Plantar Fasciitis
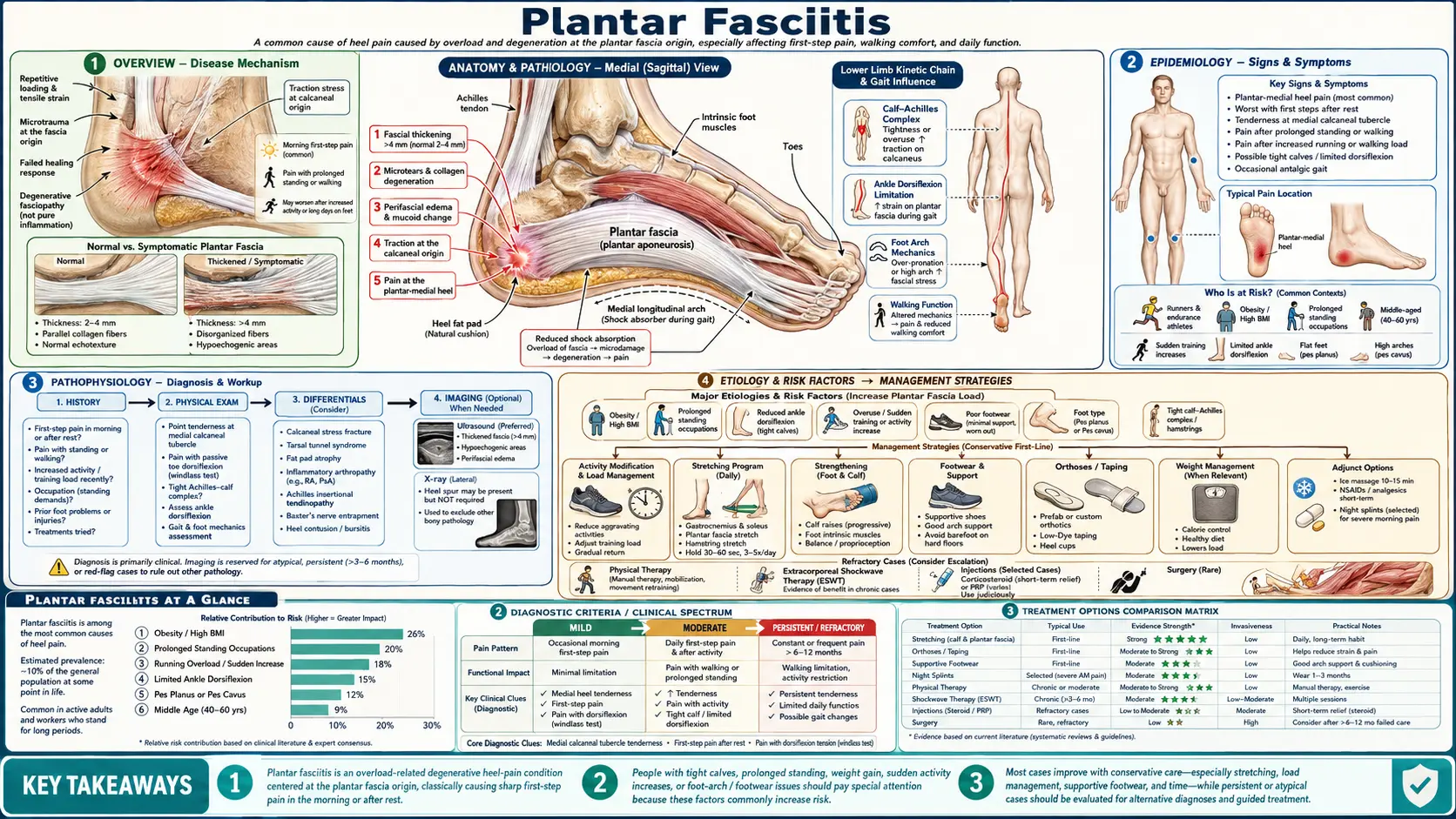
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- Diagnosis
- Treatment
- Complications
- Prognosis
- Prevention
- Recent Research and Advances
- References & Research
- Research Papers
- Connections
- Featured Videos
1. Overview
If your first few steps out of bed in the morning feel like stepping on a tack, a bruise, or a knife buried in your heel — and then it eases off after you hobble around for a few minutes — there is a very good chance you have plantar fasciitis. It is the single most common cause of heel pain, and it is one of the most common complaints that bring people to foot and ankle clinics. You are not imagining it, you are not being dramatic, and you have not done anything foolish to deserve it. This is an ordinary, well-understood condition that happens to millions of ordinary people.
