BUN (Blood Urea Nitrogen): Reference Ranges and Interpretation
Blood urea nitrogen (BUN) measures the amount of nitrogen carried in serum urea — the principal nitrogen-containing waste product of protein metabolism. It is one of the oldest, cheapest, and most widely ordered kidney tests, included on virtually every basic and comprehensive metabolic panel. BUN is sensitive to many things besides kidney function, which makes it less specific than creatinine but uniquely useful for spotting prerenal states (dehydration, GI bleed, heart failure) and the metabolic consequences of high-protein intake or catabolic stress.
Table of Contents
- What Urea Is and Where It Comes From
- Reference Range
- Why BUN Changes (Beyond Kidney Function)
- Causes of High BUN
- Causes of Low BUN
- BUN-to-Creatinine Ratio
- BUN vs Creatinine vs eGFR
- Preparation and Specimen
- Optimizing BUN: Hydration, Protein, Medications
- Research Papers and References
- Connections
- Featured Videos
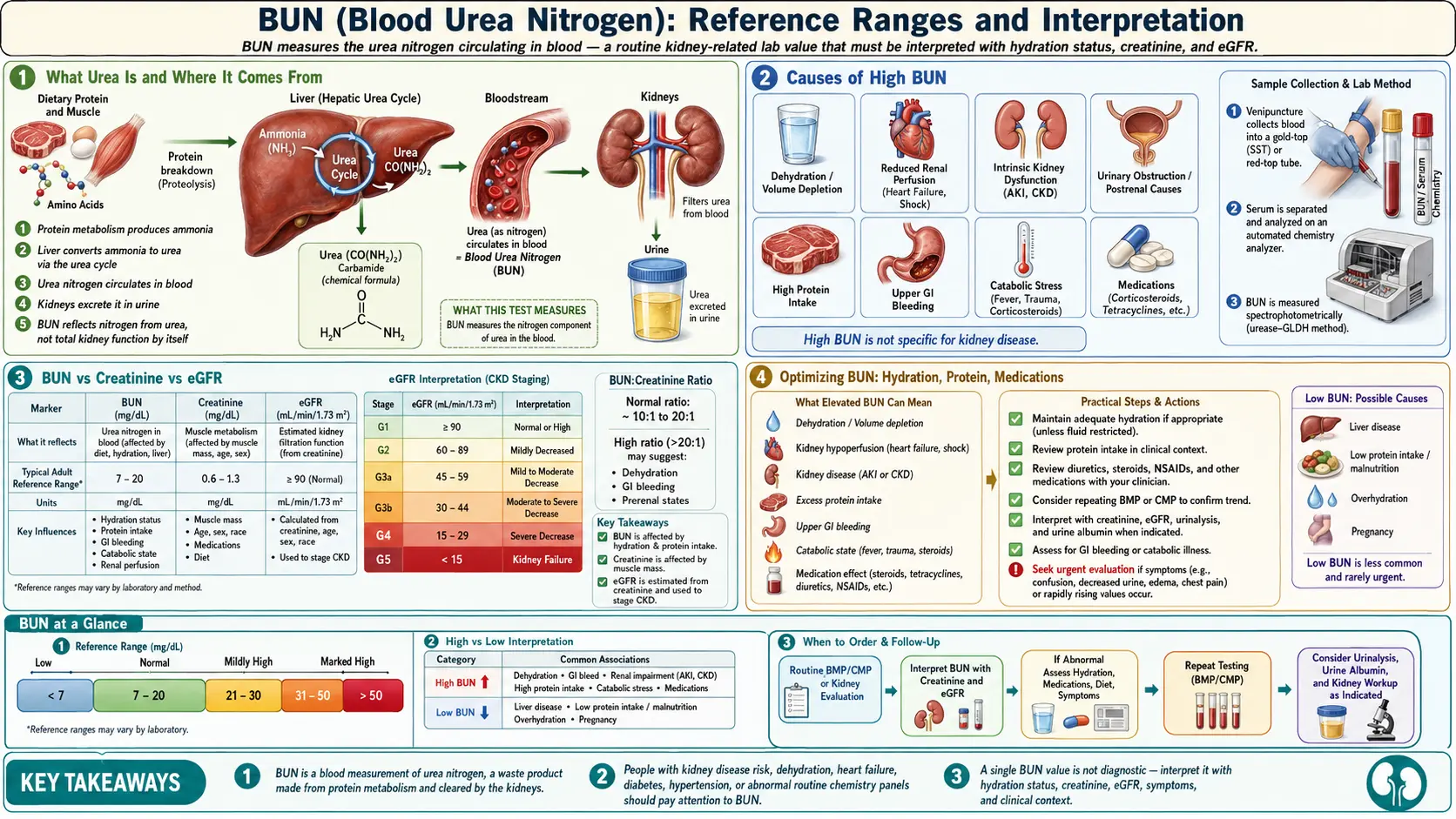
What Urea Is and Where It Comes From
When the body breaks down dietary or tissue protein, the resulting amino acids are deaminated — their nitrogen is split off as ammonia (NH₃). Ammonia is toxic, particularly to the brain, so the liver immediately runs it through the urea cycle, converting it to urea (CH₄N₂O), which is non-toxic and water-soluble. The kidneys filter urea at the glomerulus, reabsorb a variable fraction in the proximal tubule (more when dehydrated, less when over-hydrated), and excrete the rest in urine.
BUN measures only the nitrogen content of urea (each urea molecule contains two nitrogens), so the number is roughly half of the actual urea concentration. A BUN of 14 mg/dL corresponds to about 30 mg/dL of urea. Most US labs report BUN; UK and most European labs report serum urea directly.
Reference Range
BUN (mg/dL)
