Kidney Function Tests: BUN, Creatinine, eGFR, and Cystatin C
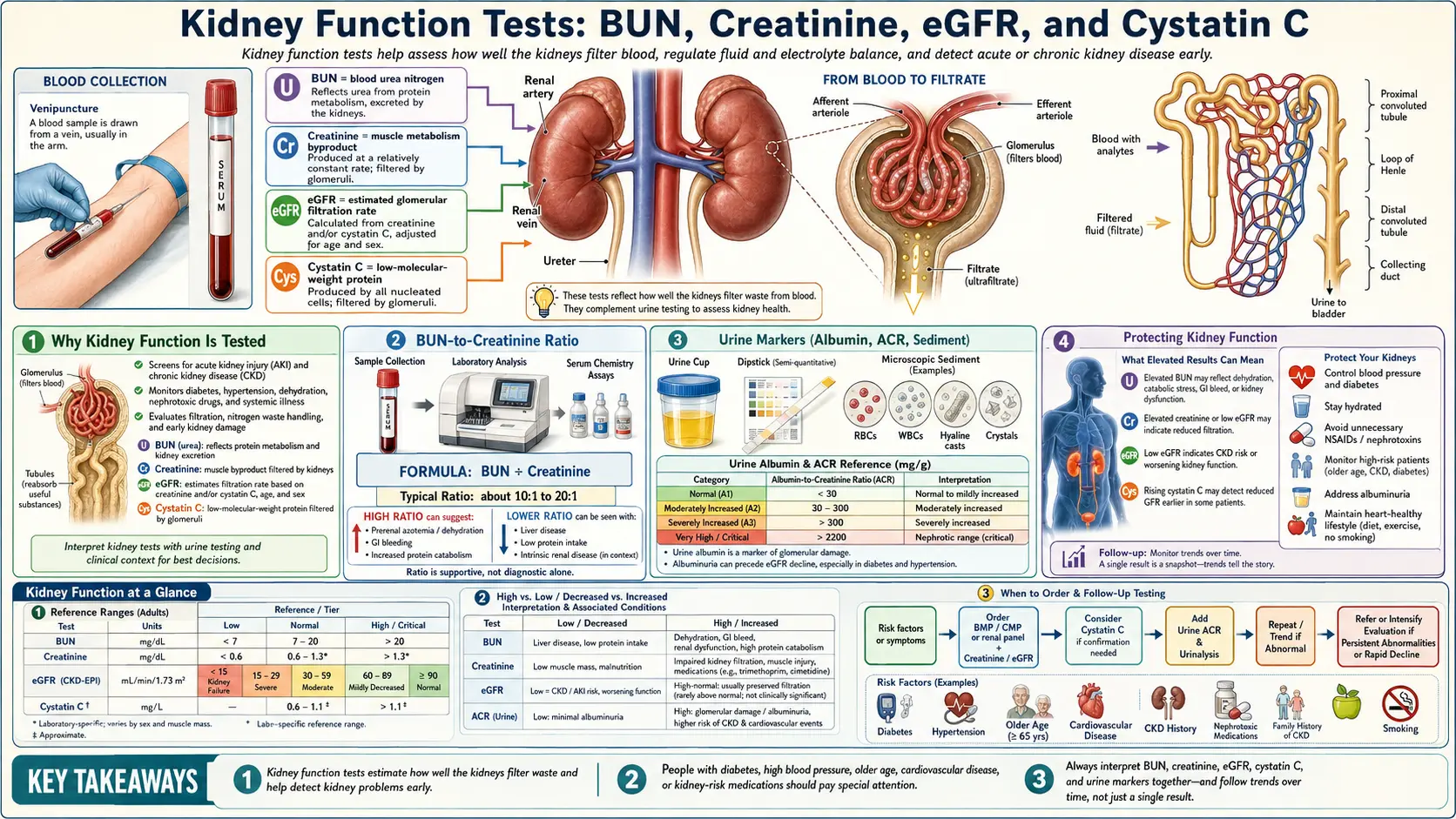
Kidney function tests are a small group of inexpensive blood markers that estimate how effectively the kidneys are filtering metabolic waste from the blood. The four core measurements — blood urea nitrogen (BUN), creatinine, the estimated glomerular filtration rate (eGFR), and cystatin C — appear on every comprehensive metabolic panel and most annual physicals. Together with urinalysis (urine albumin, urine creatinine, urine sediment), they form the diagnostic backbone for screening, staging, and monitoring chronic kidney disease (CKD), acute kidney injury (AKI), and many systemic conditions that secondarily affect the kidneys.