The plantar fascia is a thick, fibrous band of connective tissue that runs along the sole of your foot, fanning out from the bottom of your heel bone (the calcaneus) forward to the base of your toes. Think of it as a tough, slightly elastic bowstring that supports the arch of your foot and absorbs shock with every step. Plantar fasciitis is what happens when the spot where that band attaches to the heel bone becomes damaged and irritated — usually from being overloaded, over and over, for longer than the tissue can repair itself.
Here is the most important thing to know up front, and we will come back to it: plantar fasciitis is stubborn but almost always self-limiting. Roughly 90% of people get better with simple, non-surgical care, though it commonly takes six to twelve months. That timeline is frustrating, and nobody likes hearing it, but it also means you are very unlikely to need injections, shockwave machines, or surgery. The slow, boring treatments — stretching, better shoes, patience — are the ones that actually work for most people.
2. Epidemiology
Plantar fasciitis is extraordinarily common. The frequently cited estimate is that about 1 in 10 people will develop it at some point in their lifetime, and in the United States it accounts for roughly 2 million patients treated per year, making it the most common cause of heel pain seen in clinical practice.
It affects people across the spectrum, but a few patterns stand out:
- Middle age. Peak incidence falls between the ages of about 40 and 60. The plantar fascia loses some of its elasticity and resilience over the decades, so the same load that a younger foot shrugged off can become an injury.
- Two very different at-risk groups. Runners and athletes get it from high, repetitive loads; sedentary people who are overweight or who stand all day get it from sustained, lower-grade loads. Plantar fasciitis is one of the few conditions that targets both the very active and the very inactive.
- Occupation matters. People whose jobs keep them on hard floors for hours — nurses, factory workers, teachers, retail and warehouse staff, cooks — carry a meaningfully higher risk.
- It is usually one foot, but not always. About a third of cases involve both heels, which can be a clue that a whole-body factor (weight, tight calves, an inflammatory condition) is at work rather than a one-off injury.
3. Pathophysiology
The name plantar fasciitis ends in "-itis," the medical suffix for inflammation, and for most of the twentieth century that is exactly how doctors thought of it — an inflamed band of tissue. That picture turned out to be largely wrong, and the correction matters for how the condition is treated.
When researchers actually examined plantar fascia tissue taken from people with chronic heel pain — most influentially in a 2003 study by Lemont and colleagues — they found very little classic inflammation. What they found instead was degeneration: disorganized, frayed collagen fibers, microscopic tears, abnormal new blood-vessel growth, and a failed, incomplete healing response. The tissue was not so much "inflamed" as worn out and badly repaired. For this reason many specialists now prefer the term plantar fasciosis (the "-osis" suffix meaning degeneration rather than inflammation).
Why does this distinction matter to you, the patient? Because if the problem were simple inflammation, anti-inflammatory drugs and cortisone would cure it — and they do not, at least not durably. The real problem is a tissue that needs to be re-loaded and rebuilt, gradually and correctly, which is exactly why stretching and graded loading are the cornerstone of effective treatment and why simply popping ibuprofen does not fix the underlying problem.
The damage concentrates at one specific spot: the origin of the plantar fascia on the inside-front edge of the heel bone (the medial calcaneal tubercle). This is the anchor point that takes the most strain when the fascia is stretched taut — which is why pressing on that exact spot reproduces the pain so reliably, and why morning is the worst time of day, as we will see next.