Adult reference ranges vary slightly between laboratories but typically fall around 7–20 mg/dL (2.5–7.1 mmol/L of urea). Children have lower normal ranges; ranges drift upward in older adults due to the combination of declining renal reserve and reduced lean body mass affecting creatinine more than BUN. Pregnancy lowers BUN by about 25% (increased plasma volume, increased GFR).
Why BUN Changes (Beyond Kidney Function)
BUN is influenced by three independent processes:
- Production — how much nitrogen the liver is converting to urea. Driven by dietary protein, GI bleeding (digested blood is a high-protein meal), corticosteroids, fever, infection, surgery, trauma, and severe burns (catabolism). Reduced by very-low-protein diets, severe malnutrition, and advanced liver disease (impaired urea synthesis).
- Filtration — how much the glomerulus is removing per minute. Driven by GFR, which falls with age, dehydration, heart failure, kidney disease, and renal artery stenosis.
- Reabsorption — how much urea the proximal tubule pulls back into the bloodstream. Increases with dehydration and ADH-driven water reabsorption (a classic prerenal pattern).
This is why BUN is best read in the context of creatinine. A BUN of 35 with creatinine of 0.9 (ratio 39) tells a very different story than a BUN of 35 with creatinine of 3.5 (ratio 10).
Causes of High BUN
Prerenal (kidney is fine, perfusion is not)
- Dehydration — the most common cause of mildly elevated BUN. Increased ADH causes greater tubular urea reabsorption.
- Heart failure — reduced cardiac output lowers renal perfusion; BUN often disproportionately high vs creatinine.
- Hemorrhage, GI bleed — volume loss plus a "protein meal" of digested blood.
- Sepsis, shock — reduced renal perfusion plus catabolic state.
- NSAIDs and ACE inhibitors — alter glomerular hemodynamics, especially in volume-depleted patients.
