CAC vs CT Angiography vs Stress Test vs ApoB: When Each Test Is Right
Cardiovascular testing is a layered system, not a single test. The coronary calcium score occupies a specific niche — quantifying calcified plaque burden in asymptomatic adults — but is not the right answer for symptomatic chest pain, suspected acute coronary syndrome, evaluation of ischemia, or initial lipid screening. This page maps the major cardiac tests to the questions they actually answer, when CAC is the right tool, and when something else (CCTA, stress testing, ApoB/Lp(a), cardiac MRI) is the better fit.
Table of Contents
- What Each Test Actually Answers
- Coronary Artery Calcium (CAC)
- CT Coronary Angiography (CCTA)
- Exercise & Pharmacologic Stress Tests
- Cardiac MRI
- Invasive Cardiac Catheterization
- Lipid Markers (ApoB, Lp(a), LDL-C)
- Practical Decision Tree
- When CAC Isn't the Right Test
- Research Papers and References
- Connections
- Featured Videos
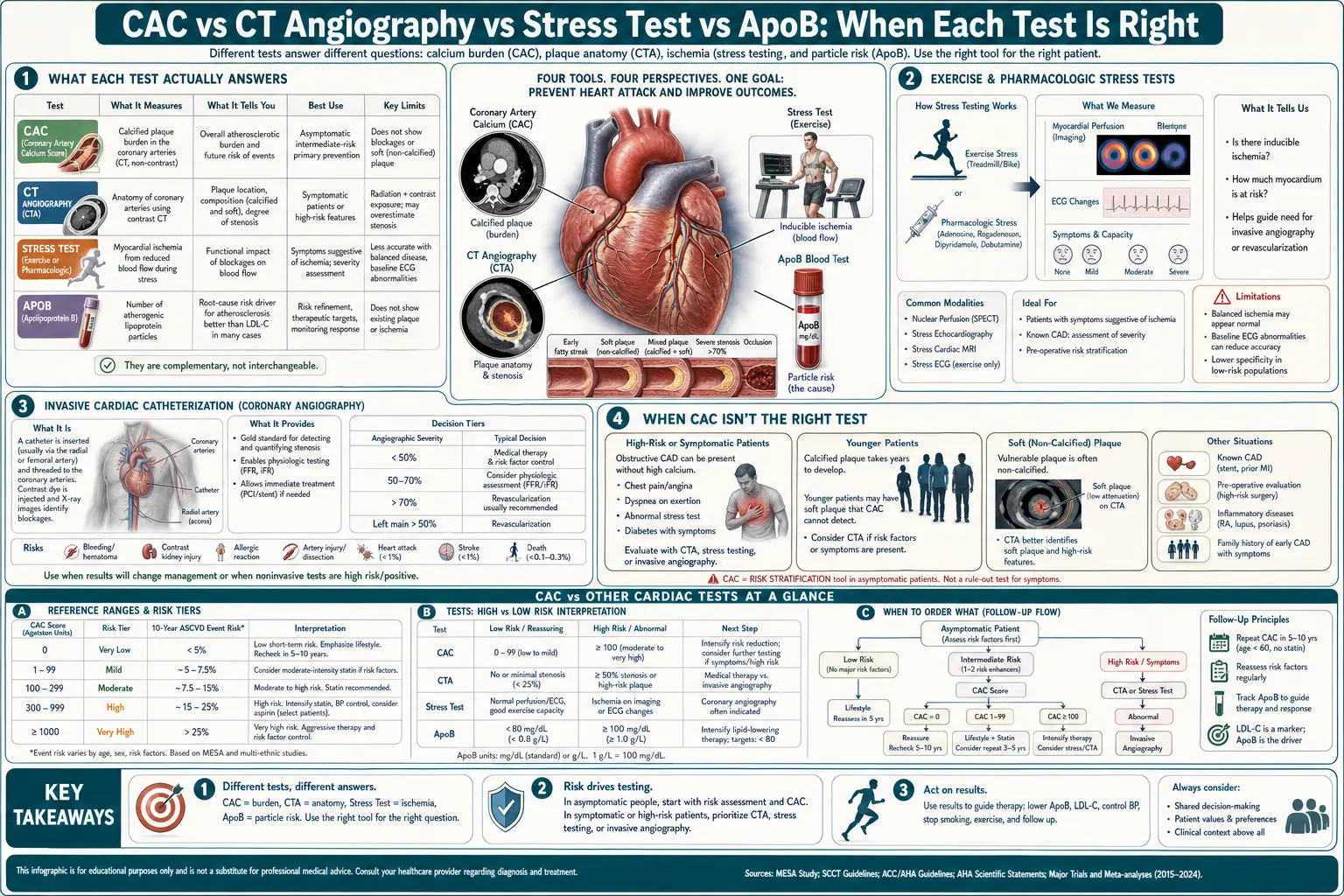
What Each Test Actually Answers
- CAC — "How much mature, calcified plaque burden have I accumulated?"