4. Etiology and Risk Factors
Plantar fasciitis is an overload injury: the tissue is asked to absorb more load, more often, than it can recover from. A large, careful case-control study by Riddle and colleagues (2003) pinned down the factors that most reliably raise the risk. The biggest three were limited ankle flexibility, obesity, and a lot of time on your feet.
- Tight calf muscles and Achilles tendon. This is the single most consistent and most fixable risk factor. A tight calf limits how far your ankle can flex upward, which forces the foot to compensate by overloading the plantar fascia with every step. The good news: it responds directly to stretching.
- Higher body weight (elevated BMI). Obesity is one of the strongest risk factors in non-athletes — every extra pound is extra load on the heel, many thousands of times a day. (See Obesity.)
- Jobs that keep you standing. Prolonged weight-bearing on hard surfaces — especially in unsupportive shoes — is a major occupational driver.
- Running and sudden activity increases. Distance running is a classic athletic cause. The trigger is very often a sudden jump in training: a new exercise program, a marathon build-up, a recent return to activity. The fascia can adapt to load, but only if the load increases slowly.
- Foot shape — both extremes. Flat feet (over-pronation) overstretch the fascia; high, rigid arches absorb shock poorly and concentrate stress on the heel. Either end of the spectrum raises risk.
- Unsupportive or worn-out footwear. Flimsy flats, old running shoes with collapsed cushioning, and going barefoot on hard floors all remove the support the arch relies on.
Heel spurs: usually a bystander, not the culprit
If an X-ray of your foot shows a heel spur — a small bony hook on the underside of the heel bone — you may be told, or may assume, that the spur is "stabbing" your fascia and causing the pain. This is one of the most persistent myths in foot care, and it is generally false.
The evidence is clear in both directions: plenty of people have heel spurs and no pain whatsoever (spurs are common incidental findings on X-rays of pain-free feet), and plenty of people have severe plantar fasciitis and no spur at all. The spur is best understood as a marker of long-standing strain at the heel — a bony response that forms over time, often after the fascia trouble began — rather than the cause of the pain. It points sideways into the muscle, not down into the fascia. The practical takeaway: removing a heel spur surgically is almost never the answer, and finding one on an X-ray should not change your treatment plan.
5. Clinical Presentation
Plantar fasciitis has a story so characteristic that an experienced clinician can often be confident of the diagnosis from the history alone, before even touching your foot. Here is that story — see how much of it matches yours:
- Sharp, stabbing pain in the bottom of the heel — usually toward the inner side, at the front edge of the heel pad where the fascia anchors.
- The first-step phenomenon. This is the signature, nearly diagnostic feature. The pain is at its absolute worst with the very first steps in the morning, or after you have been sitting for a while and then stand up. Those first few steps can be excruciating.
- It eases as you get going. After you walk around for a few minutes, the pain noticeably loosens up and fades — the fascia "warms up" and stretches out.
- It returns late in the day. After a long day of being on your feet, the ache creeps back, now from cumulative load rather than stiffness.
Why does rest make it worse, when rest helps almost every other injury? Because while you sleep (or sit), the foot relaxes into a pointed-toe position and the damaged fascia shortens and partly heals in that shortened state. The first step in the morning suddenly yanks that tight, fragile tissue to full length, re-tearing the tiny new repairs — hence the morning agony. This is also exactly why night splints, which hold the foot in a gently stretched position overnight, can help.
The pain is usually a gradual onset over weeks, not a sudden injury. A sudden, sharp "pop" or tearing sensation followed by bruising and swelling is a different and more serious event — a possible plantar fascia rupture — covered under Complications below.
6. Diagnosis
Plantar fasciitis is a clinical diagnosis. In the great majority of cases it is made from the history above plus a brief, simple physical exam — no scans or blood tests are needed. This is worth emphasizing because patients sometimes feel short-changed by not getting an X-ray or MRI; in straightforward cases, imaging adds cost and anxiety without changing the plan.
