Chronic Cough
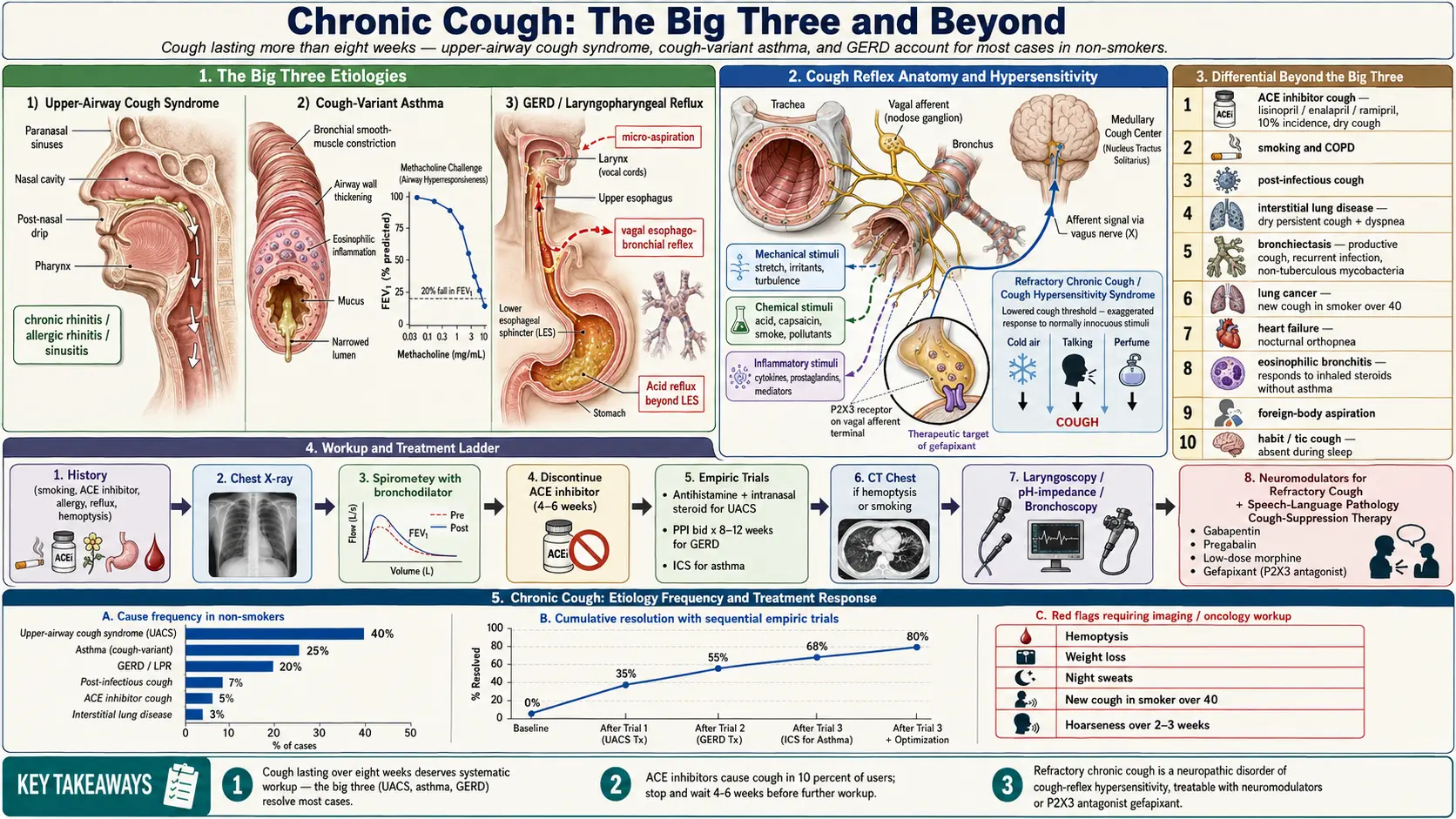

Table of Contents
- Overview
- Types of Cough
- Common Causes
- Mechanisms
- Evaluation
- Management
- When to Seek Medical Care
- Connections
- References & Research
- Featured Videos
Overview
Chronic cough is defined as cough lasting more than eight weeks in adults (four weeks in children). It is one of the most common reasons for outpatient visits and one of the most under-evaluated. In a non-smoker not on an ACE inhibitor, the "big three" account for the great majority of cases: upper-airway cough syndrome (formerly post-nasal drip), cough-variant asthma, and gastroesophageal reflux. A systematic, sequential approach can resolve symptoms in most patients, while a smaller group with cough that resists this approach has "refractory chronic cough" driven by cough-reflex hypersensitivity, and benefits from neuromodulator therapy.
