The Gerson Detoxification Theory
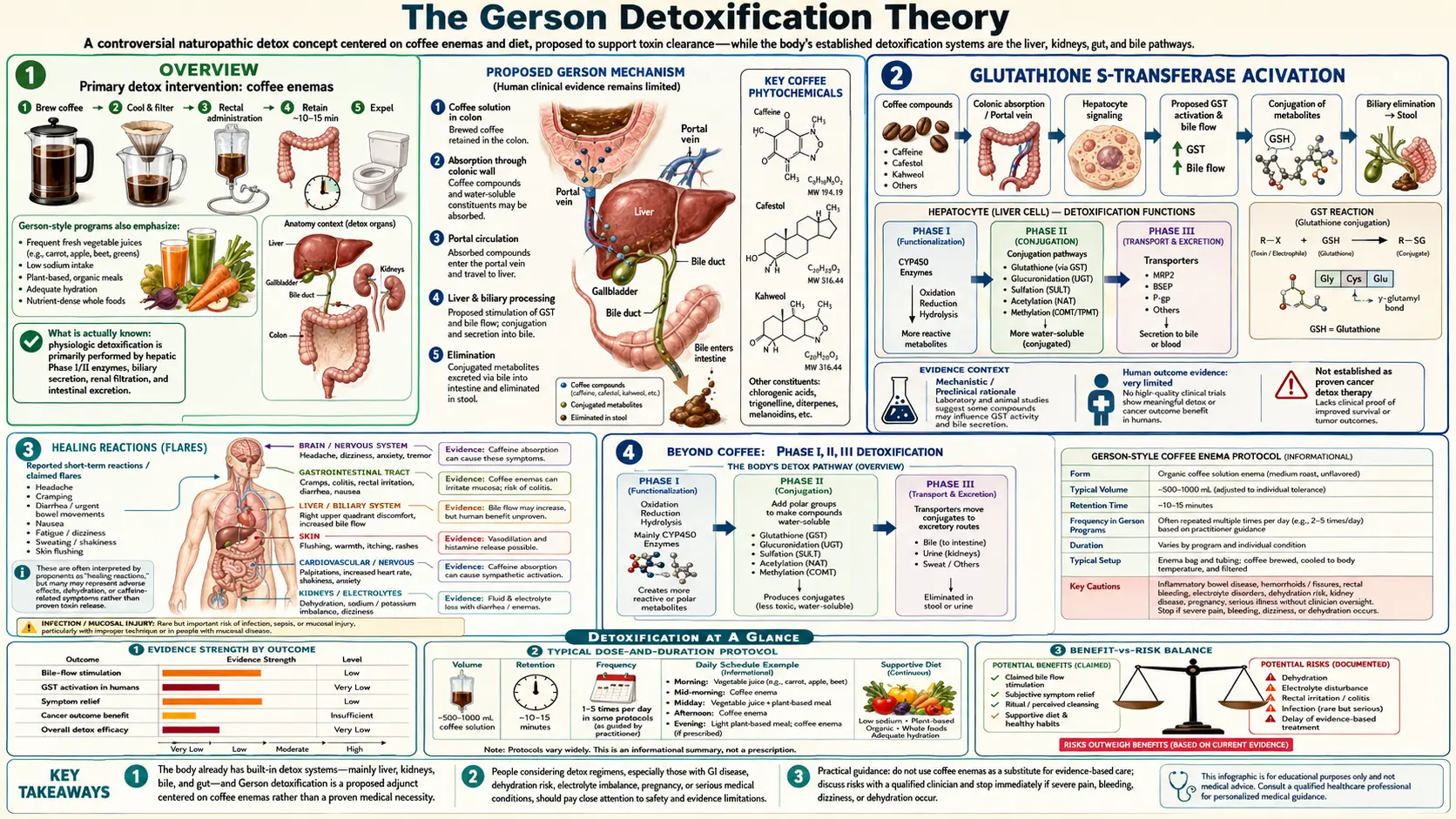
Table of Contents
- Overview
- The “Tissue Damage Syndrome”
- Bile Flow and the Cholagogue Effect
- Glutathione S-Transferase Activation
- Palmitates, Kahweol, and Cafestol
- Portal Circulation Hypothesis
- Healing Reactions (Flares)
- What Modern Hepatology Actually Says
- Oral Coffee versus Rectal Coffee
- Beyond Coffee: Phase I, II, III Detoxification
- Key Research and Sources
- Featured Videos
Overview
The detoxification theory is the conceptual core of the Gerson Therapy. Gerson believed that chronic disease, particularly cancer, was the body’s expression of an overloaded detoxification system — that diseased and dying cells, environmental toxins, and the byproducts of failed metabolism accumulated faster than the liver could neutralize and excrete them. The therapy’s job was to reduce inputs (the diet) and accelerate outputs (the enemas), giving the liver a chance to catch up.
