Bipolar Disorder
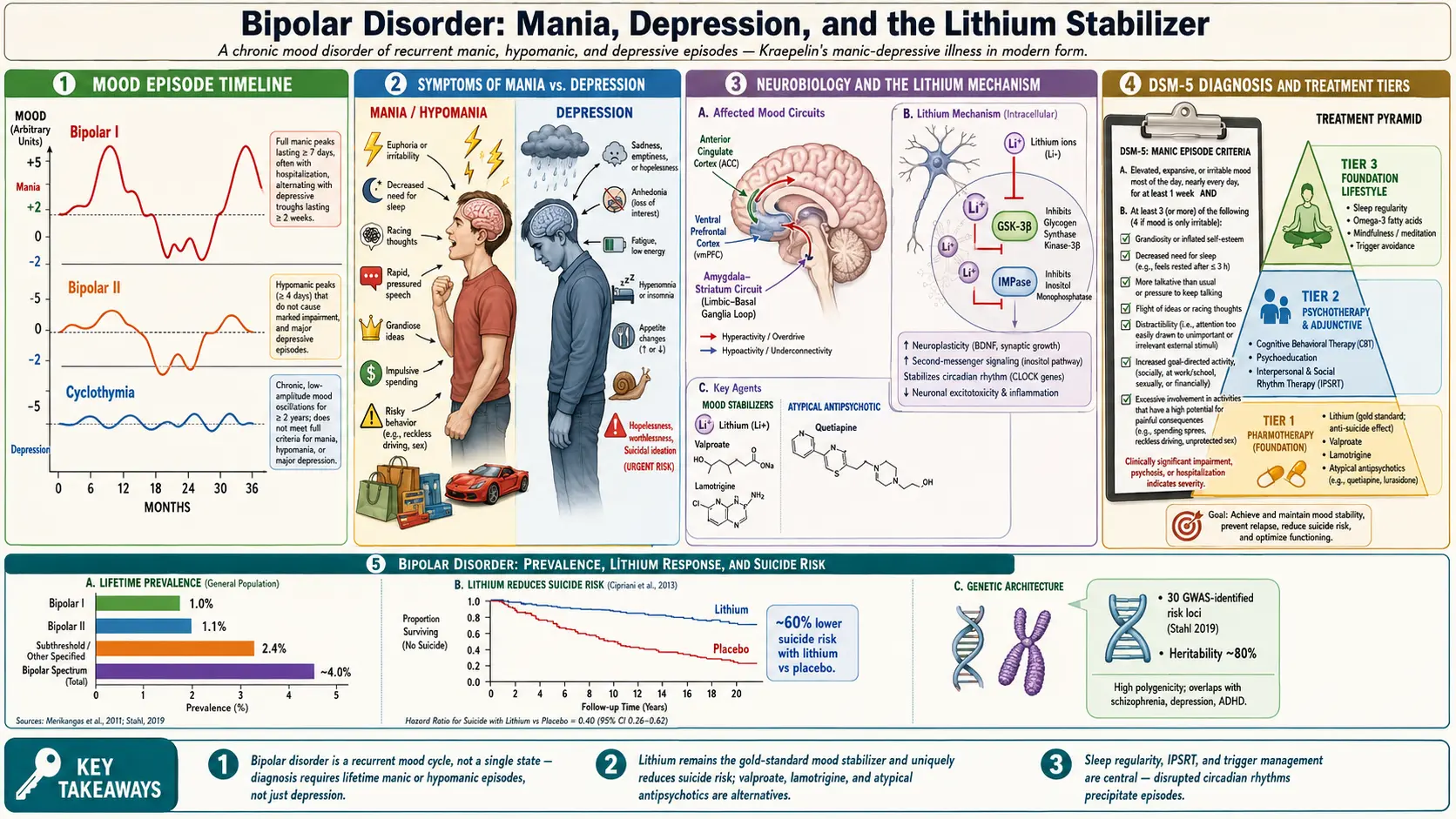
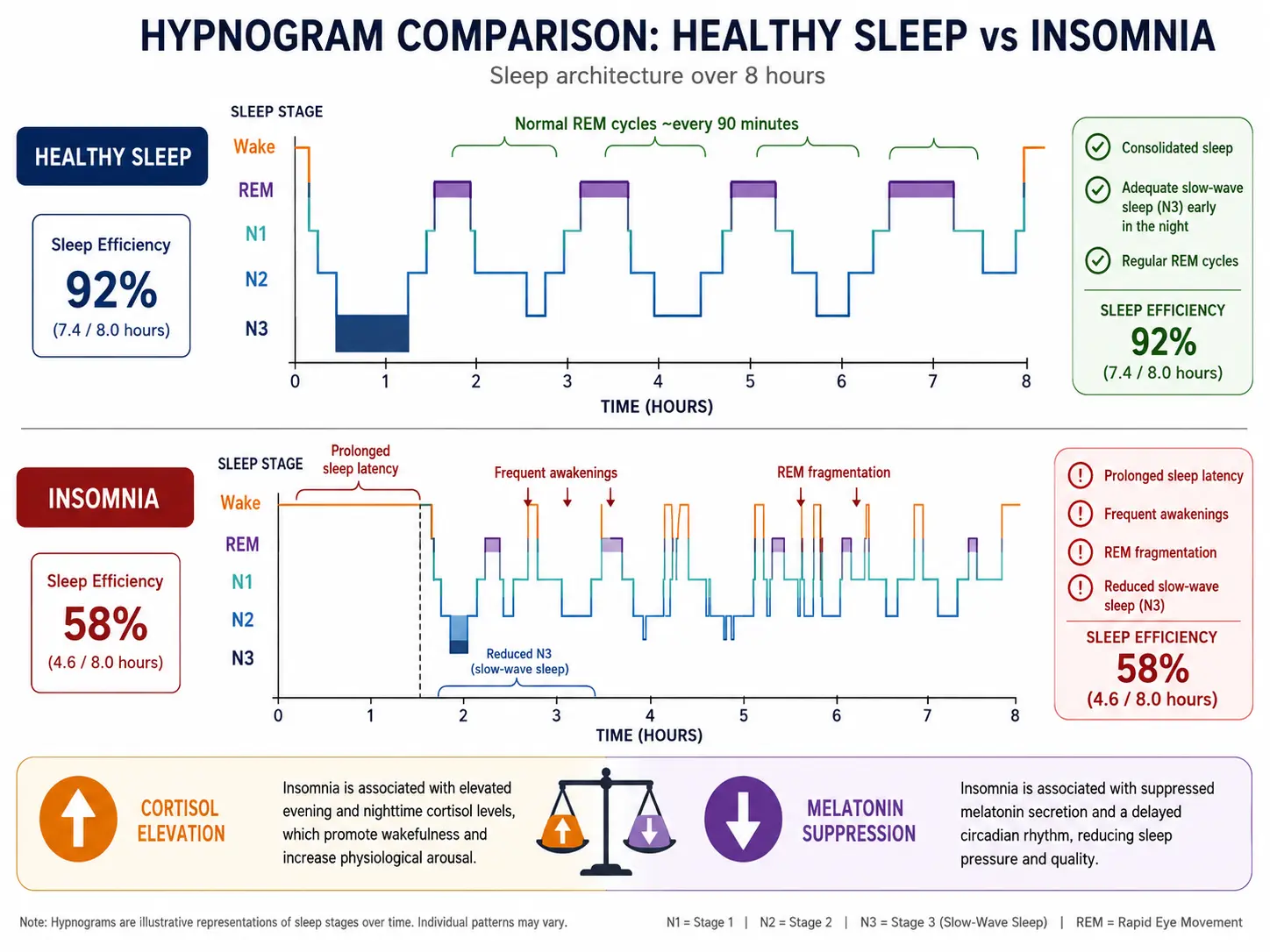
Table of Contents
- What is Bipolar Disorder?
- Bipolar I, II, and Cyclothymia
- DIGFAST: Manic Episode Criteria
- Mixed Features and Dysphoric Mania
- Kindling Hypothesis
- Pharmacotherapy — Mood Stabilizers
- Atypical Antipsychotics in Bipolar
- Antidepressant Cautions and STEP-BD
- Psychotherapy and Lifestyle
- Complications and Comorbidities
- Research Papers
- Connections
- Featured Videos
What is Bipolar Disorder?
Bipolar disorder is a chronic, episodic mood disorder characterized by abnormal swings in energy, activity, sleep, and behavior — ranging from euphoric or irritable highs (mania or hypomania) to devastating lows (major depression). It affects approximately 2–3% of the global population across its full spectrum and ranks among the leading causes of disability worldwide. Unlike ordinary mood variability, bipolar episodes are sustained, functionally impairing, and often require long-term pharmacological management.
The disorder typically emerges in late adolescence or early adulthood, with a mean age of onset around 20–25 years. Bipolar disorder carries a substantially elevated risk of suicide — lifetime rates of completed suicide are estimated at 10–15 times higher than the general population — making accurate diagnosis and aggressive treatment essential, not optional.
Neurobiologically, bipolar disorder involves dysregulation of limbic circuits, circadian rhythm machinery, and monoamine neurotransmitter systems (dopamine, serotonin, norepinephrine). Mitochondrial dysfunction, neuroinflammation, oxidative stress, and HPA-axis hyperreactivity all appear to contribute. Genome-wide association studies have identified shared genetic architecture with schizophrenia, major depression, and ADHD, underscoring the overlapping biology of psychiatric illness.
Bipolar I, II, and Cyclothymia — Differential Diagnosis
Distinguishing the three main subtypes is clinically critical because treatment strategy differs substantially between them.
