Hives and Flushing
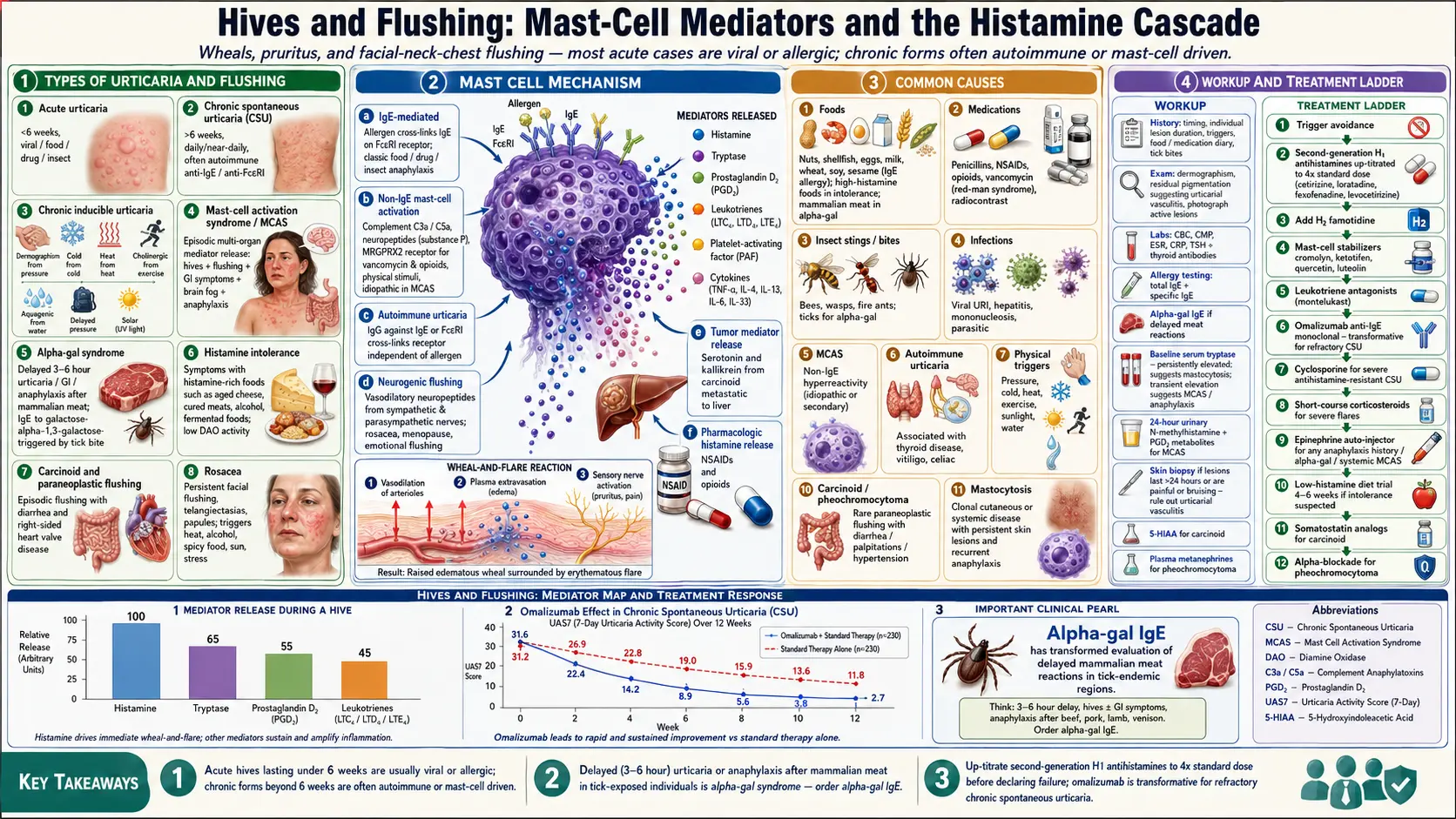

Table of Contents
- Overview
- Types of Hives and Flushing
- Common Causes
- Mechanisms
- Evaluation
- Management
- When to Seek Medical Care
- Connections
- References & Research
- Featured Videos
Overview
Hives (urticaria) are raised, itchy, blanching wheals that come and go, typically resolving within 24 hours at any given site. Flushing is transient redness and warmth, usually of the face, neck, and upper chest. Both arise from the release of histamine and other vasoactive mediators from skin mast cells. They share triggers and pathways, and frequently co-occur. Most acute cases are self-limited and viral or allergic; chronic forms (lasting more than six weeks) are more often autoimmune, mast-cell-mediated, or driven by physical triggers, and require systematic evaluation.
Types of Hives and Flushing
- Acute urticaria — less than six weeks; usually viral, food, drug, or insect-sting triggered.
- Chronic spontaneous urticaria (CSU) — daily or near-daily hives for more than six weeks without an identifiable trigger; many cases are autoimmune (anti-IgE or anti-FcεRI antibodies).
- Chronic inducible urticaria — reproducibly triggered by physical stimuli: dermographism (pressure), cold, heat, exercise (cholinergic), water (aquagenic), pressure-delayed, or solar.
- Mast cell activation syndrome (MCAS) — episodic mediator release across multiple organ systems, with flushing, hives, GI symptoms, brain fog, and sometimes anaphylaxis.