- CCTA — "What is the geometry and severity of plaque (calcified and non-calcified) in my coronaries?"
- Stress test — "Is plaque obstructing flow enough to cause ischemia under exertion?"
- Cardiac MRI — "What is the structure, function, and tissue character of my heart muscle?"
- Cardiac catheterization — "What is the gold-standard view of my coronaries, and can I be treated in the same procedure?"
- ApoB / Lp(a) / LDL-C — "What is the lipoprotein burden driving plaque formation?"
These are different questions. The right test depends on which question is being asked.
Coronary Artery Calcium (CAC)
- Best for: Asymptomatic adults aged 40–75 at intermediate ASCVD risk where the statin decision is uncertain
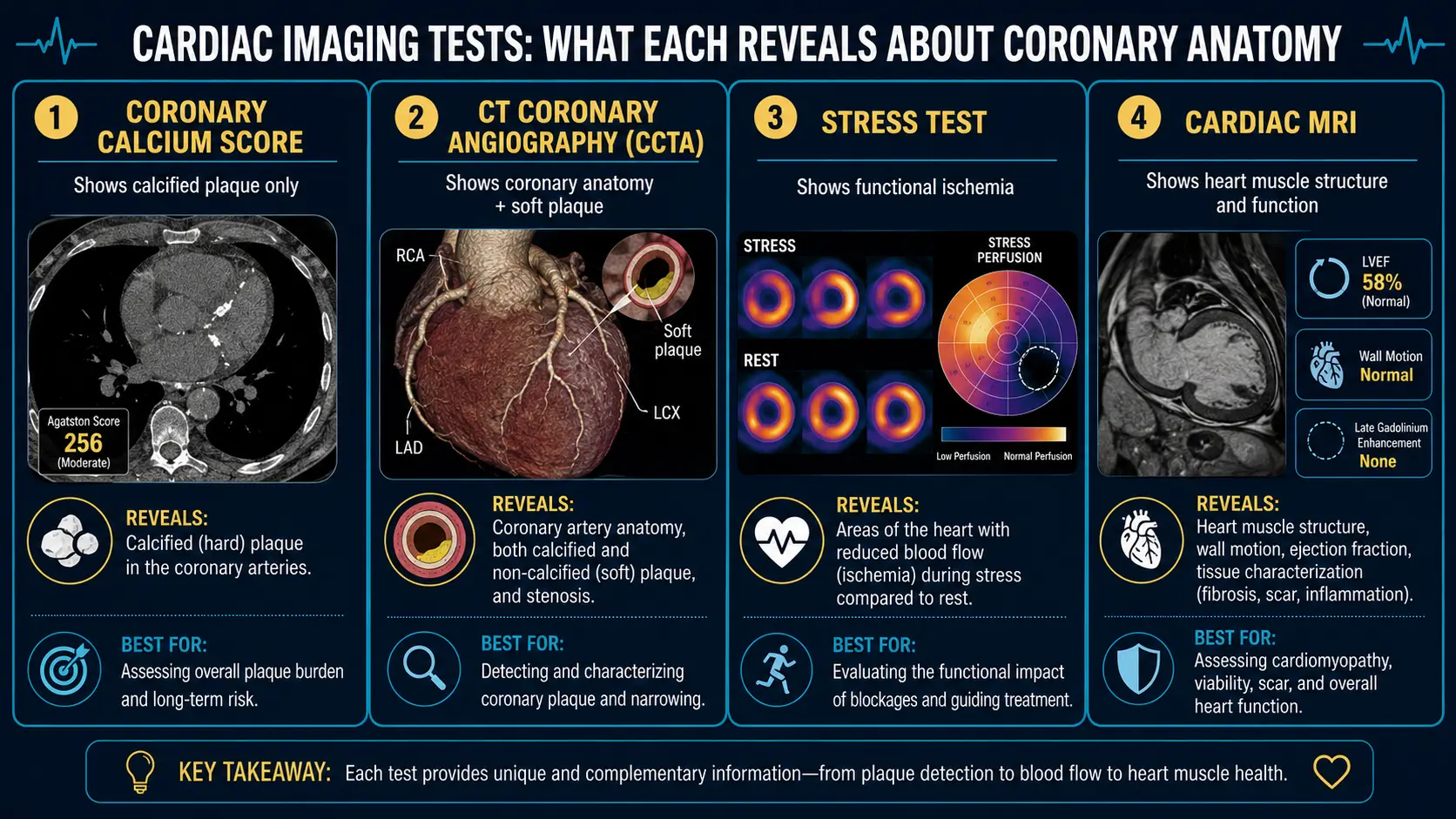
- What it shows: Calcified plaque burden, total Agatston score, vessel distribution, age/sex percentile
- What it misses: Soft (non-calcified) plaque, vulnerable plaque, microvascular disease, electrical conduction issues
- Cost: $99–$200 cash; rarely covered by insurance
- Radiation: ~1 mSv (similar to a mammogram)
- Time: 10 minutes
- No prep, no contrast, no IV
CT Coronary Angiography (CCTA)
- Best for: Symptomatic patients with low-to-intermediate pretest probability of CAD; younger patients with strong family history; patients with elevated Lp(a) where soft-plaque burden matters
- What it shows: Detailed coronary anatomy, plaque composition (soft vs calcified), stenosis severity, plaque vulnerability features, fractional flow reserve (FFR-CT) in some centers
- What it misses: Microvascular dysfunction; functional significance of intermediate stenosis (though FFR-CT addresses this)
- Cost: $500–$2,000; often partially covered with appropriate indication
- Radiation: 3–10 mSv (improving with newer scanners)
- Time: 30–60 minutes including prep
- Requires: IV contrast, beta-blocker for heart rate <65, sometimes nitroglycerin