Bipolar I Disorder
Lifetime prevalence approximately 1%. Bipolar I is defined by the presence of at least one manic episode lasting a minimum of 7 days (or any duration if hospitalization is required). The manic episode must represent a noticeable change from baseline and be present for most of the day, nearly every day. Depressive episodes are common but not required for the diagnosis. Psychotic features (delusions, hallucinations) may accompany severe manic episodes. Bipolar I is the most severe subtype and the one most associated with hospitalization and legal consequences during manic breaks.
Bipolar II Disorder
Lifetime prevalence approximately 1%. Bipolar II is defined by a history of at least one hypomanic episode (minimum 4 consecutive days) and at least one major depressive episode. Crucially, there has never been a full manic episode — if mania occurs, the diagnosis becomes Bipolar I. Hypomania is a distinct, elevated or irritable mood that is observable to others but is not severe enough to cause marked impairment or require hospitalization, and it does not include psychotic features. Bipolar II is frequently misdiagnosed as unipolar depression because patients seek help during the depressive phase and may not identify or report hypomanic periods as pathological. The depressive burden in BD-II often exceeds that of BD-I in terms of episode frequency and time spent depressed.
Cyclothymic Disorder (Cyclothymia)
Cyclothymia is a chronic, fluctuating mood disturbance characterized by numerous periods of hypomanic symptoms and periods of depressive symptoms that persist for at least 2 years (1 year in children and adolescents). Critically, the individual has not met criteria for a full hypomanic or major depressive episode during this period. Cyclothymia is a genuine disorder — not a mild personality quirk — and carries a 15–50% risk of eventually evolving into Bipolar I or II. Mood never stabilizes for more than 2 months during the qualifying period.
Other Specified and Unspecified Bipolar Disorders
This category captures presentations that cause clinically significant distress or impairment but do not meet full criteria — for example, short-duration hypomanic episodes (2–3 days instead of 4), or hypomanic episodes with insufficient symptoms. Bipolar disorder due to another medical condition (e.g., thyroid disease, Cushing syndrome, TBI) and substance/medication-induced bipolar disorder round out the diagnostic category.
Rapid Cycling Specifier
Four or more distinct mood episodes in a 12-month period, applicable to both BD-I and BD-II. Rapid cycling is associated with worse prognosis, greater depressive burden, and relative resistance to lithium. Valproate and lamotrigine are preferred. Thyroid function should be checked, as subclinical hypothyroidism drives rapid cycling in a significant minority.
DIGFAST — DSM-5 Manic Episode Criteria
The DSM-5 manic episode requires a distinct period of abnormally and persistently elevated, expansive, or irritable mood and abnormally and persistently increased goal-directed activity or energy, lasting at least 1 week and present most of the day, nearly every day. During this period, three or more of the following symptoms must be present to a significant degree (four if mood is only irritable). The DIGFAST mnemonic covers all seven:
- D — Distractibility: Attention is too easily drawn to unimportant or irrelevant external stimuli. Patients report being unable to focus; observers note they are easily sidetracked mid-sentence. Clinically distinct from ADHD distractibility by its episodic, mood-concordant onset.
- I — Impulsivity / Irresponsibility: Increased involvement in activities with a high potential for painful consequences — unrestrained buying sprees, sexual indiscretions, foolish business investments, reckless driving. The person lacks usual inhibitory judgment. This is the dimension most likely to result in legal trouble, financial ruin, or STI exposure.
- G — Grandiosity: Inflated self-esteem or grandiosity — can range from uncritical self-confidence (mild) to frank delusions of special powers, identity, or mission (severe). "I don't need sleep because I've been chosen to solve climate change" is a grandiose delusion. Distinct from healthy confidence by its ego-syntonic, mood-driven character and resistance to reality-testing.
- F — Flight of Ideas: Racing thoughts; nearly continuous flow of accelerated speech with abrupt topic changes. The patient may experience this as creativity or brilliance. Clinically, thoughts race faster than they can be verbalized, leading to derailment and tangential speech. Different from circumstantial thinking by the speed and subjective experience of acceleration.
- A — Activity Increase: Increased goal-directed activity (social, at work, school, or sexually) or psychomotor agitation. Projects multiply. The person starts multiple ambitious endeavors simultaneously. Psychomotor agitation — purposeless activity — is more prominent in dysphoric mania.
- S — Sleep Decreased: Decreased need for sleep — importantly, the patient feels rested after only 3 hours of sleep and does not experience daytime fatigue. This is distinct from insomnia (where the patient wants to sleep but cannot). Reduced sleep need often precedes and predicts manic relapse; sleep deprivation can also precipitate mania in vulnerable individuals.
- T — Talkativeness / Pressured Speech: More talkative than usual or pressure to keep talking. Speech is rapid, loud, difficult to interrupt. The person may talk over others, continue talking even when no one is listening, or be so verbose that conversation becomes impossible. Severe pressured speech can render an interview non-productive.