The exam looks for two findings:
- Point tenderness at the heel. Firm pressure on the inside-front corner of the heel bone (the fascia's origin) reproduces the patient's exact pain. Pinpoint tenderness right there is the classic sign.
- The windlass test. The examiner extends (pulls back) the big toe while the foot is loaded. This tightens the plantar fascia like winding a windlass and, in plantar fasciitis, recreates the heel pain.
When imaging is worth doing: only for atypical presentations or pain that has not improved despite several months of good conservative treatment. In those cases:
- Ultrasound can measure the thickness of the plantar fascia (a thickened fascia, generally over about 4–5 mm, supports the diagnosis) and is cheap and radiation-free.
- X-ray is not used to diagnose plantar fasciitis — remember the spur is a bystander — but can rule out a stress fracture of the heel.
- MRI is reserved for the few cases needing surgery or where the diagnosis is genuinely unclear.
The exam should also rule out a handful of mimics: a calcaneal stress fracture (squeeze-tenderness across the whole heel, not one point), fat-pad atrophy (deep central heel ache in older or thin-padded heels), tarsal tunnel syndrome (nerve pain with tingling and burning), and inflammatory arthritis — particularly if both heels hurt and there are other joint or back symptoms (see Connections).
7. Treatment
The single most encouraging fact about treatment is this: the cheap, simple, do-it-at-home measures are also the evidence-based first-line measures. You do not have to escalate to anything dramatic for the odds to be strongly in your favor. The clinical practice guidelines from the American Physical Therapy Association (Koc and colleagues, 2023) put stretching, manual therapy, and orthoses at the front of the line.
First-line: the things that actually fix it
- Stretching — the cornerstone. Two stretches matter most:
- Calf stretches (gastrocnemius and soleus), because tight calves are the biggest fixable cause.
- The plantar-fascia-specific stretch. In a landmark trial, DiGiovanni and colleagues (2003) showed that a stretch done by crossing the affected leg over the other knee and pulling the toes back with the hand — directly tensioning the fascia — outperformed the standard calf-only stretch. At two-year follow-up (DiGiovanni 2006), the fascia-specific group was still doing better. Do it several times a day, especially before that first morning step.
- Supportive shoes and orthoses. Wear cushioned, arch-supporting shoes; stop going barefoot on hard floors. Heel cushions or arch supports help. An important and honest point: inexpensive prefabricated (off-the-shelf) orthoses work about as well as expensive custom ones for most people. Landorf and colleagues (2006) found orthoses gave modest short-term benefit, and a 2018 review (Rasenberg) confirmed custom devices are not clearly superior to prefabricated. Start with an over-the-counter insert before paying for a custom mold.
- Night splints. A brace worn while you sleep holds the foot in a gentle stretch so the fascia heals at length, blunting the dreaded first step. Probe and colleagues (1999) and other trials support them; they are most useful for stubborn, long-standing cases — though some people find them awkward to sleep in.
- Activity modification and load management. You do not have to stop moving — in fact total rest can stiffen things — but back off the aggravating load (cut running mileage, switch temporarily to cycling or swimming) and rebuild gradually. This is a re-loading injury, so the goal is smarter load, not no load.
- NSAIDs — short term only. Ibuprofen or naproxen can take the edge off for a couple of weeks and help you tolerate stretching. But remember the tissue is degenerative, not inflamed, so anti-inflammatories manage symptoms, they do not cure the condition — do not rely on them long term.
- Ice and rolling. Rolling the arch over a frozen water bottle or a chilled golf/tennis ball for a few minutes gives both a stretch and a soothing cold massage — cheap, safe, and genuinely helpful for flare-ups.
Second-line: for the minority who do not improve
Most people never need these. They are options for pain that persists despite several months of diligent first-line care.