Types of Cough
- Acute cough — less than three weeks; usually viral upper respiratory infection.
- Subacute cough — three to eight weeks; commonly post-infectious cough after a viral illness, sometimes pertussis.
- Chronic cough — more than eight weeks; what this page addresses.
- Dry vs productive — productive (mucus) suggests bronchitis, COPD, bronchiectasis, infection; dry suggests asthma, reflux, post-nasal drip, ILD, ACE-inhibitor cough.
- Daytime vs nocturnal — nocturnal cough that wakes the patient suggests asthma, GERD, or heart failure.
- Refractory chronic cough — persistent despite treatment of identifiable causes; cough-reflex hypersensitivity is the unifying concept.
- Hemoptysis — coughing blood; always warrants evaluation.
Common Causes
- Upper-airway cough syndrome — chronic rhinitis, post-nasal drip, allergic rhinitis, sinusitis. The most common cause in non-smokers.
- Asthma and cough-variant asthma — cough is the dominant or only symptom in cough-variant asthma; spirometry may be normal between flares.
- GERD and laryngopharyngeal reflux (LPR) — reflux of acid or non-acid contents triggers cough through vagal reflex and direct laryngeal irritation.
- ACE inhibitor cough — lisinopril, enalapril, ramipril, etc. produce a dry cough in about 10 percent of users; resolves within weeks of discontinuation.
- Smoking and COPD — current smokers and patients with chronic bronchitis or emphysema.
- Post-infectious cough — persistent airway hyperreactivity for weeks to months after a viral or bacterial respiratory infection.
- Interstitial lung disease and pulmonary fibrosis — dry, persistent cough with progressive shortness of breath.
- Bronchiectasis and chronic infection — productive cough, often with recurrent infections; consider non-tuberculous mycobacteria and atypical pathogens.
- Lung cancer — particularly in smokers and former smokers; new persistent cough or change in chronic cough warrants imaging.
- Heart failure — nocturnal cough, orthopnea, dyspnea on exertion, leg swelling.
- Eosinophilic bronchitis — airway eosinophilia without asthma; responds to inhaled corticosteroids.
- Foreign-body aspiration — consider in any sudden-onset persistent cough, particularly children and the cognitively impaired.
- Habit cough and tic cough — often in children and adolescents; absent during sleep.
Mechanisms
- Cough reflex — mechanical, chemical, and inflammatory stimuli activate vagal afferent nerves in the airway; signals travel to the medulla and trigger the cough motor program.
- Cough-reflex hypersensitivity — in chronic cough, the threshold for triggering cough is lowered; ordinary stimuli (cold air, talking, perfume) provoke cough.
- Inflammation — eosinophilic, neutrophilic, or mixed airway inflammation produces ongoing afferent stimulation.
- Mucus and ciliary dysfunction — excess mucus or impaired clearance triggers cough; central in COPD, bronchiectasis, and cystic fibrosis.
- Reflux pathways — both micro-aspiration of refluxate and vagally mediated reflexes (esophago-bronchial) drive reflux-related cough.
Evaluation
- History — smoking, occupational exposures, ACE inhibitor use, allergies, reflux symptoms, weight loss, fever, hemoptysis, travel, TB exposure.
- Chest X-ray — first-line imaging in any chronic cough.
- Spirometry — with bronchodilator response; methacholine challenge if normal but asthma still suspected.
- Discontinue ACE inhibitor — if applicable; allow up to 4–6 weeks for resolution.
- Empiric trial for upper-airway cough syndrome — first-generation antihistamine plus decongestant or intranasal corticosteroid for 2–3 weeks.
- Empiric trial for GERD — PPI twice daily for 8–12 weeks plus lifestyle modifications.
- CT chest — if abnormal X-ray, hemoptysis, smoking history, or no response to empiric therapy.
- ENT evaluation — laryngoscopy for refractory or LPR-suggestive cough.
- Esophageal pH-impedance testing — for non-acid reflux when PPI fails.
- Bronchoscopy — for hemoptysis, suspected foreign body, or persistent unexplained findings.
Management
- Stop smoking — the single most effective intervention in smokers.
- Discontinue ACE inhibitors — switch to ARB if needed.