The full manic episode must cause marked impairment in social or occupational functioning, necessitate hospitalization to prevent harm, or include psychotic features. If symptoms are sufficient for mania but clearly due to substances or medications, the diagnosis shifts to substance/medication-induced bipolar disorder — but antidepressant-induced mania that persists beyond the physiological effect of the drug does count toward a BD-I diagnosis per DSM-5.
Mixed Features Specifier — Dysphoric Mania and Mixed Episodes
The DSM-5 replaced the older "mixed episode" category with a "mixed features" specifier that can be applied to manic, hypomanic, or depressive episodes. This change reflects the dimensional reality of bipolar disorder: many patients experience simultaneous depressive and manic symptoms rather than clean alternating episodes.
Mixed Features During a Manic/Hypomanic Episode
At least 3 depressive symptoms are present during the episode: dysphoric mood (prominent sadness or emptiness), diminished interest or pleasure, psychomotor slowing (contrasting with the overall elevated energy), fatigue, feelings of worthlessness or excessive guilt, or recurrent thoughts of death. This is sometimes called "dysphoric mania" — the patient has the energy and insomnia of mania combined with the suffering, hopelessness, and suicidal ideation of depression. This combination is particularly dangerous: the energy to act on suicidal impulses is present, unlike in retarded depression where the patient may be too slowed to carry out a plan.
Mixed Features During a Depressive Episode
At least 3 manic/hypomanic symptoms are present: elevated or expansive mood, inflated self-esteem, increased talkativeness, flight of ideas or racing thoughts, increased energy, decreased sleep need, or impulsive behavior. This presentation often goes unrecognized when a clinician focuses only on the depression and misses the hypomanic undercurrents.
Clinical Implications
Mixed features predict a worse prognosis, higher suicide risk, more frequent episodes, and more rapid cycling. Antidepressant monotherapy is contraindicated. Valproate is particularly effective for mixed states. Quetiapine and cariprazine have demonstrated efficacy. Lithium is less effective than for classic euphoric mania in mixed presentations.
The Kindling Hypothesis — Episode Sensitization
The kindling hypothesis, most systematically articulated by Robert M. Post and colleagues beginning in the late 1980s and formalized in 1992, proposes that repeated mood episodes progressively lower the threshold required to trigger subsequent episodes. Like neurological kindling — where repeated subthreshold electrical stimuli eventually produce spontaneous seizures — bipolar episodes appear to self-perpetuate over time, becoming increasingly autonomous of external stressors.
Key Observations
- Early episodes are often stress-precipitated — identifiable psychosocial stressors (bereavement, job loss, relationship breakdown) commonly precede the first two to three episodes.
- Later episodes become autonomous — as the disorder progresses, episodes occur without discernible precipitants. The nervous system has been "kindled" into a state of sustained vulnerability.
- Cycle acceleration — on average, the inter-episode interval shortens over the course of the illness. Early in the disorder, episodes may be years apart; by the third decade of illness, many patients experience multiple episodes annually or continuous cycling.
- Cross-sensitization — stress hormones (particularly cortisol) and stimulant exposure can also accelerate kindling, explaining why cocaine use and severe life stressors hasten illness progression.
Molecular Substrates
Post's group proposed that kindling involves progressive gene expression changes in limbic circuits — altered immediate-early gene (c-fos, c-jun) induction, synaptic remodeling, and changes in BDNF signaling. Repeated episodes are associated with progressive hippocampal volume loss on neuroimaging, consistent with glucocorticoid-mediated neurotoxicity during severe mood episodes.
Clinical Implications for Early Treatment
The kindling model carries a powerful clinical imperative: the best time to treat bipolar disorder aggressively is early in its course. Every untreated or undertreated episode may permanently lower the threshold for the next. Early, sustained mood stabilizer treatment — even between episodes — is not just about preventing the current crisis; it is neuroprotective in the literal sense. This is why maintenance therapy is recommended indefinitely after a second manic episode, and often after the first if risk factors are present.
Pharmacotherapy — Mood Stabilizers in Depth
The pharmacological management of bipolar disorder is more complex than any other psychiatric condition, requiring differentiated approaches for acute mania, acute depression, maintenance, and rapid cycling. No single agent covers all phases optimally.
Lithium — The Gold Standard
Lithium remains the only medication with robust evidence for antisuicidal efficacy independent of its mood-stabilizing effect. It is first-line for classic euphoric mania (BD-I, not mixed), long-term maintenance, and suicide prevention. Discovered as a mood stabilizer by Australian psychiatrist John Cade in 1949, it has more randomized controlled trial evidence than any other mood stabilizer.
Therapeutic index: Narrow. Serum levels must be monitored routinely.
- Acute mania: target 0.8–1.2 mEq/L
- Maintenance: target 0.6–1.0 mEq/L (lower end acceptable for tolerability)
- Toxicity threshold: levels above 1.5 mEq/L carry significant risk
Monitoring requirements:
- Renal function (GFR and creatinine) — every 6 months in stable patients; more frequently after dose changes or intercurrent illness. Lithium causes nephrogenic diabetes insipidus (polyuria/polydipsia) in up to 40% and can cause progressive tubulointerstitial nephropathy with long-term use.