Some elements of this framing align well with current biochemistry. The liver does perform Phase I oxidation, Phase II conjugation, and Phase III biliary excretion. Plant phytochemicals do upregulate glutathione synthesis. Bile flow is the primary route of fat-soluble waste excretion. Other elements — the idea that “toxins” accumulate in tissues until purged, the idea that the liver’s detoxification capacity can be measured by clinical “healing reactions,” the idea that rectal coffee delivers compounds to the liver in clinically meaningful concentrations — remain unsupported by direct human evidence.
The “Tissue Damage Syndrome”
Gerson described what he called the “tissue damage syndrome” — a generalized condition in chronic disease patients in which cells leak intracellular potassium and accumulate sodium, mitochondrial respiration is impaired, and oxidative stress markers rise. The clinical features he attributed to this syndrome included fatigue, edema, intolerance of fat, intolerance of caffeine taken orally, sensitivity to environmental odors, food intolerance, and slowed wound healing.
Modern equivalents of this clinical picture exist under different labels — mitochondrial dysfunction, chronic inflammation, low-grade systemic oxidative stress — but the consolidated “tissue damage syndrome” concept did not survive into mainstream medicine. The constellation of symptoms Gerson described is real; the unifying mechanism he proposed is not a recognized clinical entity.
Bile Flow and the Cholagogue Effect
The bile flow argument is the most concrete biochemical claim in the Gerson detoxification theory. Caffeine, theophylline, and theobromine — the three methylxanthines in coffee — are smooth-muscle relaxants. Theophylline in particular relaxes the sphincter of Oddi, the muscular ring at the junction of the common bile duct and the duodenum. Relaxing the sphincter allows bile that has been concentrated in the gallbladder to flow more freely into the small intestine. The same effect is exploited in clinical hepatology when theophylline derivatives are used as cholagogues (bile flow stimulants).
What is not established is whether rectal administration of coffee delivers methylxanthines to the liver and biliary system at concentrations sufficient to produce a clinically meaningful cholagogue effect. The case-report-level evidence that the urge to defecate after a coffee enema is often associated with the passage of bile-tinted material is consistent with bile flow, but is not proof of clinically meaningful detoxification.
Glutathione S-Transferase Activation
The most-cited single piece of mechanistic biochemistry behind the Gerson coffee enema is the in vitro and animal evidence that compounds in coffee, particularly the diterpenes kahweol and cafestol, upregulate hepatic glutathione S-transferase (GST) activity. GST is the central Phase II detoxification enzyme. It conjugates reactive electrophiles (including many drug metabolites and a number of carcinogens) with glutathione, rendering them water-soluble and excretable in bile and urine.
The animal data — mostly rodent studies from the 1980s and 1990s — do show measurable GST induction with oral coffee diterpenes. Whether the same upregulation occurs with rectally administered coffee in humans, and whether the magnitude of induction is clinically meaningful, has not been established. The Gerson literature treats the rodent data as definitive; mainstream hepatology treats it as suggestive but unconfirmed.
Palmitates, Kahweol, and Cafestol
Kahweol and cafestol are diterpene fatty acid esters present primarily in the unfiltered oil layer of brewed coffee. Drip-filtered coffee removes most of them; French-press, Turkish, espresso, and the simmered-not-pressed Gerson enema brew preserve them. They are the same compounds that raise serum cholesterol when consumed orally in unfiltered coffee — an important fact for anyone using rectal administration of unfiltered coffee chronically.
The Gerson literature emphasizes the GST-inducing and chemoprotective profiles of these compounds. The cardiology literature emphasizes their LDL-cholesterol-raising profile. Both characterizations are correct and apply at the same time; whether the net effect is favorable depends on the patient and the duration of exposure.
Portal Circulation Hypothesis
One of the most distinctive Gerson claims is that rectally administered substances reach the liver in a more concentrated form than orally administered substances, because the rectal venous drainage joins the portal circulation. The anatomy is partially true: the superior rectal vein drains into the inferior mesenteric vein, which joins the portal system. The middle and inferior rectal veins drain into systemic circulation through the internal iliacs. So rectally absorbed substances enter both portal and systemic circulation, with the proportion depending on how distally in the rectum the substance is absorbed.
What is not established is that the portal-vein delivery in this scenario is high enough to produce hepatic compound concentrations meaningfully greater than those from oral coffee, given the very different absorption kinetics from the rectal mucosa versus the gastrointestinal tract. The pharmacokinetics of rectal caffeine absorption have been studied; the kinetics of rectal kahweol and cafestol have not.