Renal (kidney itself is damaged)
- Acute kidney injury (any cause)
- Chronic kidney disease (CKD) — BUN typically tracks creatinine
- Glomerulonephritis, interstitial nephritis
- Polycystic kidney disease
Postrenal (obstruction)
- Bladder outlet obstruction (BPH, prostate cancer)
- Ureteral obstruction (stones, retroperitoneal fibrosis, malignancy)
- Neurogenic bladder
Increased urea production (kidney is fine, more nitrogen to excrete)
- Very high protein intake (carnivore diet, post-workout protein loading)
- Corticosteroid therapy (prednisone, dexamethasone) — catabolic effect
- Hyperthyroidism
- Tetracycline antibiotics — rare but classic; reduce protein synthesis
- Severe trauma, burns, major surgery, sepsis
Causes of Low BUN
- Low protein intake — vegan or strict vegetarian diet, anorexia, malnutrition
- Liver disease — impaired urea synthesis (cirrhosis, severe hepatitis); ammonia rises while urea falls
- Pregnancy — physiologic; increased plasma volume and GFR
- Overhydration / SIADH — dilution and increased GFR
- Anabolic states — large doses of anabolic steroids or growth hormone diverting nitrogen into protein synthesis
Importantly, a low BUN by itself is rarely worrisome; it usually reflects diet or hydration. Low BUN with elevated ammonia or jaundice points to liver dysfunction.
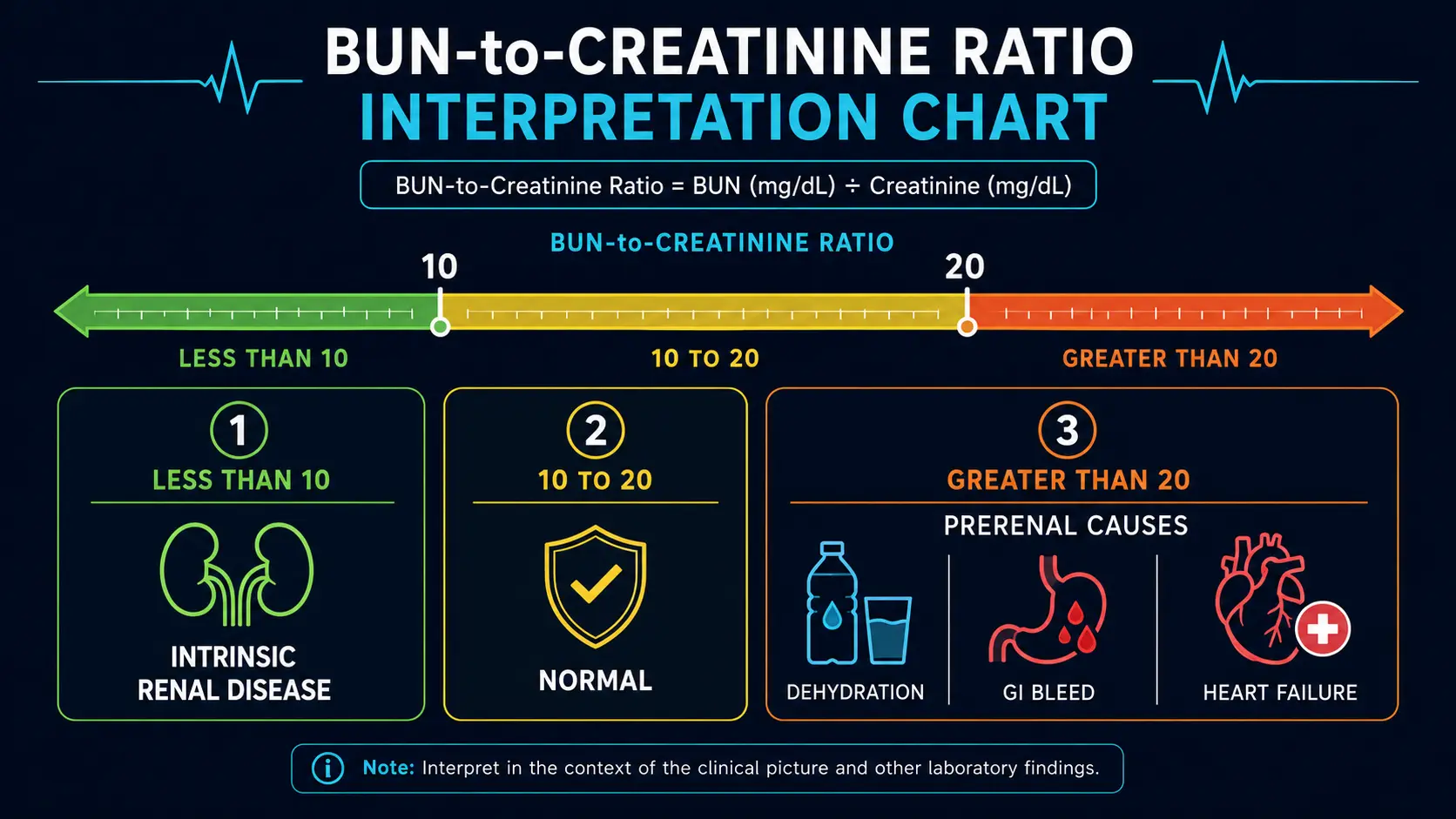
BUN-to-Creatinine Ratio
Dividing BUN by creatinine (both in mg/dL) gives a ratio that helps localize the problem.
