Soft Plaque and CAC Zero: When a Calcium Score of Zero Isn't a Free Pass
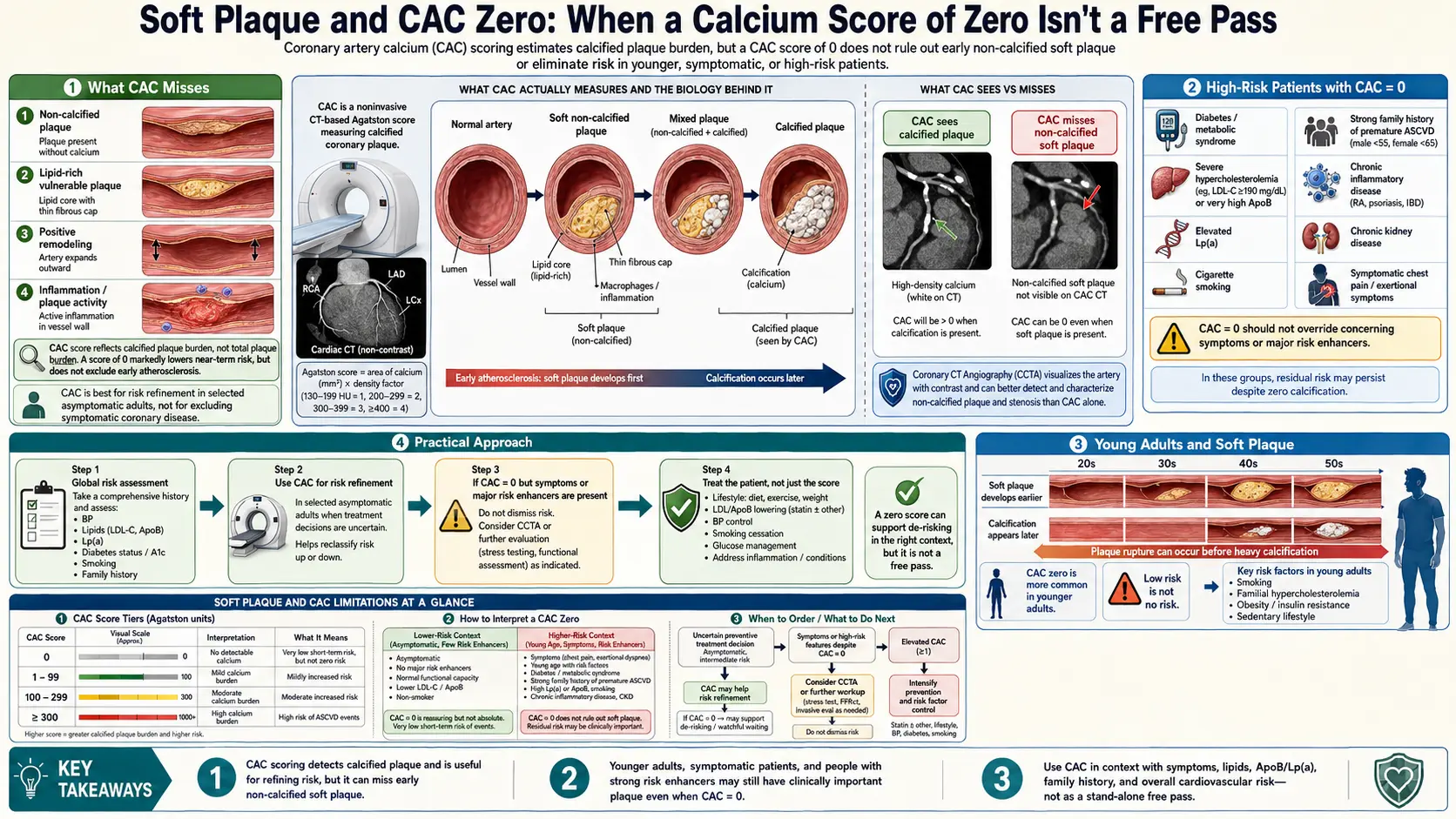
The coronary calcium score has a real blind spot: non-calcified plaque. By design, the CAC scan only detects calcified material above 130 Hounsfield Units. Mature, stable atherosclerotic plaques are calcified and show up. But early atherosclerotic lesions, the lipid-rich "vulnerable" plaques most prone to rupture, and the soft components within mixed plaques are invisible on a non-contrast CAC scan. For most middle-aged and older adults this blind spot is small — calcified plaque correlates well enough with total plaque burden to make CAC clinically useful. But there are specific populations where the blind spot matters and a calcium score of zero can mislead.