Healing Reactions (Flares)
Gerson described “healing reactions,” later sometimes called “detox reactions” or “flares,” as transient worsening of symptoms that he interpreted as evidence of accelerated detoxification. These typically include headache, nausea, fatigue, body aches, low-grade fever, mood changes, and sometimes a worsening of the patient’s primary symptom (skin lesion flare in tuberculosis patients, increased pain at a tumor site in cancer patients) for one to several days.
From a Gerson framing, healing reactions are evidence the protocol is working. From a mainstream pharmacology framing, similar symptoms are described as Herxheimer-like reactions and are well documented in some specific contexts (initiation of antibiotic therapy in spirochetal infection, for instance) but should not be treated as a marker of treatment efficacy in general. Patients should be cautious about interpreting symptom flares as proof of progress, and should differentiate “healing reactions” from genuine adverse drug or supplement effects (electrolyte disturbance, thyroid overshoot, infection) which can present similarly.
What Modern Hepatology Actually Says
Modern hepatology accepts the broad framework of Phase I, Phase II, and Phase III hepatic detoxification, accepts that nutrition modifies the activity of all three phases, and accepts that some plant phytochemicals (sulforaphane from broccoli, curcumin, milk thistle silymarin, and yes, coffee diterpenes) induce protective Phase II enzymes. It does not accept the broader framework that the body accumulates a generalized burden of “toxins” that requires periodic external removal in healthy people.
Mainstream medicine rejects the concept of “cleanses” for healthy people because there is no demonstrated accumulation to clean and no outcome data showing that cleansing improves health in unselected populations. The honest summary on this point is that the broad Gerson detoxification framing contains some real biochemistry embedded in a larger conceptual structure that is not supported by current evidence.
Oral Coffee versus Rectal Coffee
For most of the proposed benefits of coffee — hepatoprotection, GST induction, reduced risk of hepatocellular carcinoma, reduced acute kidney injury risk, improved insulin sensitivity, reduced Parkinson’s risk — the evidence base is overwhelmingly oral. Three to four cups of brewed coffee a day is associated in large prospective cohort studies (UK Biobank, EPIC, NIH-AARP) with reduced all-cause mortality, reduced cardiovascular mortality, and reduced incidence of several cancers and chronic liver diseases.
None of this evidence applies to rectal administration. The proposed unique benefits of the enema route — portal-vein delivery, sphincter of Oddi relaxation in concentrated form, GST induction at higher hepatic exposure — remain mechanistically plausible at best and have not been confirmed in human outcome studies.
For the vast majority of people interested in coffee’s health benefits, drinking the coffee delivers most of the documented benefits without any of the documented risks of rectal administration. See the Coffee hub for the oral-coffee evidence base.
Beyond Coffee: Phase I, II, III Detoxification
The Gerson Therapy supports hepatic detoxification through more channels than the coffee enema alone. The diet provides large doses of cruciferous vegetables (sulforaphane and indole-3-carbinol, which induce Phase II), allium vegetables (organosulfurs), polyphenol-rich fruits (which support glutathione recycling), and the high potassium and magnesium content needed for Phase III biliary excretion. The flax oil contributes alpha-linolenic acid for membrane fluidity and bile composition. The reduction in dietary fat lowers the load on biliary clearance. The avoidance of alcohol, processed food, and tobacco removes major Phase I oxidative stressors.
If the protocol works at all in non-cancer indications, it is plausible that the dietary components carry most of the load and that the coffee enema is the most controversial and least essential element. For patients drawn to the broader detoxification framework but uncomfortable with daily enemas, the modified Gerson diet alone — without enemas — captures most of the documented hepatoprotective benefit while eliminating the documented harms.
Key Research and Sources
- Lam LK et al. (1982). “Isolation and identification of kahweol palmitate and cafestol palmitate as active constituents of green coffee beans that enhance glutathione S-transferase activity in the mouse.” Cancer Research. PMID: 7104999
- Cavin C et al. (2002). “Cafestol and kahweol, two coffee specific diterpenes with anticarcinogenic activity.” Food and Chemical Toxicology. PMID: 12067578
- Urgert R, Katan MB (1997). “The cholesterol-raising factor from coffee beans.” Annual Review of Nutrition. — the cardiovascular side of cafestol and kahweol.
- Hodgman MJ et al. (1998). “Caffeine’s effect on the rectal mucosa.” — rectal absorption pharmacokinetics.
- Gerson Institute. “The detoxifying enema.” gerson.org
- Loftfield E et al. (2018). “Association of coffee drinking with mortality by genetic variation in caffeine metabolism.” JAMA Internal Medicine. PMID: 29971434
- PubMed search: “glutathione S-transferase coffee”
- PubMed search: “Phase II detoxification phytochemicals”