- Contrast contraindications: severe renal impairment, prior contrast reaction
CCTA has surged in clinical use over the past decade, particularly after the SCOT-HEART trial showed that CCTA-guided care reduced 5-year MI rates compared to standard care. It is now first-line in many centers for stable chest pain evaluation.
Exercise & Pharmacologic Stress Tests
- Treadmill EKG stress test — cheapest stress test; sensitivity ~50–70% for obstructive CAD; useful for functional capacity assessment but limited diagnostic accuracy
- Stress echo — adds wall-motion analysis; sensitivity ~80–85%; no radiation
- Nuclear stress (SPECT, PET) — perfusion imaging; sensitivity ~85–90%; some radiation; PET higher resolution and lower radiation than SPECT
- Stress cardiac MRI — perfusion + function; high sensitivity; no radiation; longer test, higher cost
- Pharmacologic stress (dobutamine, regadenoson) — for patients who cannot exercise
Stress tests answer a functional question: is there flow-limiting ischemia? They are appropriate when symptoms suggest ischemia or when you need to confirm functional consequences of anatomic disease seen on CCTA. They are not the right primary test for asymptomatic risk stratification, where CAC outperforms.
Cardiac MRI
- Best for: Cardiomyopathy evaluation, pericardial disease, cardiac mass, congenital heart disease, late gadolinium enhancement to characterize scarring
- What it shows: Heart structure and function in exquisite detail; myocardial tissue characterization; viability assessment
- What it misses: Direct coronary visualization (poor for stenosis evaluation)
- Cost: $1,500–$3,500
- Radiation: none
- Time: 45–90 minutes
- Requires: stillness, breath-holds, often gadolinium contrast
Cardiac MRI is not a coronary plaque test. It is a heart-muscle test. Different question, different tool.
