Reflux and Heartburn
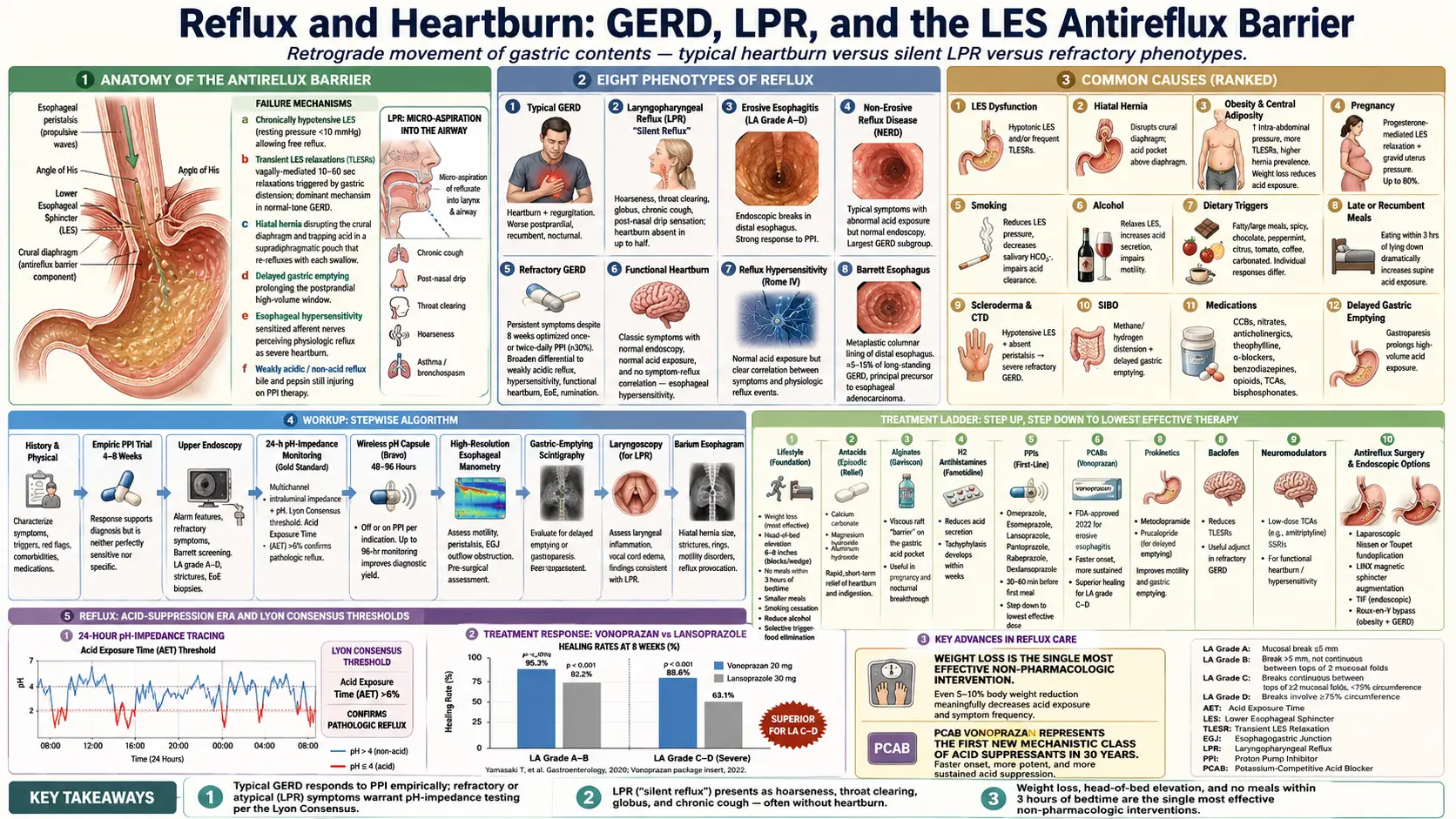

Table of Contents
- Overview
- Types of Reflux
- Common Causes
- Mechanisms
- Evaluation
- Management
- When to Seek Medical Care
- Connections
- References & Research
- Featured Videos
Overview
Reflux is the retrograde movement of gastric contents up into the esophagus, and sometimes beyond into the throat, larynx, or airways. Heartburn is the burning retrosternal sensation that often, but not always, accompanies reflux. Regurgitation is the effortless return of acidic or bitter material into the mouth. Gastroesophageal reflux disease (GERD) is diagnosed when reflux produces troublesome symptoms or measurable mucosal injury, occurring in roughly 20 percent of adults in Western populations. Laryngopharyngeal reflux (LPR), also called "silent reflux," is a related condition in which refluxate reaches the larynx and pharynx and produces hoarseness, chronic throat clearing, post-nasal drip sensation, globus, and chronic cough — often without classic heartburn. Not all reflux is symptomatic, not all heartburn is GERD, and the relationship between perceived symptoms and objective acid exposure is loose enough that diagnosis often requires more than a history alone.