- Corticosteroid (cortisone) injection. A steroid injected at the heel can give real, but short-lived, relief. McMillan and colleagues (2012), in an ultrasound-guided randomized trial, found benefit at four weeks that had largely faded by three months. Two honest cautions: the relief usually does not last, and there is a small but real risk of rupturing the plantar fascia or thinning the protective heel fat pad, especially with repeated injections. Use sparingly.
- Extracorporeal shockwave therapy (ESWT). Acoustic pulses are delivered to the heel to stimulate healing in the degenerated tissue. The evidence is reasonably good — Gollwitzer and colleagues (2015) showed benefit over placebo in a multicenter randomized trial, and network meta-analyses (Babatunde 2018) rank it among the more effective options. It is non-invasive and worth considering before surgery.
- Platelet-rich plasma (PRP). An injection of a concentrate from your own blood, intended to spur repair. The evidence is genuinely mixed — some trials (Monto 2014) suggest it lasts longer than cortisone, others show no clear advantage. We will be honest: PRP is promising but not yet proven, and it is often expensive and not covered by insurance. Treat it as experimental.
Surgery — rarely needed
Surgery (a plantar fascia release, sometimes with calf-muscle lengthening) is reserved for the small minority — on the order of 5% or fewer — whose disabling pain persists despite a full 6–12 months of thorough conservative treatment. It can help, but it carries risks (nerve irritation, flattening of the arch, slow recovery), so it sits at the very end of the line. The overwhelming message is that the great majority of people heal without ever entering an operating room.
8. Complications
Plantar fasciitis is not a dangerous condition, but a few complications are worth knowing about:
- Chronic heel pain and changed gait. The most common "complication" is simply that it drags on, and that the limping you adopt to protect the heel throws extra stress onto the other foot, the knees, the hips, and the lower back — sometimes creating new aches. Treating the heel and walking as normally as tolerated helps prevent this cascade.
- Plantar fascia rupture. A full tear of the fascia is uncommon but important. It usually announces itself with a sudden "pop" or tearing sensation, sharp pain, swelling, and bruising along the arch — quite different from the slow morning ache of ordinary plantar fasciitis. The two biggest risk factors are repeated cortisone injections and pushing hard through pain. A rupture often needs a period of immobilization and a slower, more careful rehabilitation.
- Deconditioning. Months of reduced activity can lead to weight gain and loss of fitness, which in turn worsen the very risk factors that caused the problem — a frustrating loop. Low-impact cross-training (cycling, swimming, pool walking) breaks it.
9. Prognosis
Here is the reassurance, stated plainly: the long-term outlook for plantar fasciitis is excellent. Around 90% of people recover fully with simple conservative care, and only a small fraction ever need injections, shockwave, or surgery.
The honest catch is the timeline. Recovery is typically measured in months, not days or weeks — commonly six to twelve months for the pain to settle completely. This is genuinely the hardest part for most patients, because the slowness feels like the treatment is not working. It is not a sign of failure; it is simply how this degenerative tissue heals. Setting that expectation up front prevents people from abandoning the stretches that are, in fact, slowly fixing them, or chasing aggressive interventions out of impatience.
The people who do best are the ones who treat it like the marathon it is: consistent daily stretching, sensible shoes, weight management, and patience. Flare-ups can happen for years afterward, usually triggered by a sudden activity spike or a return to bad footwear — and they respond to the same simple measures.
10. Prevention
Because plantar fasciitis is an overload injury, prevention comes down to keeping the load on the fascia within what it can handle. If you have had it once, these habits also cut your chance of a recurrence:
- Stretch your calves and feet regularly. Keeping the calf and Achilles supple is the highest-yield prevention there is, because calf tightness is the most common driver. A daily wall calf stretch and the plantar-fascia stretch go a long way.
- Wear supportive footwear. Choose shoes with good arch support and cushioning for the surfaces and hours you spend on your feet; avoid long stretches barefoot on hard floors and worn-flat flip-flops.