- Thyroid (TSH) — every 6–12 months. Lithium inhibits thyroid hormone release; hypothyroidism occurs in up to 40% of long-term users. Subclinical hypothyroidism drives rapid cycling.
- Calcium and PTH — annually. Lithium promotes parathyroid cell proliferation; hypercalcemia from primary hyperparathyroidism occurs in approximately 10% of patients after 10+ years of treatment.
- Sodium and fluid intake — dietary sodium depletion (low-sodium diets, excessive sweating, fever, diarrhea) dramatically increases lithium reabsorption and can precipitate toxicity. NSAIDs and ACE inhibitors raise lithium levels dangerously; patients must be counseled about this interaction.
Toxicity signs: At levels above 1.5 mEq/L — coarse tremor, nausea, vomiting, diarrhea, confusion, ataxia. Above 2.0 mEq/L — seizures, cardiac arrhythmias, irreversible cerebellar damage. Treatment: hydration, dialysis for severe toxicity.
Mechanism: Lithium inhibits inositol monophosphatase and GSK-3 beta, modulates BDNF signaling, and stabilizes circadian rhythm gene expression (CRY/PER clock genes). It is one of the few psychiatric medications with proven neuroprotective and possibly neurogenic properties at therapeutic doses.
Valproate (Divalproex Sodium)
Valproate (as divalproex sodium) is FDA-approved for acute mania and is particularly effective for mixed states and rapid cycling — two presentations where lithium is relatively less effective. It is a broad-spectrum anticonvulsant that enhances GABAergic transmission and inhibits sodium channels.
Critical safety concern — TERATOGENICITY: Valproate is subject to an FDA REMS (Risk Evaluation and Mitigation Strategy) program due to serious and well-documented fetal risks:
- Neural tube defects (spina bifida) — risk 1–2% compared to 0.06–0.07% background rate
- Congenital malformations (cardiac, craniofacial, limb abnormalities) — 2-3x increased risk
- Dose-dependent cognitive impairment in children exposed in utero — average IQ deficit of 7–10 points at age 6 compared to lamotrigine-exposed children
- Autism spectrum disorder risk approximately doubled in offspring
Valproate should not be used as first-line therapy in women of childbearing age unless other treatments have failed and reliable contraception is confirmed. All prescribers must enroll in the REMS program.
Monitoring: LFTs and CBC at baseline (rare hepatotoxicity and thrombocytopenia); serum valproate levels (therapeutic range 50–125 mcg/mL for acute mania); ammonia levels if encephalopathy is suspected (valproate-induced hyperammonemia can occur even with normal LFTs).
Key drug interaction: Valproate approximately doubles lamotrigine levels by inhibiting its glucuronidation. When combining the two, lamotrigine must be started at half the usual dose and titrated more slowly to avoid Stevens-Johnson syndrome.
Lamotrigine
Lamotrigine occupies a unique niche in bipolar pharmacotherapy: it is primarily effective for bipolar depression and maintenance, but has no meaningful efficacy for acute mania. It is first-line for BD-II (where depression predominates) and for maintenance prevention of depressive episodes in BD-I. The landmark Calabrese 2003 trial established its superiority over placebo in BD-I maintenance with particular strength in preventing depressive recurrence.
Stevens-Johnson Syndrome (SJS) risk: SJS is a rare but potentially life-threatening mucocutaneous hypersensitivity reaction (toxic epidermal necrolysis at the severe end). Risk is dose-escalation-dependent, not idiosyncratic — the vast majority of serious rashes occur when the titration protocol is violated or when valproate is co-prescribed without dose halving.
Mandatory slow titration protocol:
- Weeks 1–2: 25 mg/day
- Weeks 3–4: 50 mg/day
- Weeks 5–6: 100 mg/day
- Week 7 onward: 200 mg/day (target maintenance dose)
- If taking valproate: halve all doses above (start at 25 mg every other day)
Patients must be instructed to stop lamotrigine immediately and seek emergency care if any rash develops — benign maculopapular rashes also occur, but distinguishing them from early SJS requires clinical evaluation. Do not restart after discontinuation for rash without specialist guidance.
Mechanism: Inhibits voltage-gated sodium channels, reducing release of excitatory neurotransmitters (glutamate, aspartate). Its antidepressant mechanism is not fully understood but likely involves stabilization of hyper-active corticolimbic glutamatergic circuits.
Atypical Antipsychotics in Bipolar Disorder
Second-generation (atypical) antipsychotics have become central to bipolar pharmacotherapy across all phases. Their D2/D3 blockade addresses the dopaminergic excess of mania; some agents have additional mechanisms that address bipolar depression.