Invasive Cardiac Catheterization
- Best for: Acute coronary syndrome, high-likelihood obstructive disease where intervention may be needed in the same session, surgical planning
- What it shows: Real-time coronary anatomy with the option to measure pressure gradient (FFR), perform IVUS/OCT for plaque characterization, and intervene with stenting or rotational atherectomy
- Cost: $20,000+ (covered by insurance for appropriate indications)
- Radiation: ~5–15 mSv
- Risks: bleeding, vascular injury, contrast nephropathy, stroke (rare)
- Time: 60–120 minutes; longer if intervention performed
The most invasive test; appropriate when non-invasive testing has localized significant disease and intervention is anticipated. Not a screening tool.
Lipid Markers (ApoB, Lp(a), LDL-C)
- LDL-C — the conventional lipid marker; calculated or directly measured; useful for screening and treatment monitoring
- ApoB — measures the number of atherogenic particles directly; outperforms LDL-C in particle-discordant patients (metabolic syndrome, T2DM, hypertriglyceridemia)
- Lp(a) — genetically determined, mostly fixed across life; an independent risk factor with no proven pharmacologic treatment yet (RNA-targeted therapies in trials); crucial in family-history-of-premature-CAD patients
The lipid markers and CAC answer different questions: lipid markers describe the driving forces of atherosclerosis, CAC describes the current state of accumulated plaque. They are complementary.
Practical Decision Tree
Asymptomatic adult, primary prevention:
- Annual lipid panel including ApoB if not previously done
- Lp(a) once in lifetime (genetically fixed)
- ASCVD risk calculator
- If intermediate risk (5–19.9%) or family history of premature CAD: CAC scoring
- CAC = 0: defer therapy, re-evaluate in 5–10 years
- CAC 1–99: lifestyle + consider statin based on percentile
- CAC 100–299: statin recommended; aggressive lifestyle
- CAC ≥300: statin + reassess for stress testing or CCTA if symptoms appear
Symptomatic patient with chest pain, stable:
- EKG, lipid panel, troponin if appropriate
- CCTA as first-line non-invasive imaging in most centers (per SCOT-HEART, PROMISE)
- Stress testing if CCTA shows intermediate stenosis or for functional confirmation
- Invasive catheterization if stress positive or CCTA shows severe disease
Acute chest pain or suspected ACS:
- ER evaluation, EKG, troponin
- Invasive catheterization if STEMI or high-risk NSTEMI
- Risk stratification with stress testing or CCTA in low-risk presentations
When CAC Isn't the Right Test
- Symptomatic chest pain — CCTA or stress test, not CAC alone
- Acute coronary syndrome suspected — ER evaluation, troponin, possibly cath
- Known CAD on therapy — the diagnostic question is already answered; CAC adds little
- Very low pretest probability — ASCVD < 5%; the CAC test rarely changes management
- Patients with metal artifacts (stents, pacemakers) — image quality compromised
- Elevated baseline radiation exposure concerns — though CAC's 1 mSv is modest, it's still radiation; pregnant patients should defer
Research Papers and References
- SCOT-HEART trial — PubMed search
- PROMISE trial — PubMed search
- CCTA vs stress test — PubMed search
- ApoB vs LDL-C — PubMed search
- FFR-CT — PubMed search
Connections
- Coronary Calcium Score
- ApoB
- Agatston Score Calculation and Interpretation
- Lipid Panel
- Soft Plaque and CAC Limitations
- MESA Risk Calculator and Age Percentiles
- CAC Zero and the Power of Negative Result
- Lipoprotein(a)
- Full Body MRI
- CAC in Women and Younger Adults
- Statin Threshold and CAC
- Reversal Plaque Stabilization and Lifestyle
- Chest Pain
- Atherosclerosis
- Cardiovascular Disease
- Insurance Cost and Access