BUN : Creatinine ratio
A ratio above 20 with normal or only mildly elevated creatinine almost always means prerenal — rehydrate, treat the underlying volume problem, and recheck. A ratio above 30 in the setting of black, tarry stools is highly suggestive of an upper GI bleed even before the hemoglobin drops.
A ratio below 10 with elevated creatinine usually means intrinsic renal disease (acute tubular necrosis, advanced CKD), severe malnutrition, or advanced liver disease.
BUN vs Creatinine vs eGFR
Each test brings something different:
- BUN — sensitive but non-specific; best for detecting prerenal patterns and dietary or catabolic effects
- Creatinine — the workhorse; tracks GFR closely once established but lags in early CKD because of "creatinine blind range" up to ~50% nephron loss
- eGFR — calculated from creatinine; the variable used to stage CKD
- Cystatin C — alternative filtration marker; better in non-standard body composition (frail, athletes, amputees)
For most routine outpatient screening, the BUN + creatinine + eGFR triad is sufficient. Add cystatin C when creatinine-based eGFR seems implausible for the patient's body habitus, or when early CKD detection matters (diabetes, family history of polycystic kidney disease).
Preparation and Specimen
- Fasting: not strictly required, but typically drawn fasting because BUN is part of the comprehensive metabolic panel that also reports glucose
- Tube: serum separator tube (gold-top SST) or lithium heparin (green-top)
- Stability: stable at room temperature for 24 hours, refrigerated 7 days, frozen indefinitely
- Hydration: avoid heavy water-loading just before the draw — can artificially lower BUN
- Recent high-protein meal or workout: can transiently raise BUN; if a borderline result matters, repeat under standard conditions
Optimizing BUN: Hydration, Protein, Medications
If your BUN is mildly elevated and your eGFR is normal:
- Drink more water — aim for pale-yellow urine; in healthy adults, 30–35 mL/kg/day is a reasonable starting point. Around heavy exercise or hot weather, increase further.
- Match protein intake to activity — healthy adults tolerate 1.0–1.6 g/kg/day without consequence. Strict carnivore or 250 g/day intake will reliably push BUN above the reference range without indicating disease.
- Review medications — chronic NSAID use is the most common culprit Americans miss. Steroids, lithium, and aminoglycosides also contribute.
- Treat heart failure aggressively — if BUN climbs while creatinine stays flat, the cardiologist should be involved; SGLT2 inhibitors and judicious diuresis often help both organs.
If your BUN is elevated and creatinine is rising, the issue is no longer dietary — this is the time to read the Creatinine and eGFR pages and to ask your physician about urine ACR and a renal ultrasound.
Research Papers and References
- BUN and kidney function — PubMed search
- BUN-to-creatinine ratio in prerenal azotemia — PubMed search
- Urea cycle and protein metabolism — PubMed search
- BUN as a prognostic marker in heart failure — PubMed search
- High-protein diet and BUN — PubMed search
- Upper GI bleed and BUN/Cr ratio — PubMed search
External Authoritative Resources
Connections
- Creatinine
- eGFR
- Cystatin C
- Kidney Function Tests
- Comprehensive Metabolic Panel
- Urinalysis
- Kidney Disease
- Acute Kidney Injury
- Heart Failure
- Liver Disease
- Glomerulonephritis
- Cirrhosis
- Sepsis
- Diabetes