Quetiapine
Quetiapine is one of the most comprehensively studied agents in bipolar disorder, with FDA approval for acute mania, acute bipolar depression, and maintenance — the only agent approved for all three phases as monotherapy. The BOLDER I (McElroy 2004) and BOLDER II (Calabrese 2005) trials established quetiapine's efficacy for bipolar depression, demonstrating superiority over placebo on MADRS total scores at doses of 300 and 600 mg/day. The EMBOLDEN I and II trials extended these findings.
Quetiapine's antidepressant effect is thought to be mediated in part by its active metabolite norquetiapine, which acts as a norepinephrine reuptake inhibitor and has partial agonist activity at 5-HT1A receptors. This distinguishes it mechanistically from purely antidopaminergic agents.
Metabolic monitoring required: Quetiapine causes weight gain, dyslipidemia, and insulin resistance. Fasting glucose, HbA1c, lipid panel, and weight should be measured at baseline and every 3 months for the first year, then annually.
Cariprazine
Cariprazine (Vraylar) is FDA-approved for both acute manic/mixed episodes and bipolar I depression. As a dopamine D3/D2 partial agonist with high selectivity for D3 receptors, it has a distinct mechanism from quetiapine. D3 receptor modulation in mesolimbic circuits may underlie its antidepressant effect. The CANMAT 2018 guidelines list cariprazine as a first-line option for bipolar I depression, where effective treatments are particularly scarce. Metabolic adverse effects are generally milder than olanzapine or quetiapine. Akathisia is the most common reason for discontinuation.
Aripiprazole
Aripiprazole is FDA-approved for acute mania and maintenance in BD-I. As a partial D2/D3 agonist, it has a favorable metabolic profile compared to full antagonists. It is less sedating than quetiapine, which is an advantage in some patients and a disadvantage in those needing sedation during acute mania. Evidence for bipolar depression is weaker than for mania.
Olanzapine
Olanzapine is among the most potent agents for acute mania and has proven maintenance efficacy, but carries the highest metabolic burden of the atypical antipsychotics — clinically significant weight gain (averaging 4–6 kg in the first year), hyperglycemia, and dyslipidemia are common. The olanzapine-fluoxetine combination (Symbyax) is FDA-approved for bipolar I depression. Given its metabolic risks, olanzapine is typically reserved for patients who require potent acute control and for whom metabolic risk is acceptable, or as a third-line option when alternatives have failed.
First-Generation Antipsychotics (FGAs) — Risks in Bipolar
Haloperidol and other FGAs can manage acute mania effectively and are sometimes used in emergency settings. However, their use in bipolar disorder carries specific long-term risks:
- Tardive dyskinesia (TD) — involuntary repetitive movements (typically orofacial) from chronic D2 blockade; risk increases with cumulative exposure and may be irreversible
- Extrapyramidal symptoms (EPS) — acute dystonia, parkinsonism, akathisia — occurring at higher rates than with SGAs
- Depressive switch — FGAs may worsen or precipitate depressive episodes in bipolar patients, possibly via D2 blockade in mesocortical circuits
- Neuroleptic malignant syndrome (NMS) — rare but life-threatening; more common with FGAs than SGAs
For long-term bipolar management, SGAs are strongly preferred over FGAs. FGA use should be short-term and circumstance-driven (acute agitation, psychosis requiring rapid control, resource-limited settings).
Antidepressant Cautions and the STEP-BD Data
The use of antidepressants in bipolar disorder is one of the most contested areas in psychiatry. The risks are real and well-documented; the benefits, especially as monotherapy, are not.
The Manic Switch Risk
Antidepressant monotherapy in bipolar disorder — prescribing an antidepressant without a concurrent mood stabilizer — risks precipitating a manic or hypomanic episode, a phenomenon known as the manic switch. Tricyclic antidepressants carry the highest switch risk; SNRIs are intermediate; SSRIs and bupropion have lower but still real risks. Antidepressant-induced mania can be more severe and more difficult to treat than spontaneous mania.
STEP-BD Evidence
The Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD), a large NIMH-funded naturalistic study, provided pivotal data on antidepressant use in bipolar disorder. The landmark Sachs 2007 paper found that adjunctive antidepressant therapy (paroxetine or bupropion added to a mood stabilizer) was not more effective than mood stabilizer alone for treating bipolar depression. The manic switch rate was low when antidepressants were added to a mood stabilizer, but the lack of efficacy signal was striking — challenging the widespread clinical practice of adding antidepressants to mood stabilizers for bipolar depression.