Table of Contents
- What CAC Misses
- Vulnerable Plaque
- "CAC-Zero MI"
- High-Risk Patients with CAC = 0
- CCTA as a Complement to CAC
- Young Adults and Soft Plaque
- Elevated Lp(a) and Soft Plaque
- Familial Hypercholesterolemia
- Practical Approach
- Research Papers and References
- Connections
- Featured Videos
What CAC Misses
Atherosclerosis progresses through stages, and CAC is sensitive to the late stages but not the early ones:
- Endothelial dysfunction — the earliest stage; not visible on any imaging modality
- Lipid accumulation in the artery wall — foam cells, fatty streaks; invisible on CAC
- Soft plaque formation — lipid-rich core with thin fibrous cap; invisible on CAC, visible on CCTA
- Mixed plaque — partial calcification of soft plaque; partly visible on CAC
- Mature calcified plaque — stable, dense calcification; clearly visible on CAC
CAC catches stages 4 and 5 reliably. Stages 1–3 are the soft-plaque blind spot. The good news: stages 4 and 5 are when most clinical events occur in the population, which is why CAC is such a powerful risk-stratification tool. The bad news: stages 1–3 are when the lipid-rich, vulnerable plaque most prone to acute rupture exists in greatest concentration.
Vulnerable Plaque
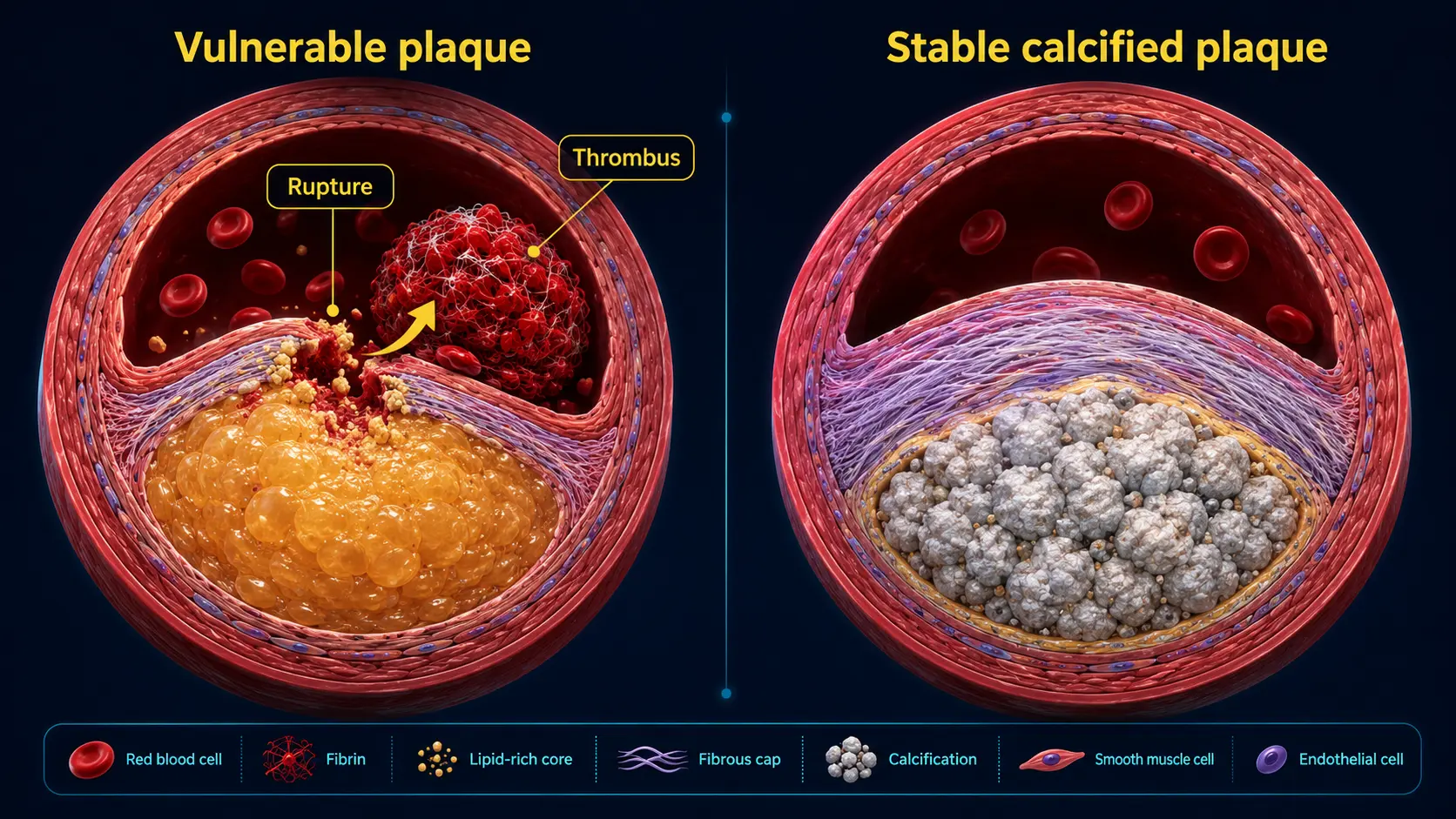
The acute coronary syndromes — STEMI, NSTEMI, unstable angina — are caused predominantly by plaque rupture, not by progressive narrowing. The plaque most likely to rupture has these features:
- Large lipid-rich core
- Thin fibrous cap (<65 µm)
- Macrophage-rich infiltrate
- Sparse smooth muscle cells
- Minimal calcification — calcification is a stabilization process
This is why high-density calcified plaque on a follow-up CAC after years of statin therapy is reassuring, while soft plaque on CCTA is worrying: density tracks stability. The Agatston score's density factor weights stable plaque higher, by design.
"CAC-Zero MI"