Types of Reflux
- Typical GERD — classic heartburn and regurgitation, worse after meals, when bending or lying flat, and at night. Symptoms respond reasonably well to acid-suppressive therapy.
- Laryngopharyngeal reflux (LPR / silent reflux) — refluxate reaches the upper aerodigestive tract. Predominant symptoms are hoarseness, chronic throat clearing, globus (lump-in-throat sensation), chronic cough, and post-nasal-drip sensation. Heartburn is absent in up to half of cases.
- Erosive esophagitis — endoscopically visible breaks in the distal esophageal mucosa from acid injury. Graded by the Los Angeles classification A through D. Strongly responsive to PPIs.
- Non-erosive reflux disease (NERD) — typical GERD symptoms with abnormal acid exposure on pH testing but a normal-appearing endoscopy. The largest GERD subgroup; response to PPIs is more variable.
- Refractory GERD — persistent symptoms despite at least eight weeks of optimized once- or twice-daily PPI therapy. Roughly 30 percent of GERD patients fall here, and the differential broadens to include weakly acidic reflux, esophageal hypersensitivity, functional heartburn, eosinophilic esophagitis, and rumination.
- Functional heartburn — classic heartburn symptoms, normal endoscopy, normal acid exposure, and no symptom-reflux correlation. A disorder of esophageal hypersensitivity rather than acid burden.
- Reflux hypersensitivity — normal acid exposure but a clear correlation between symptoms and physiologic reflux events. A Rome IV diagnosis distinct from both NERD and functional heartburn.
- Barrett esophagus — metaplastic columnar lining of the distal esophagus, the principal precursor to esophageal adenocarcinoma. Develops in 5–15 percent of long-standing GERD.
Common Causes
- Lower esophageal sphincter (LES) dysfunction — baseline hypotension or frequent transient relaxations of the LES allow gastric contents to move retrograde.
- Hiatal hernia — the proximal stomach herniates above the diaphragm, disrupting the antireflux barrier and creating a reservoir of acid that refluxes easily.
- Obesity and central adiposity — increased intra-abdominal pressure, increased TLESR frequency, and higher prevalence of hiatal hernia. Weight loss is one of the few interventions shown to reduce acid exposure.
- Pregnancy — progesterone-mediated LES relaxation plus mechanical pressure from the gravid uterus. Reflux affects up to 80 percent of pregnancies, peaking in the third trimester.
- Smoking — reduces LES pressure, decreases salivary bicarbonate (which neutralizes refluxate), and impairs esophageal acid clearance.
- Alcohol — relaxes the LES, increases gastric acid secretion, and impairs esophageal motility.
- Dietary triggers — fatty meals, large meals, spicy food, chocolate, peppermint, citrus, tomato-based foods, coffee, and carbonated beverages variably provoke symptoms; individual responses differ.
- Late or recumbent meals — eating within three hours of lying down dramatically increases supine acid exposure.
- Scleroderma and other connective-tissue diseases — produce a hypotensive LES with absent esophageal peristalsis, leading to severe and often refractory GERD.
- Small intestinal bacterial overgrowth (SIBO) — methane- and hydrogen-driven distension and delayed gastric emptying can worsen reflux; many patients describe overlapping bloating and heartburn.