Table of Contents
- Why Kidney Function Is Tested
- What the Kidney Does
- The Four Core Tests
- BUN-to-Creatinine Ratio
- CKD Staging Using eGFR
- Urine Markers (Albumin, ACR, Sediment)
- Beyond the Standard Panel
- When to Worry: Red-Flag Patterns
- Protecting Kidney Function
- Research Papers and References
- Connections
Why Kidney Function Is Tested
Chronic kidney disease affects an estimated 14% of US adults, yet most cases go undiagnosed until function has fallen below 50%. The kidneys have enormous functional reserve: a person can lose roughly half their nephrons before serum creatinine and eGFR begin to shift outside the reference range. This means routine kidney function tests are screening tools as much as diagnostic ones — the goal is to catch decline before it becomes symptomatic.
Specific situations that prompt or intensify kidney testing:
- Annual screening in adults, especially after age 50 or when other cardiovascular risk factors are present
- Diabetes — the leading cause of CKD; annual eGFR and urine albumin-to-creatinine ratio (ACR) testing is standard
- Hypertension — the second leading cause of CKD; high blood pressure both damages kidneys and is worsened by failing kidneys
- Cardiovascular disease, heart failure — cardiorenal syndrome; reduced kidney perfusion drives renal decline
- Medication monitoring — before and during use of NSAIDs, ACE inhibitors/ARBs, contrast dye, lithium, aminoglycosides, vancomycin, methotrexate, and many chemotherapy agents