- Increase activity gradually. Build running mileage and new exercise programs slowly — the common "10% per week" rule of thumb — so the fascia has time to adapt. Most cases trace back to doing too much, too soon.
- Manage your weight. Reducing body weight directly lowers the load on the heel with every step (see Obesity).
- Replace worn-out shoes. Cushioning and support break down with miles even when the shoe still looks fine. Running shoes are usually past their prime by around 300–500 miles; replace them before the support is gone.
11. Recent Research and Advances
Plantar fasciitis is far from a closed book, and current research is refining how it is understood and treated:
- The shift to "fasciosis." The reframing from an inflammatory to a degenerative model (building on Lemont 2003) continues to reshape treatment, steering the field away from cortisone-as-cure and toward graded loading and tissue-stimulating therapies.
- Load-based and strengthening exercise. Beyond passive stretching, there is growing interest in high-load progressive strengthening of the foot and calf (for example, heel raises performed with the toes propped up to load the fascia). Early trials suggest it may speed recovery for some patients — treating the fascia more like a tendon that needs rebuilding than a tissue that needs rest.
- Comparative-effectiveness evidence. Network meta-analyses such as Babatunde and colleagues (2018) now let clinicians and patients see how stretching, orthoses, injections, and shockwave stack up against each other, rather than against placebo alone — supporting a stepwise, conservative-first approach.
- Biologics under scrutiny. PRP and related injectable therapies remain under active, and appropriately skeptical, study. The honest current verdict is "promising but unproven," and patients are best served by clear-eyed expectations rather than hype.
- Updated practice guidelines. The 2023 revision of the heel-pain clinical practice guidelines (Koc and colleagues) consolidates the strongest evidence and reaffirms stretching, manual therapy, taping, and orthoses as first-line care — reassuring confirmation that the simple measures are the right ones.
12. References & Research
Historical Background
Heel pain has been described for as long as medicine has been written down, and "policeman's heel" was a common nineteenth- and twentieth-century name for it, reflecting its association with long hours on the feet. For most of the modern era the condition was understood as an inflammation of the plantar fascia — the very name encodes that assumption. The pivotal conceptual shift came in 2003, when Lemont and colleagues examined the actual tissue and found degeneration rather than inflammation, prompting many specialists to re-christen the condition plantar fasciosis. The same early-2000s period produced the modern evidence base for treatment: DiGiovanni's plantar-fascia-specific stretching trials (2003, 2006), Riddle's risk-factor study (2003), and the maturation of extracorporeal shockwave therapy as a non-surgical option — together moving care decisively toward conservative, loading-based management.
Key Research Papers
- Buchbinder R. Plantar Fasciitis. New England Journal of Medicine. 2004;350(21):2159–2166.
- DiGiovanni BF, Nawoczenski DA, Lintal ME, et al. Tissue-Specific Plantar Fascia-Stretching Exercise Enhances Outcomes in Patients With Chronic Heel Pain. Journal of Bone and Joint Surgery (American). 2003;85(7):1270–1277.
- DiGiovanni BF, Nawoczenski DA, Malay DP, et al. Plantar Fascia-Specific Stretching Exercise Improves Outcomes in Patients With Chronic Plantar Fasciitis (Two-Year Follow-up). Journal of Bone and Joint Surgery (American). 2006;88(8):1775–1781.
- Riddle DL, Pulisic M, Pidcoe P, et al. Risk Factors for Plantar Fasciitis: A Matched Case-Control Study. Journal of Bone and Joint Surgery (American). 2003;85(5):872–877.
- Lemont H, Ammirati KM, Usen N. Plantar Fasciitis: A Degenerative Process (Fasciosis) Without Inflammation. Journal of the American Podiatric Medical Association. 2003;93(3):234–237.
- Landorf KB, Keenan AM, Herbert RD. Effectiveness of Foot Orthoses to Treat Plantar Fasciitis: A Randomized Trial. Archives of Internal Medicine. 2006;166(12):1305–1310.