Current Clinical Guidance
Based on STEP-BD and subsequent meta-analyses:
- Antidepressant monotherapy is contraindicated in bipolar disorder — any use should be accompanied by a mood stabilizer or atypical antipsychotic
- First-line treatments for bipolar depression should be quetiapine, cariprazine, lurasidone (FDA-approved for BD-I depression), or lamotrigine — not antidepressants
- If antidepressants are used (after failure of preferred agents), SSRIs or bupropion are preferred; tricyclics and venlafaxine carry higher switch risk
- Antidepressants should generally be discontinued after the depressive episode resolves rather than continued long-term
- The CANMAT 2018 guidelines designate antidepressants as third-line for bipolar I depression and second-line for bipolar II depression (where switch risk is lower)
Psychotherapy, Lifestyle, and Complementary Approaches
Pharmacotherapy is necessary but not sufficient for optimal outcomes in bipolar disorder. Psychosocial interventions significantly reduce relapse rates, improve medication adherence, and address the interpersonal damage that accumulates over the course of the illness.
Evidence-Based Psychotherapies
- Psychoeducation — arguably the single most important psychosocial intervention. Structured education about bipolar disorder, early warning signs, triggers, and treatment rationale dramatically improves long-term outcomes. The Barcelona Psychoeducation Program (Colom et al.) demonstrated that 21 sessions of group psychoeducation reduced both manic and depressive recurrences over 5-year follow-up.
- Cognitive-Behavioral Therapy (CBT) — targets dysfunctional thoughts and beliefs that maintain depression (cognitive distortions, helplessness) and that facilitate manic decisions (grandiosity as valid self-assessment). Lam et al. (2003) showed CBT reduced relapses and hospitalization rates in BD-I.
- Interpersonal and Social Rhythm Therapy (IPSRT) — developed specifically for bipolar disorder by Frank et al. IPSRT combines interpersonal therapy for grief and role transitions with behavioral regulation of daily routines (sleep/wake timing, meal timing, social contacts). Circadian rhythm stabilization through social rhythm regulation reduces episode frequency.
- Family-Focused Therapy (FFT) — intensive psychoeducation for the patient and family, communication enhancement training, and problem-solving. Particularly valuable for adolescents with bipolar disorder and for reducing high-expressed-emotion family environments that predict relapse.
Sleep and Circadian Rhythm Regulation
Sleep disruption is both a prodromal symptom and a trigger of bipolar episodes — a bidirectional relationship. Maintaining a consistent sleep-wake schedule (even on weekends) is one of the most powerful nonpharmacological mood-stabilizing interventions available. Patients should be counseled about sleep debt as a manic trigger, night-shift work risks, and transmeridian travel effects. Light exposure timing (bright light in the morning, minimizing blue light at night) supports circadian entrainment.
Supplements with Emerging Evidence
- Omega-3 fatty acids (EPA/DHA) — meta-analyses suggest adjunctive omega-3s (particularly high-EPA formulations at 2-4g/day) reduce bipolar depression. The mechanism involves anti-inflammatory pathways, cell membrane fluidity effects on receptor function, and modulation of arachidonic acid cascades. Not effective as monotherapy.
- Magnesium — preliminary evidence for adjunctive benefit in mania; magnesium acts as an endogenous NMDA receptor antagonist. Deficiency is common in patients on lithium or valproate.
- N-Acetylcysteine (NAC) — Berk et al. (2008) published a double-blind RCT showing NAC 2g/day significantly reduced depression scores in bipolar disorder over 24 weeks; subsequent studies have been mixed. Mechanism likely involves glutathione repletion (reducing oxidative stress) and modulation of glutamatergic neurotransmission.
- Inositol — an intracellular second messenger depleted by lithium (via inositol monophosphatase inhibition); some evidence for adjunctive antidepressant and anxiolytic benefit in bipolar disorder at 12-18g/day.
Complications and Comorbidities
Bipolar disorder rarely exists in isolation. The comorbidity burden is substantial and significantly complicates both diagnosis and treatment.
- Suicide: The most serious complication. Lifetime risk of completed suicide is 10–15 times the general population rate. Approximately 25–50% of individuals with bipolar disorder attempt suicide at least once. Lithium's antisuicidal effect — independent of mood stabilization — is one of the strongest arguments for its continued use as first-line treatment.
- Substance use disorders: The most common comorbidity — approximately 60% of individuals with BD-I have a lifetime substance use disorder. Alcohol and cannabis are most frequent. Substance use worsens outcomes: more episodes, more hospitalizations, worse medication adherence, and higher suicide risk. Comorbid substance use must be treated concurrently, not sequentially.
- Anxiety disorders: Present in up to 75% of bipolar patients across the lifespan. Panic disorder, generalized anxiety, PTSD, and social anxiety all commonly co-occur. Anxiety complicates mania (via psychomotor agitation) and deepens depression. Benzodiazepines provide short-term anxiolysis but carry addiction risk in this population.
- ADHD: True comorbidity (not just symptomatic overlap) occurs in approximately 20–30% of bipolar patients, particularly those with childhood-onset. Disentangling ADHD from bipolar disorder requires careful longitudinal history. Stimulants can be used cautiously in ADHD+bipolar patients on adequate mood stabilization.