The "CAC-zero MI" is the rare but real phenomenon of a patient suffering an acute coronary event with a normal calcium score. Studies suggest 1–3% of MIs occur in patients with CAC = 0. Common patterns:
- Younger patients (under 50) — not enough time for calcification, but soft plaque present
- Heavy smokers — pro-thrombotic and pro-rupture independent of plaque burden
- Cocaine users — vasospasm and pro-thrombotic
- Spontaneous coronary artery dissection (SCAD) — particularly in women, peripartum
- Coronary spasm — vasospastic angina (Prinzmetal)
- Microvascular disease — especially in diabetic patients
- Familial hypercholesterolemia — soft plaque develops early
- Markedly elevated Lp(a) — pro-thrombotic, pro-inflammatory effects independent of total plaque burden
- Connective tissue or autoimmune disease — SLE, RA accelerate plaque rupture
The clinical history matters more than the test result in identifying these patients. Symptoms always override imaging.
High-Risk Patients with CAC = 0
Specific scenarios where a CAC = 0 result should not provide complete reassurance:
- Symptomatic patient with chest pain — CAC = 0 does not exclude soft-plaque-mediated ischemia or non-atherosclerotic causes; further workup (CCTA or stress test) needed
- Family history of premature CAD with FH or markedly elevated Lp(a) — consider CCTA
- Active smoker, especially with other risk factors — CAC = 0 does not negate smoking-driven event risk
- Connective tissue disease, especially SLE — consider CCTA in younger patients
- Newly diagnosed type 2 diabetes — CAC = 0 reassuring but follow-up sooner than usual
CCTA as a Complement to CAC
CT coronary angiography (CCTA) addresses the soft-plaque blind spot directly. With IV iodinated contrast and gated cardiac CT, CCTA visualizes both calcified and non-calcified plaque, vessel lumen geometry, and (with FFR-CT) the functional impact of stenoses.