- Medications — calcium-channel blockers, nitrates, anticholinergics, theophylline, alpha-blockers, benzodiazepines, opioids, tricyclic antidepressants, and bisphosphonates lower LES pressure or directly irritate the esophagus.
- Delayed gastric emptying — gastroparesis from diabetes or post-viral injury increases gastric volume and TLESR frequency.
Mechanisms
Reflux occurs when the antireflux barrier at the gastroesophageal junction fails. Several overlapping mechanisms are usually involved:
- LES barrier failure — chronically hypotensive LES (resting pressure below 10 mmHg) allows free reflux, particularly with increased intra-abdominal pressure. Common in scleroderma, severe obesity, and large hiatal hernia.
- Transient LES relaxations (TLESRs) — vagally mediated, swallow-independent relaxations of the LES lasting 10–60 seconds. The dominant mechanism of reflux in patients with otherwise normal LES tone, triggered by gastric distension after meals.
- Hiatal hernia — disrupts the crural diaphragm component of the antireflux barrier and traps acid in a supradiaphragmatic pouch that re-refluxes with each swallow.
- Delayed gastric emptying — prolongs the postprandial window of high gastric volume and increases TLESR frequency.
- Esophageal hypersensitivity — even physiologic reflux is perceived as severe heartburn. Central and peripheral sensitization of esophageal afferent nerves drives symptoms in NERD, reflux hypersensitivity, and functional heartburn.
- Weakly acidic and non-acid reflux — on PPI therapy, gastric pH rises but reflux events continue; bile, pepsin, and weakly acidic refluxate can still produce symptoms and tissue injury, particularly in the larynx.
- Pepsin and bile in LPR — pepsin is taken up by laryngeal cells and reactivated when the local pH drops, perpetuating mucosal injury even between reflux events. Bile acids contribute to non-acid LPR symptoms.
- Micro-aspiration — small-volume aspiration of refluxate into the airway in LPR drives chronic cough, post-nasal-drip sensation, and asthma exacerbations.
- Impaired esophageal clearance — weak peristalsis and reduced salivary bicarbonate prolong contact time between refluxate and mucosa.
Evaluation
Most uncomplicated reflux is diagnosed and treated empirically. Objective testing is reserved for alarm features, refractory symptoms, atypical presentations, or pre-surgical workup.
- Symptom-based diagnosis — classic heartburn and regurgitation in the absence of alarm features have a high enough specificity that empiric therapy is reasonable first-line.
- Empiric PPI trial — once-daily PPI for four to eight weeks. Symptom response supports the diagnosis but is neither perfectly sensitive nor specific.
- Upper endoscopy — indicated for alarm features, symptoms refractory to PPIs, or screening for Barrett esophagus in long-standing GERD with risk factors. Identifies erosive esophagitis (LA grade A–D), strictures, Barrett, eosinophilic esophagitis, and malignancy.
- 24-hour pH-impedance monitoring — the gold standard for quantifying acid and non-acid reflux. Performed off PPI to confirm GERD or on PPI to evaluate refractory symptoms. The Lyon Consensus thresholds (acid exposure time greater than 6 percent on pH studies) define conclusive evidence of pathologic reflux.
- Wireless pH capsule (Bravo) — 48- to 96-hour ambulatory recording without a transnasal catheter; better tolerated than catheter-based studies.
- High-resolution esophageal manometry — required before antireflux surgery to rule out achalasia and severe motility disorders, and useful in evaluating refractory symptoms and dysphagia.
- Gastric-emptying scintigraphy — if delayed emptying is suspected (early satiety, postprandial fullness, vomiting of undigested food).
- Laryngoscopy — in suspected LPR, to identify posterior laryngeal edema, erythema, and pseudosulcus. Findings are nonspecific and do not by themselves confirm reflux.
- Barium esophagram — useful to demonstrate hiatal hernia, strictures, and motility abnormalities; less sensitive than endoscopy for mucosal disease.
- Eosinophilic esophagitis biopsies — even in patients without dysphagia, esophageal biopsies during endoscopy are often warranted in PPI-refractory symptoms to rule out EoE.