- Family history of polycystic kidney disease, IgA nephropathy, or congenital kidney disease
- Acute illness — sepsis, dehydration, post-surgical states, contrast exposure, rhabdomyolysis
- Symptoms — foamy urine, blood in urine, persistent edema, unexplained fatigue, decreased urine output, flank pain
What the Kidney Does
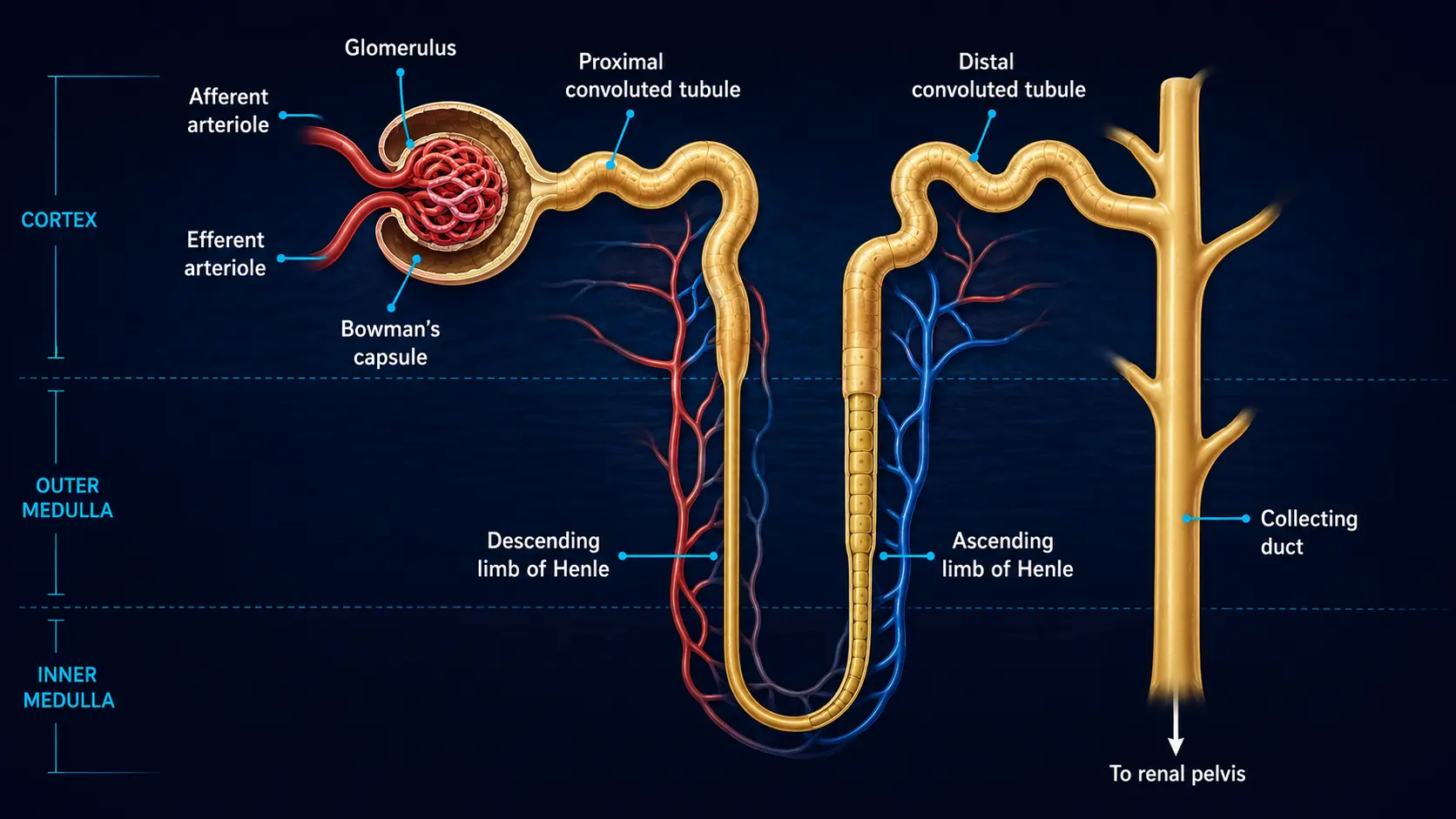
Each kidney contains roughly one million microscopic filtering units called nephrons. Every minute the kidneys filter about 125 mL of plasma through the glomerular capillaries, producing roughly 180 liters of filtrate per day. Of that volume, more than 99% is reabsorbed; the remaining 1.5–2 L exits as urine. The kidneys also secrete erythropoietin (which stimulates red blood cell production), activate vitamin D (1,25-dihydroxyvitamin D), regulate blood pressure via the renin-angiotensin-aldosterone system, balance sodium, potassium, calcium, phosphate and acid-base chemistry, and excrete drugs and metabolic waste.
This is why kidney decline is rarely "just a kidney problem." Worsening function shows up as anemia (low erythropoietin), bone disease (impaired vitamin D activation, phosphate retention), refractory hypertension, hyperkalemia, metabolic acidosis, and accumulation of medications normally cleared renally.
The Four Core Tests
Each of the four standard kidney function markers measures a slightly different physiologic process. None is perfect on its own — they are most useful together.
