a substantially higher mortality, particularly in elderly patients, and complication rates correlate directly with delay in appropriate management.
Patients with a history of gallstone pancreatitis who do not undergo cholecystectomy have a 25–30% risk of recurrent pancreatitis within 6 weeks, reinforcing the need for early definitive surgical management. After successful cholecystectomy, the recurrence risk is negligible.
10. Prevention
Primary prevention strategies target modifiable risk factors:
- Weight management: Maintaining a healthy BMI reduces gallstone risk proportionally. Moderate, sustained weight loss (<1.5 kg/week) is preferred over rapid loss.
- Physical activity: Regular aerobic exercise reduces gallstone risk by approximately 20–40% through improved gallbladder motility and reduced metabolic syndrome.
- Dietary modification: A diet rich in polyunsaturated fats, fiber, and moderate in carbohydrates reduces lithogenicity. Coffee consumption (2–3 cups/day) has been consistently associated with reduced gallstone risk, possibly through stimulation of CCK release and gallbladder motility. Extreme fat restriction is paradoxically lithogenic due to elimination of CCK stimulus.
- Ursodeoxycholic acid prophylaxis: Strongly recommended at 500–600 mg/day (or 300 mg twice daily) for patients undergoing rapid weight loss programs or bariatric surgery. Reduces gallstone formation by approximately 40% in this population.
- Statin therapy: Epidemiological data suggest statins reduce cholesterol secretion into bile and may lower gallstone risk as a secondary benefit, though this is not an established indication.
- Enteral nutrition: In patients receiving TPN, supplemental enteral feeding (even small volumes) stimulates CCK release and reduces biliary sludge formation.
11. Recent Research
Recent investigations have advanced understanding of gallbladder disease pathogenesis and treatment:
- Microbiome and cholelithiasis: Emerging evidence implicates gut dysbiosis in gallstone pathogenesis. Altered bile acid metabolism by intestinal bacteria modifies the ratio of primary to secondary bile acids, affecting cholesterol solubility in bile. Specific microbial signatures have been identified in gallstone patients compared to stone-free controls.
- Genetic determinants: Genome-wide association studies (GWAS) have identified additional susceptibility loci beyond ABCG5/ABCG8, including variants in TM4SF4, SULT2A1, and CYP7A1. These findings open potential pharmacogenomic approaches to lithogenesis prevention.
- Single-incision laparoscopic surgery (SILS) and robotic cholecystectomy: Compared to standard 3-4 port laparoscopy in randomized trials, SILS offers marginal cosmetic advantages but comparable complication rates and longer operative times. Robotic platforms have not demonstrated superiority to laparoscopic cholecystectomy in randomized data and carry higher costs.
- ERCP versus laparoscopic common bile duct exploration (LCBDE): Meta-analyses suggest equivalent outcomes for choledocholithiasis, with single-stage LCBDE associated with shorter hospital stay and lower cost. Single-stage management is gaining traction in high-volume centers.
- Tokyo Guidelines TG18 validation: Prospective multicenter validation studies have confirmed the diagnostic accuracy and severity stratification of TG18 criteria, supporting their global adoption in acute cholecystitis management.
- Cholecystokinin receptor agonists: Research into CCK-A receptor agonists as pharmacological agents to enhance gallbladder motility and reduce stone formation is ongoing, though no agent has yet reached clinical application.
12. References
- Yokoe M, Hata J, Takada T, et al. Tokyo Guidelines 2018: diagnostic criteria and severity grading of acute cholecystitis. J Hepatobiliary Pancreat Sci. 2018;25(1):41-54.
- Okamoto K, Suzuki K, Takada T, et al. Tokyo Guidelines 2018: flowchart for the management of acute cholecystitis. J Hepatobiliary Pancreat Sci. 2018;25(1):55-72.
- Stinton LM, Shaffer EA. Epidemiology of gallbladder disease: cholelithiasis and cancer. Gut Liver. 2012;6(2):172-187.
- Portincasa P, Moschetta A, Palasciano G. Cholesterol gallstone disease. Lancet. 2006;368(9531):230-239.
- Beal JM. Historical perspective of gallstone disease. Surg Gynecol Obstet.
- Strasberg SM, Brunt LM. Rationale and use of the critical view of safety in laparoscopic cholecystectomy. J Am Coll Surg. 2010;211(1):132-138.
- Gallaher JR, Charles A. Acute cholecystitis: a review. JAMA. 2022;327(10):965-975.
- Williams E, Beckingham I, El Sayed G, et al. Updated guideline on the management of common bile duct stones (CBDS). Gut. 2017;66(5):765-782.
- Gurusamy KS, Davidson C, Gluud C, Davidson BR. Early versus delayed laparoscopic cholecystectomy for people with acute cholecystitis. Cochrane Database Syst Rev. 2013;6:CD005440.
- Indar AA, Beckingham IJ. Acute cholecystitis. BMJ. 2002;325(7365):639-643.
- Di Ciaula A, Wang DQ, Portincasa P. An update on the pathogenesis of cholesterol gallstone disease. Curr Opin Gastroenterol. 2018;34(2):71-80.
- Ransohoff DF, Gracie WA. Treatment of gallstones. Ann Intern Med. 1993;119(7 Pt 1):606-619.
- Paumgartner G, Sauerbruch T. Gallstones: pathogenesis. Lancet. 1991;338(8775):1117-1121.
- Shabanzadeh DM. New determinants for gallstone disease? J Clin Gastroenterol. 2018;52(7):570-578.
- Nakeeb A, Comuzzie AG, Martin L, et al. Gallstones: genetics versus environment. Ann Surg. 2002;235(6):842-849.
- Csikesz N, Ricciardi R, Tseng JF, Shah SA. Current status of surgical management of acute cholecystitis in the United States. World J Surg. 2008;32(10):2230-2236.
- Aune D, Vatten LJ, Boffetta P. Tobacco smoking and the risk of gallbladder disease. Eur J Epidemiol. 2016;31(7):643-653.
- Erlinger S. Gallstones in obesity and weight loss. Eur J Gastroenterol Hepatol. 2000;12(12):1347-1352.
Research Papers
Curated PubMed topic searches of peer-reviewed literature on Gallbladder Disease. Each link opens a live PubMed query so you always see the most current studies.
- PubMed: Gallstone epidemiology
- PubMed: Acute cholecystitis management
- PubMed: Laparoscopic cholecystectomy
- PubMed: Gallstone pathogenesis
- PubMed: Ultrasound diagnosis
- PubMed: Biliary colic
- PubMed: Choledocholithiasis and ERCP
- PubMed: Gallbladder cancer
- PubMed: Porcelain gallbladder
- PubMed: Ursodeoxycholic acid therapy
- PubMed: Gallstones and bariatric surgery
- PubMed: Acalculous cholecystitis
Connections
- Pancreatitis
- Gastroesophageal Reflux Disease (GERD)
- SIBO
- SIBO Root Causes
- Magnesium
- Bloating
- Milk Thistle
- Turmeric
- Vitamin C
- Cirrhosis
- Crohn's Disease
- Irritable Bowel Syndrome
- Jaundice
- Cancer
- Obesity
- GGT (Liver Health)
- Abdominal Pain
- Liver Disease
- Pancreatic Cancer