Management
- Lifestyle modification — weight loss in overweight or obese patients (the single most effective non-pharmacologic intervention), elevation of the head of the bed by 6–8 inches (use blocks or a wedge, not extra pillows), avoiding meals within 3 hours of bedtime, smaller meals, smoking cessation, and reducing alcohol. Selective trigger-food elimination is reasonable when individual triggers are clear.
- Antacids — calcium carbonate, magnesium hydroxide, aluminum hydroxide. Fast-acting symptomatic relief; appropriate for episodic symptoms but not for daily use.
- Alginates — Gaviscon and similar agents form a viscous raft on top of gastric contents that suppresses the postprandial acid pocket. Useful adjunct, particularly in pregnancy and for breakthrough nocturnal symptoms.
- H2-receptor antagonists — famotidine, nizatidine, cimetidine. Useful for mild or intermittent symptoms and as nighttime add-on therapy. Tachyphylaxis develops within weeks of regular use. Ranitidine was withdrawn worldwide in 2020 due to NDMA contamination.
- Proton pump inhibitors (PPIs) — omeprazole, esomeprazole, lansoprazole, pantoprazole, rabeprazole, dexlansoprazole. The mainstay for erosive esophagitis, NERD, and many cases of LPR. Take 30–60 minutes before the first meal of the day. Step-down to the lowest effective dose after symptom control. Long-term safety concerns (kidney disease, fracture, dementia, pneumonia, C. difficile, magnesium and B12 deficiency) are mostly observational and modest in absolute risk, but warrant the lowest dose for the shortest duration that controls disease.
- Potassium-competitive acid blockers (PCABs) — vonoprazan was approved by the FDA in 2022 for erosive esophagitis. Faster onset and more sustained acid suppression than PPIs, with non-inferiority for healing erosive disease and superiority for severe LA grade C–D esophagitis.
- Prokinetics — metoclopramide, domperidone (where available), and prucalopride may help when delayed gastric emptying contributes. Long-term metoclopramide carries tardive dyskinesia risk; reserve for specific indications.
- Baclofen — reduces TLESR frequency; an option in refractory GERD with documented non-acid reflux, though sedation limits use.
- Neuromodulators — low-dose tricyclics (amitriptyline) or SSRIs help functional heartburn and reflux hypersensitivity by reducing visceral pain perception.
- Antireflux surgery — laparoscopic Nissen or Toupet (partial) fundoplication, indicated for PPI-refractory disease with documented reflux, large hiatal hernia, or PPI intolerance. Long-term, roughly 60–70 percent of patients remain off acid-suppressive medication at 10 years.
- Magnetic sphincter augmentation (LINX device) — a ring of magnetic beads laparoscopically placed at the GE junction; comparable efficacy to fundoplication with less postoperative bloating and gas-bloat syndrome.
- Transoral incisionless fundoplication (TIF) — endoscopic creation of a partial fundoplication using the EsophyX device. An option for selected patients who want a less invasive procedure than laparoscopic surgery.
- Bariatric surgery — Roux-en-Y gastric bypass is the antireflux procedure of choice for patients with both morbid obesity and GERD; sleeve gastrectomy can worsen reflux.
- LPR-specific measures — aggressive lifestyle change (especially weight loss, late-meal avoidance, head-of-bed elevation), often twice-daily PPI for 12–16 weeks, alginates after meals and at bedtime, and treatment of any concurrent rhinosinusitis. Symptom response is slower than in classic GERD.
When to Seek Medical Care
- Dysphagia — difficulty swallowing or food sticking, raises concern for stricture, eosinophilic esophagitis, or malignancy.
- Odynophagia — painful swallowing, suggests severe esophagitis, infection, or pill esophagitis.
- Unintentional weight loss — especially with new or worsening reflux symptoms.
- Iron-deficiency anemia or evidence of chronic blood loss.
- Hematemesis, melena, or hematochezia — vomiting blood, black tarry stool, or bloody stool.
- Persistent vomiting — particularly of undigested food (suggests gastroparesis or obstruction).
- New-onset symptoms in adults over 50, or a long GERD history with new alarm features, where Barrett esophagus and adenocarcinoma must be considered.
- Chest pain — cardiac causes must be excluded before attributing chest pain to reflux, particularly in patients with cardiovascular risk factors.