BUN (Blood Urea Nitrogen)
Urea is the nitrogen-containing waste product of protein metabolism in the liver. The kidneys filter and excrete it; some is reabsorbed in the proximal tubule. BUN reflects both kidney function and hydration, dietary protein, and tissue catabolism. Useful but non-specific. Read the full BUN page →
Creatinine
Creatinine is a waste product of muscle metabolism (creatine breakdown). It is produced at a relatively constant rate proportional to muscle mass and is freely filtered by the glomerulus with minimal tubular reabsorption. Creatinine is the workhorse of routine kidney testing — cheap, automated, available everywhere — but it is influenced by muscle mass, age, sex, ethnicity, dietary creatine, and certain medications. Read the full Creatinine page →
eGFR (estimated Glomerular Filtration Rate)
eGFR is not measured directly. It is calculated from serum creatinine using a formula (most commonly the 2021 race-free CKD-EPI equation), with inputs of age and sex. It estimates how many milliliters of blood per minute the kidneys are clearing of creatinine, normalized to a body surface area of 1.73 m². eGFR is what defines CKD stages (G1–G5). Read the full eGFR page →
Cystatin C
Cystatin C is a small protein produced by all nucleated cells at a steady rate, freely filtered by the glomerulus, and almost completely metabolized by the proximal tubule. Unlike creatinine, it is largely independent of muscle mass, age, sex, and diet. It detects mild renal impairment earlier than creatinine and refines eGFR in patients with non-standard body composition (frail elderly, amputees, athletes, bodybuilders). Read the full Cystatin C page →
BUN-to-Creatinine Ratio
The ratio of BUN to creatinine helps distinguish three broad patterns of kidney dysfunction:
BUN : Creatinine ratio (typical units, mg/dL : mg/dL)
A high BUN-to-creatinine ratio with normal creatinine usually points to a prerenal cause — the kidneys themselves are healthy but are being asked to work against poor perfusion (dehydration, blood loss, heart failure) or an unusually high nitrogen load (gastrointestinal bleed releasing protein into the gut, very-high-protein diet, corticosteroid-induced catabolism). A low BUN-to-creatinine ratio with elevated creatinine suggests intrinsic renal disease (the kidneys themselves are damaged), severe malnutrition, or advanced liver disease (impaired urea synthesis).