- Treat upper-airway cough syndrome — intranasal corticosteroid, second-generation antihistamine for allergic rhinitis; first-generation antihistamine + decongestant for non-allergic rhinitis.
- Treat asthma and cough-variant asthma — inhaled corticosteroid with or without long-acting beta-agonist; leukotriene antagonist as adjunct.
- Treat GERD — PPI, weight loss, bed-head elevation, avoidance of late meals and trigger foods; consider surgical fundoplication for refractory cases.
- Treat eosinophilic bronchitis — inhaled corticosteroids.
- Pulmonary rehabilitation and airway clearance — in COPD, bronchiectasis, ILD.
- Cough-suppressant neuromodulators — gabapentin, pregabalin, low-dose morphine, and the P2X3 antagonist gefapixant for refractory chronic cough.
- Speech-language pathology cough-suppression therapy — behavioral retraining of cough reflex, particularly for refractory chronic cough and habit cough.
- Vaccinations — influenza, pneumococcal, pertussis to reduce post-infectious cough.
When to Seek Medical Care
- Coughing up blood (any amount).
- Unintentional weight loss, drenching night sweats, or persistent fever.
- Progressive shortness of breath or chest pain with cough.
- New cough in a current or former smoker over 40.
- Cough lasting more than eight weeks not responding to standard therapy.
- Hoarseness or voice change persisting more than 2–3 weeks.
- Cough with leg swelling, orthopnea (consider heart failure).
- Known TB exposure or recent travel to endemic areas.
Connections
- Asthma
- COPD
- Interstitial Lung Disease
- GERD
- Heart Failure
- Influenza
- Allergies
- Pneumonia
- Pulmonary Embolism
- Reflux
- Shortness of Breath
- Chest Pain
- Sinusitis
- Cystic Fibrosis
- Mold Mycotoxins
References & Research
Historical Background
The systematic study of chronic cough began with Irwin's 1981 anatomic-diagnostic protocol, which established the "big three" etiologies and a sequential approach. The European Respiratory Society and American College of Chest Physicians have since published a series of guidelines, and the conceptual framework has shifted from "identify the cause" to "identify the cough hypersensitivity phenotype." The 2022 approval of gefapixant in several jurisdictions made refractory chronic cough a treatable condition for the first time.
Key Research Papers
- Irwin RS, Corrao WM, Pratter MR. Chronic persistent cough in the adult: the spectrum and frequency of causes and successful outcome of specific therapy. American Review of Respiratory Disease. 1981;123(4):413-417.
- Morice AH, Millqvist E, Bieksiene K, et al. ERS guidelines on the diagnosis and treatment of chronic cough in adults and children. European Respiratory Journal. 2020;55(1):1901136.
- Irwin RS, Baumann MH, Bolser DC, et al. Diagnosis and management of cough: ACCP evidence-based clinical practice guidelines. Chest. 2006;129(1 Suppl):1S-23S.
- McGarvey LP, Birring SS, Morice AH, et al. Efficacy and safety of gefapixant, a P2X3 receptor antagonist, in refractory chronic cough and unexplained chronic cough (COUGH-1 and COUGH-2). The Lancet. 2022;399(10328):909-923.
- Chung KF, McGarvey L, Mazzone SB. Chronic cough as a neuropathic disorder. Lancet Respiratory Medicine. 2013;1(5):414-422.
- Pratter MR. Chronic upper airway cough syndrome secondary to rhinosinus diseases (previously referred to as postnasal drip syndrome). Chest. 2006;129(1 Suppl):63S-71S.
- Dicpinigaitis PV. Chronic cough due to asthma. Chest. 2006;129(1 Suppl):75S-79S.
- Irwin RS. Chronic cough due to gastroesophageal reflux disease. Chest. 2006;129(1 Suppl):80S-94S.
- Vertigan AE, Theodoros DG, Gibson PG, Winkworth AL. Efficacy of speech pathology management for chronic cough: a randomised placebo-controlled trial. Thorax. 2006;61(12):1065-1069.
- Ryan NM, Birring SS, Gibson PG. Gabapentin for refractory chronic cough: a randomised, double-blind, placebo-controlled trial. The Lancet. 2012;380(9853):1583-1589.
PubMed Topic Searches
- Chronic cough evaluation
- Cough-variant asthma
- GERD and chronic cough
- Cough hypersensitivity syndrome
- Gefapixant and P2X3 antagonists for cough
- ACE inhibitor cough