When CCTA adds meaningful information beyond CAC:
- Symptomatic patients regardless of CAC result
- Asymptomatic patients with strong family history of premature CAD and CAC = 0 (rule out soft plaque)
- Asymptomatic patients with markedly elevated Lp(a) or FH with CAC = 0
- Following up an unexpectedly low CAC score that conflicts with clinical risk picture
- One-time anatomic snapshot in patients with rapid risk-factor evolution (new diabetes, sustained dyslipidemia)
Trade-offs: higher cost ($500–$2,000 vs $99–$200), higher radiation (3–10 mSv vs 1 mSv), need for IV contrast and beta-blockade, and longer scan time. CCTA is generally not appropriate as a first-line screening test in low-to-intermediate risk asymptomatic adults — CAC remains the right starting point in that population.
Young Adults and Soft Plaque
In adults under 40, atherosclerosis is often soft plaque only — calcification has not had time to develop. A CAC = 0 in a 30-year-old with strong family history may be falsely reassuring. The case for additional evaluation in young adults:
- Family history of premature CAD (male first-degree relative < 55, female < 65)
- Markedly elevated Lp(a) (> 100 nmol/L or > 50 mg/dL)
- Familial hypercholesterolemia (LDL-C > 190 mg/dL or genetically confirmed)
- Symptoms suggestive of cardiac etiology
For these patients, a complete picture often requires lipid markers (ApoB, Lp(a)), genetic testing where appropriate, and consideration of CCTA. CAC alone is not sufficient.
Elevated Lp(a) and Soft Plaque
Lipoprotein(a) is a genetically determined LDL-like particle linked to apolipoprotein(a). Elevated Lp(a) is associated with:
- Increased pro-thrombotic activity (apolipoprotein(a) shares structural homology with plasminogen)
- Inflammatory and oxidative effects on the arterial wall
- Accelerated atherosclerosis even at "normal" LDL-C
- Calcific aortic valve stenosis in older age
- An event-rate increase even at low CAC scores
Patients with markedly elevated Lp(a) (above 100 nmol/L or 50 mg/dL) may have normal or low CAC scores yet substantial soft-plaque burden. CCTA may be warranted, and lipid management should be aggressive (LDL-C targets below standard population goals).
Familial Hypercholesterolemia
Familial hypercholesterolemia is a genetic disorder (typically LDLR, APOB, or PCSK9 mutations) causing severely elevated LDL-C from birth. FH patients develop atherosclerosis decades earlier than the general population, often with substantial soft-plaque burden by their 30s. CAC scoring in FH:
- Detects calcified plaque progression earlier than non-FH controls
- Underestimates total burden because soft plaque dominates in younger FH patients
- Should be combined with CCTA evaluation in young or symptomatic FH patients
- Should not be used to defer therapy — FH patients need lifelong intensive lipid-lowering regardless of imaging
Practical Approach
For the typical asymptomatic middle-aged adult:
- Lipid panel, ApoB, Lp(a) once
- ASCVD risk calculation
- CAC if intermediate risk or family history
- Manage based on integrated picture
For the high-risk asymptomatic patient (FH, markedly elevated Lp(a), strong premature CAD family history):
- Lipid panel, ApoB, Lp(a) once
- Comprehensive risk assessment
- CAC scoring
- If CAC > 0, manage as appropriate
- If CAC = 0 but high baseline genetic/lipid risk: consider CCTA to rule out soft plaque
- Manage aggressively regardless of imaging if FH or high Lp(a)
For the symptomatic patient at any age: CAC alone is not the right test — CCTA, stress test, or invasive evaluation as clinically indicated. See the CAC vs Other Tests page.
Research Papers and References
- Soft plaque and CCTA — PubMed search
- CAC = 0 MI — PubMed search
- Lp(a) and soft plaque — PubMed search
- FH and coronary imaging — PubMed search
- Vulnerable plaque biology — PubMed search
Connections
- Coronary Calcium Score
- CAC vs Other Cardiac Tests
- Agatston Score Calculation and Interpretation
- ApoB
- CAC Zero and the Power of Negative Result
- CAC in Women and Younger Adults
- Statin Threshold and CAC
- MESA Risk Calculator and Age Percentiles
- Reversal Plaque Stabilization and Lifestyle
- Lipoprotein(a)
- Lipid Panel
- Atherosclerosis
- Chest Pain
- Full Body MRI
- Insurance Cost and Access