CKD Staging Using eGFR
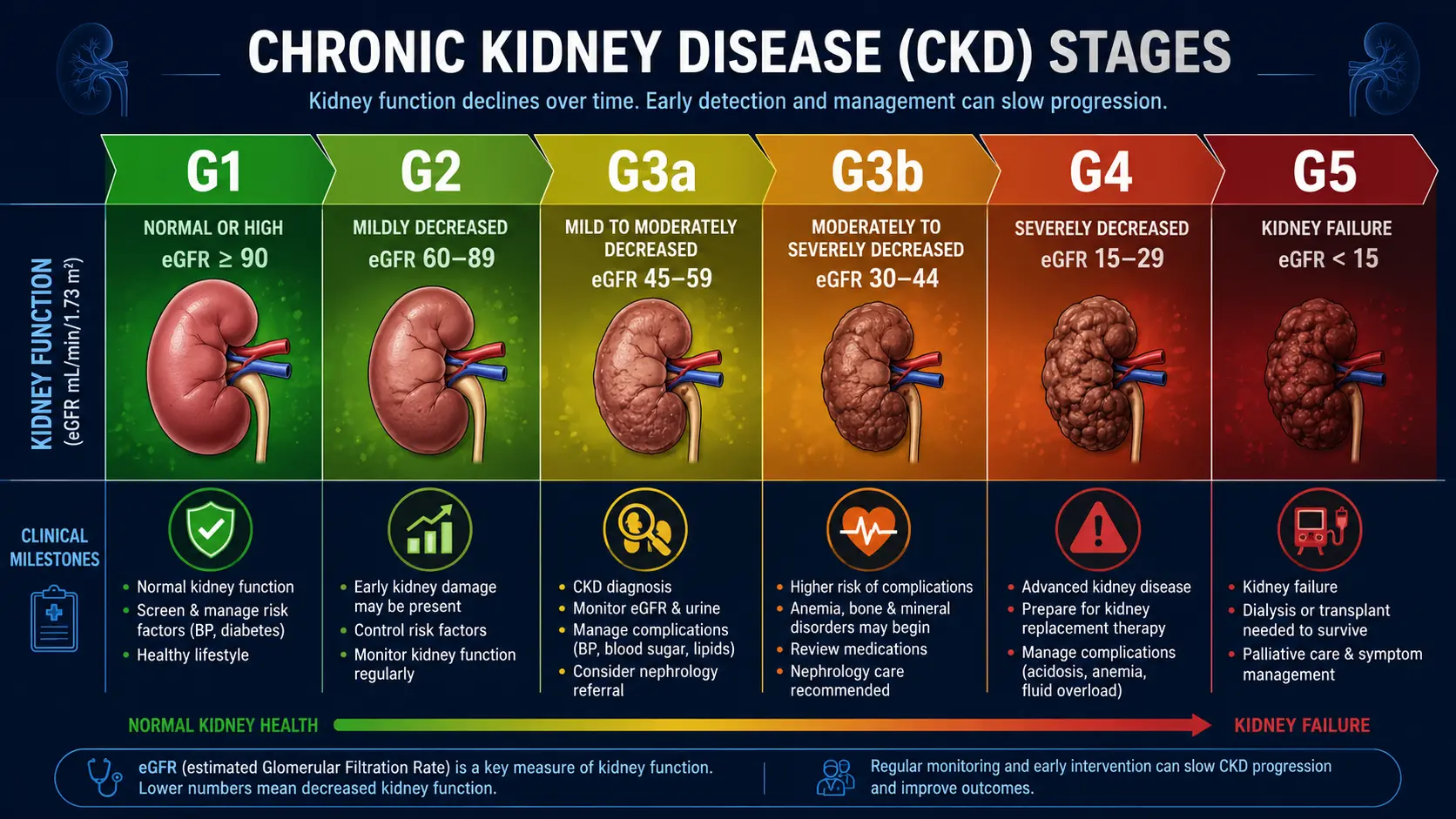
Chronic kidney disease is staged by the worst of either eGFR or albuminuria sustained for at least three months. The G stages (G for GFR) come from the 2012 KDIGO guidelines:
- G1 — eGFR ≥ 90 mL/min/1.73 m²: normal or high. Considered CKD only if there is also albuminuria, structural abnormality on imaging, or a known kidney disorder.
- G2 — eGFR 60–89: mildly decreased. Same caveat as G1 — mild eGFR drop alone does not equal CKD.
- G3a — eGFR 45–59: mildly to moderately decreased. The threshold at which CKD is diagnosed regardless of other findings.
- G3b — eGFR 30–44: moderately to severely decreased. Anemia, bone-mineral disease, and cardiovascular risk start to climb.
- G4 — eGFR 15–29: severely decreased. Nephrology referral and pre-dialysis planning are standard.
- G5 — eGFR < 15: kidney failure. Dialysis or transplant evaluation.
Albuminuria adds an A stage: A1 (urine ACR < 30 mg/g), A2 (30–300), A3 (> 300). Combined G/A staging predicts cardiovascular events, progression to dialysis, and all-cause mortality more accurately than either marker alone.
Urine Markers (Albumin, ACR, Sediment)
Blood-based markers tell you how much filtration is happening; urine markers tell you whether the filter itself is intact. The two key urine measurements:
- Urine albumin-to-creatinine ratio (ACR) — on a single random sample. Healthy glomeruli are nearly impermeable to albumin; persistent leakage indicates glomerular damage. ACR is the earliest detectable marker of diabetic kidney disease, often abnormal years before eGFR changes.
- Urinalysis (UA) with microscopy — dipstick screens for blood, protein, glucose, leukocyte esterase, nitrites, and pH. Microscopy looks for red cells, white cells, casts (cellular, granular, waxy), and crystals. Red cell casts strongly suggest glomerulonephritis; muddy brown casts suggest acute tubular necrosis.