- McMillan AM, Landorf KB, Gilheany MF, et al. Ultrasound Guided Corticosteroid Injection for Plantar Fasciitis: Randomised Controlled Trial. BMJ. 2012;344:e3260.
- Probe RA, Baca M, Adams R, et al. Night Splint Treatment for Plantar Fasciitis: A Prospective Randomized Study. Clinical Orthopaedics and Related Research. 1999;368:190–195.
- Gollwitzer H, Saxena A, DiDomenico LA, et al. Clinically Relevant Effectiveness of Focused Extracorporeal Shock Wave Therapy in the Treatment of Chronic Plantar Fasciitis. Journal of Bone and Joint Surgery (American). 2015;97(9):701–708.
- Monto RR. Platelet-Rich Plasma Efficacy Versus Corticosteroid Injection Treatment for Chronic Severe Plantar Fasciitis. Foot & Ankle International. 2014;35(4):313–318.
- Babatunde OO, Legha A, Littlewood C, et al. Comparative Effectiveness of Treatment Options for Plantar Heel Pain: A Systematic Review With Network Meta-Analysis. British Journal of Sports Medicine. 2018;53(3):182–194.
- Koc TA, Bise CG, Neville C, et al. Heel Pain – Plantar Fasciitis: Revision 2023 Clinical Practice Guidelines. Journal of Orthopaedic & Sports Physical Therapy. 2023;53(12):CPG1–CPG39.
- Rasenberg N, Riel H, Rathleff MS, et al. Efficacy of Foot Orthoses for the Treatment of Plantar Heel Pain: A Systematic Review and Meta-Analysis. British Journal of Sports Medicine. 2018;52(16):1040–1046.
- Motley T. Plantar Fasciitis/Fasciosis. Clinics in Podiatric Medicine and Surgery. 2021;38(2):193–200.
Research Papers
The links below run live searches on PubMed, the U.S. National Library of Medicine's database of biomedical literature. Use them to explore the current evidence on plantar fasciitis — its causes, diagnosis, and the full range of treatments — and to find newer studies as they are published.
- Plantar fasciitis treatment
- Plantar fasciitis stretching exercise
- Plantar fasciitis risk factors
- Plantar fasciosis degeneration
- Extracorporeal shockwave therapy for plantar fasciitis
- Corticosteroid injection for plantar fasciitis
- Foot orthoses for plantar heel pain
- Night splint for plantar fasciitis
- Platelet-rich plasma for plantar fasciitis
- Heel spur and plantar fasciitis
- Plantar fascia rupture
- Plantar fasciitis ultrasound diagnosis
Connections
- Tendinitis — the same overuse/degenerative mechanism in a tendon; the "fasciosis" model mirrors tendinosis.
- Sciatica — another cause of foot and lower-limb pain; nerve-related heel pain can mimic plantar fasciitis.
- Carpal Tunnel Syndrome — a comparable repetitive-load entrapment/overuse problem in the wrist.
- Herniated Disc — a spinal cause of radiating leg and foot pain to distinguish from heel-local pain.
- Fibromyalgia — widespread pain and tenderness that can complicate or coexist with localized heel pain.
- Osteoarthritis — degenerative joint disease; foot and ankle OA can accompany chronic heel problems.
- Gout — a cause of sudden, severe foot pain to consider when heel/foot pain is atypical or red and hot.
- Ankylosing Spondylitis — inflammatory enthesitis classically causes heel pain; suspect it when both heels hurt with back symptoms.
- Rheumatoid Arthritis — inflammatory arthritis that can produce foot pain and bilateral heel involvement.
- Obesity — one of the strongest modifiable risk factors; extra weight loads the heel with every step.
- Chronic Pain — the persistent, months-long course of plantar fasciitis can feed broader chronic-pain patterns.
- Diabetes — affects foot health, healing, and nerve sensation, complicating foot pain and footwear choices.
- Orthopedics — the full list of musculoskeletal conditions on this site.
- All Conditions — browse every disease and condition covered on myhealthcare.com.