- Refractory symptoms on twice-daily PPI for 8–12 weeks — warrant referral for endoscopy and pH-impedance testing.
- Choking or aspiration episodes, recurrent pneumonia, or worsening asthma.
Connections
- SIBO
- GERD
- Bloating
- Peptic Ulcer Disease
- Asthma
- Gallbladder Disease
- Gut Healing
- Prokinetics & Relapse Prevention
- Nausea and Vomiting
- SIBO Root Causes
- Abdominal Pain
- Chronic Cough
- Chest Pain
- Obesity
- Magnesium
- Peppermint
- Fennel
- Licorice
- Esophageal Cancer
References & Research
Historical Background
Reflux was recognized clinically for centuries but understood mechanistically only in the late twentieth century. The histamine H2-receptor antagonists ushered in the modern era of acid suppression: cimetidine reached US markets in 1977 and became the first billion-dollar drug, with ranitidine and famotidine following through the 1980s. Omeprazole, the first proton pump inhibitor, was approved in Europe in 1988 and in the US in 1989, transforming the treatment of erosive esophagitis and peptic ulcer disease. The Montreal Definition (Vakil 2006) standardized terminology and diagnostic criteria, distinguishing esophageal from extraesophageal manifestations of GERD. Through the 2000s and 2010s, laryngopharyngeal reflux gained increasing recognition through the work of Koufman and others, although consensus on diagnosis and treatment remained uneven. The Lyon Consensus (2018, updated 2024) consolidated the use of pH-impedance metrics to define conclusive evidence of pathologic reflux. The potassium-competitive acid blocker vonoprazan, available in Japan since 2015, received FDA approval for erosive esophagitis in 2022 and represents the first new mechanistic class of acid suppressants in three decades.
Key Research Papers
- Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R; Global Consensus Group. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. American Journal of Gastroenterology. 2006;101(8):1900-1920.
- Katz PO, Dunbar KB, Schnoll-Sussman FH, Greer KB, Yadlapati R, Spechler SJ. ACG clinical guideline for the diagnosis and management of gastroesophageal reflux disease. American Journal of Gastroenterology. 2022;117(1):27-56.
- Gyawali CP, Kahrilas PJ, Savarino E, et al. Modern diagnosis of GERD: the Lyon Consensus. Gut. 2018;67(7):1351-1362.
- Gyawali CP, Yadlapati R, Fass R, et al. Updates to the modern diagnosis of GERD: Lyon Consensus 2.0. Gut. 2024;73(2):361-371.
- Kahrilas PJ. Gastroesophageal reflux disease. New England Journal of Medicine. 1995;333(15):1014-1020. (Foundational PPI-era review)
- Galmiche JP, Hatlebakk J, Attwood S, et al. Laparoscopic antireflux surgery vs esomeprazole treatment for chronic GERD: the LOTUS randomized clinical trial. JAMA. 2011;305(19):1969-1977.
- Spechler SJ, Hunter JG, Jones KM, et al. Randomized trial of medical versus surgical treatment for refractory heartburn. New England Journal of Medicine. 2019;381(16):1513-1523.
- Laine L, DeVault K, Katz P, et al. Vonoprazan versus lansoprazole for healing and maintenance of healing of erosive esophagitis: a randomized trial. Gastroenterology. 2023;164(1):61-71.
- Koufman JA, Aviv JE, Casiano RR, Shaw GY. Laryngopharyngeal reflux: position statement of the committee on speech, voice, and swallowing disorders of the American Academy of Otolaryngology–Head and Neck Surgery. Otolaryngology–Head and Neck Surgery. 2002;127(1):32-35.
- Yadlapati R, Gyawali CP, Pandolfino JE; CGIT GERD Consensus Conference Participants. AGA clinical practice update on the personalized approach to the evaluation and management of GERD. Clinical Gastroenterology and Hepatology. 2022;20(5):984-994.
PubMed Topic Searches
- Gastroesophageal reflux disease pathophysiology
- Laryngopharyngeal reflux (LPR / silent reflux)
- Lyon Consensus — pH-impedance and GERD
- Vonoprazan and erosive esophagitis
- Transient LES relaxations (TLESRs)
- Fundoplication and LINX antireflux surgery