- Metabolic syndrome: Rates of obesity, type 2 diabetes, and cardiovascular disease are substantially elevated in bipolar disorder — partly due to medications (particularly olanzapine and quetiapine) and partly due to lifestyle factors (poor diet, sedentary behavior, smoking, disrupted sleep).
- Cognitive impairment: Bipolar disorder is not a neurodegenerative illness, but cumulative episode burden produces lasting cognitive deficits in attention, memory, and executive function. Neuropsychological impairment persists between episodes ("inter-episode cognitive deficits") and worsens with each additional severe episode — another argument for early, aggressive treatment.
- Postpartum episodes: Women with bipolar disorder face a dramatically elevated risk of postpartum episodes — particularly postpartum mania and psychosis — in the first 4–6 weeks after delivery. Discontinuing mood stabilizers during pregnancy without a replacement plan is extremely high-risk. This requires careful risk-benefit analysis involving the patient, partner, psychiatrist, and obstetrician.
Research Papers
Key Research Papers
- Vieta E, et al. Bipolar disorders. Nature Reviews Disease Primers. 2018;4:18008. — Comprehensive authoritative review covering epidemiology, neurobiology, genetics, and treatment across the full bipolar spectrum.
- Grande I, et al. Bipolar disorder. The Lancet. 2016;387(10027):1561–1572. — Accessible clinical review with practice-oriented guidance on diagnosis and pharmacotherapy.
- Post RM. Transduction of psychosocial stress into the neurobiology of recurrent affective disorder. American Journal of Psychiatry. 1992;149(8):999–1010. — The foundational paper articulating the kindling hypothesis for recurrent mood disorders.
- Baldessarini RJ, Tondo L, Hennen J. Lithium treatment and suicide risk in major affective disorders: update and new findings. Journal of Clinical Psychiatry. 2003;64(Suppl 5):44–52. — Meta-analysis establishing lithium's robust antisuicidal effect across mood disorders.
- Stahl EA, et al. Genome-wide association study identifies 30 loci associated with bipolar disorder. Nature Genetics. 2019;51(5):793–803. — Largest GWAS to date; identifies shared genetic architecture with schizophrenia and depression.
- Sachs GS, et al. Effectiveness of adjunctive antidepressant treatment for bipolar depression. New England Journal of Medicine. 2007;356(17):1711–1722. — STEP-BD primary outcome paper; showed adjunctive antidepressants no more effective than mood stabilizer alone for bipolar depression.
- Calabrese JR, et al. A randomized, double-blind, placebo-controlled trial of quetiapine in the treatment of bipolar I or II depression. American Journal of Psychiatry. 2005;162(7):1351–1360. — BOLDER II trial establishing quetiapine efficacy for bipolar depression.
- Durgam S, et al. Cariprazine in acute exacerbation of schizophrenia and bipolar I disorder. Journal of Clinical Psychiatry. 2016;77(3):e305–e312. — Pivotal trial supporting FDA approval of cariprazine for acute mania and bipolar depression.
- Yatham LN, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder. Bipolar Disorders. 2018;20(2):97–170. — The most comprehensive current clinical guidelines covering all phases of bipolar disorder.
- Cipriani A, et al. Lithium in the prevention of suicide in mood disorders: updated systematic review and meta-analysis. BMJ. 2013;346:f3646. — Definitive meta-analysis confirming lithium's unique antisuicidal properties.
- Tomson T, et al. Valproate in the treatment of epilepsy in girls and women of childbearing potential. Epilepsia. 2015;56(7):1006–1019. — Comprehensive review of valproate teratogenicity informing the FDA REMS program guidance.
- Berk M, et al. N-acetyl cysteine as a glutathione precursor for schizophrenia — a double-blind, randomized, placebo-controlled trial. Biological Psychiatry. 2008;64(5):361–368. — Pivotal RCT showing NAC's benefit in bipolar depression through oxidative stress and glutamatergic pathways.
PubMed Topic Searches
- PubMed: bipolar disorder DSM-5 diagnosis
- PubMed: bipolar disorder lithium maintenance
- PubMed: bipolar disorder valproate mania
- PubMed: lamotrigine bipolar depression maintenance
- PubMed: quetiapine bipolar depression BOLDER trials
- PubMed: bipolar disorder mixed features
- PubMed: bipolar disorder kindling sensitization Post
- PubMed: cariprazine bipolar disorder
- PubMed: bipolar disorder suicide prevention
- PubMed: bipolar antidepressant manic switch STEP-BD
- PubMed: bipolar disorder omega-3 fatty acids
- PubMed: bipolar disorder GWAS genetics
Connections
- Depression
- Anxiety
- Schizophrenia
- Insomnia
- ADHD
- Postpartum Depression
- Addiction
- Magnesium
- Vitamin D3
- Omega-3 Fatty Acids
- Choline
- Inositol
- Sleep Hygiene
- Stress Management
- NAC and Mental Health
- Dementia
- Vitamin B12
- Natural Anxiety Relief
- Fatigue
- Breathwork