See Urinalysis → for a deeper walkthrough.
Beyond the Standard Panel
When the routine markers raise concern, a nephrologist may order:
- Renal ultrasound — size, echogenicity, hydronephrosis, cysts, stones
- Urine sodium and FENa (fractional excretion of sodium) — distinguishes prerenal from intrinsic AKI
- Serum and urine electrophoresis with free light chains — rules out multiple myeloma, light-chain disease
- ANA, ANCA, anti-GBM, complement (C3/C4), ASO — autoimmune and post-infectious glomerulonephritis
- Hepatitis B/C, HIV serology — viral nephropathies
- 24-hour urine collection — proteinuria quantification, creatinine clearance, stone-risk profile
- Kidney biopsy — the gold standard for diagnosing intrinsic glomerular and tubulointerstitial disease
When to Worry: Red-Flag Patterns
- Creatinine rising by > 0.3 mg/dL within 48 hours — meets the KDIGO definition of acute kidney injury (AKI)
- eGFR dropping more than 5 mL/min/yr — rapid progressive CKD; warrants nephrology referral
- Persistent ACR > 300 mg/g — significant proteinuria; aggressive blood-pressure and SGLT2-inhibitor management
- Hematuria with proteinuria — suspect glomerulonephritis
- Oliguria (< 400 mL/day) or anuria — medical emergency
- Hyperkalemia > 6.0 mmol/L — cardiac risk; immediate evaluation
Protecting Kidney Function
For most people, kidney protection means doing the boring things consistently:
- Tight blood pressure control — goal < 130/80 in most CKD patients; ACE inhibitors or ARBs preferred for proteinuria
- Tight glycemic control in diabetes — A1c around 7%; SGLT2 inhibitors (empagliflozin, dapagliflozin) and GLP-1 agonists slow progression independent of glucose lowering
- Avoid chronic NSAIDs — ibuprofen, naproxen, diclofenac; even short courses can precipitate AKI in dehydration or low perfusion states
- Adequate hydration — especially around contrast studies, intense exercise, or hot weather
- Limit nephrotoxic herbal products — aristolochic acid (some Chinese herbal preparations), high-dose vitamin C in stone formers, excessive licorice
- Treat sleep apnea — nocturnal hypoxia accelerates kidney decline
- Smoking cessation, weight management, regular exercise — same fundamentals as cardiovascular protection
- Watch the medication list — PPIs, lithium, calcineurin inhibitors, certain antibiotics; periodic medication review with your physician
For supplements that may help, see the Magnesium, Vitamin D3, and Berberine pages. For diabetes-specific kidney protection, Blood Sugar protocols and anti-inflammatory diet are evidence-supported starting points.
Research Papers and References
The following are curated PubMed literature searches covering kidney function testing and chronic kidney disease management. Each link opens a live, filtered query so the results stay current as new studies are indexed.
- 2021 race-free CKD-EPI equation — PubMed search
- Cystatin C for kidney function — PubMed search
- BUN-to-creatinine ratio interpretation — PubMed search
- Urine albumin-to-creatinine ratio — PubMed search
- KDIGO CKD staging guidelines — PubMed search
- SGLT2 inhibitors and CKD progression — PubMed search
- Acute kidney injury (KDIGO) — PubMed search
- NSAIDs and kidney injury — PubMed search
External Authoritative Resources
- National Kidney Foundation — Blood Tests for Kidney Function
- KDIGO Guidelines — Global Kidney Disease Reference
- NIDDK — Kidney Disease Information (NIH)
Connections
- BUN
- Creatinine
- eGFR
- Cystatin C
- Urinalysis
- Comprehensive Metabolic Panel
- Uric Acid
- Kidney Disease
- Acute Kidney Injury
- Glomerulonephritis
- Nephrotic Syndrome
- Heart Failure
- Hypertension
- Diabetes
- Creatine
- Magnesium
- Vitamin D3
- Anti-Inflammatory Diet