- Alpha-gal syndrome — delayed (3–6 hour) urticaria, GI symptoms, or anaphylaxis after eating mammalian meat or gelatin, triggered by tick-bite-induced IgE to galactose-alpha-1,3-galactose.
- Histamine intolerance — symptoms with histamine-rich or histamine-releasing foods (aged cheese, cured meats, alcohol, fermented foods); often from low diamine oxidase (DAO) activity.
- Carcinoid and other paraneoplastic flushing — episodic flushing with diarrhea and right-sided heart valve disease; rare but important.
- Rosacea-related flushing — persistent or episodic facial flushing, often triggered by heat, alcohol, spicy food, sun, or stress.
Common Causes
- Foods — nuts, shellfish, eggs, milk, wheat, soy, sesame in classic IgE allergy; high-histamine foods in histamine intolerance; mammalian meat in alpha-gal syndrome.
- Medications — penicillins, NSAIDs, opioids, vancomycin (red-man syndrome), radiocontrast.
- Insect stings and bites — bees, wasps, fire ants; tick bites can trigger alpha-gal sensitization.
- Infections — viral upper respiratory infections, hepatitis, mononucleosis, parasitic infections.
- MCAS — non-IgE mast-cell hyperreactivity to a wide variety of triggers (foods, exercise, heat, stress, hormones).
- Autoimmune urticaria — IgG against IgE or its receptor; associated with autoimmune thyroid disease, vitiligo, celiac disease.
- Physical triggers — pressure, cold, heat, sun, water, exercise.
- Environmental allergens — pollen, dust mite, animal dander.
- Hormonal — perimenstrual flares, menopause flushing, pregnancy.
- Carcinoid tumor and pheochromocytoma — rare but consider with sustained or paroxysmal flushing, diarrhea, palpitations, or hypertension.
- Mastocytosis — clonal mast-cell disease (cutaneous or systemic) with persistent skin lesions and recurrent anaphylaxis.
Mechanisms
- Mast-cell degranulation — histamine, tryptase, prostaglandin D2, leukotrienes, platelet-activating factor and cytokines released from skin and gut mast cells produce vasodilation, plasma extravasation (wheal), pruritus, and smooth-muscle effects.
- IgE-mediated — allergen cross-links IgE on mast cells via the high-affinity FcεRI receptor; classic in food, drug, and insect-sting anaphylaxis.
- Non-IgE mast-cell activation — complement (C3a, C5a), neuropeptides (substance P), MRGPRX2 receptor signaling (vancomycin, opioids), physical stimuli, and idiopathic triggers in MCAS.
- Autoimmune urticaria — circulating IgG autoantibodies against IgE or FcεRI cross-link the receptor independent of allergen.
- Neurogenic flushing — vasodilatory neuropeptides released from sympathetic and parasympathetic nerves; rosacea, menopause, and emotional flushing.
- Tumor mediator release — serotonin, kallikrein, and other mediators from carcinoid tumors metastatic to liver.
Evaluation
- History — timing, duration of individual lesions, triggers, food and medication diary, recent infections, tick bites, geographic exposures.
- Physical exam — check for dermographism, look for residual pigmentation (suggests urticarial vasculitis), photograph or document active lesions when present.
- CBC, CMP, ESR, CRP, TSH and thyroid antibodies — baseline workup in chronic urticaria.
- Total IgE and specific IgE — if specific food or environmental trigger suspected.
- Alpha-gal IgE — in any patient with delayed reactions to mammalian meat, particularly with tick exposure.
- Baseline serum tryptase — persistently elevated levels suggest mastocytosis; transient elevations during reactions support MCAS or anaphylaxis.
- 24-hour urinary N-methylhistamine, prostaglandin D2 metabolites — if MCAS suspected.
- Skin biopsy — if lesions last more than 24 hours, are painful, leave bruising, or are atypical (rule out urticarial vasculitis).
- 5-HIAA in 24-hour urine — if carcinoid suspected (sustained flushing with diarrhea).
- Plasma metanephrines — if pheochromocytoma suspected (paroxysmal flushing, hypertension, palpitations).
Management
- Trigger avoidance — food, medication, insect, alcohol, heat, exercise as identified.
- Second-generation H1 antihistamines — cetirizine, loratadine, fexofenadine, levocetirizine; uptitrate to four times the standard dose in chronic urticaria before declaring failure.
- Add H2 antihistamines — famotidine; helps in some patients, particularly with GI symptoms.
- Mast-cell stabilizers — cromolyn sodium (oral for GI symptoms), ketotifen, quercetin, luteolin; particularly useful in MCAS.
- Leukotriene receptor antagonists — montelukast as adjunct in chronic urticaria, particularly aspirin-exacerbated.
- Omalizumab — anti-IgE monoclonal antibody; transformative for refractory chronic spontaneous urticaria.
- Cyclosporine — for severe, antihistamine-resistant chronic urticaria.
- Short courses of corticosteroids — for severe acute flares; avoid chronic use.
- Epinephrine auto-injector — prescribed for any patient with prior anaphylaxis, alpha-gal syndrome, or systemic MCAS.
- Low-histamine diet trial — if histamine intolerance suspected; reassess after 4–6 weeks.
- Treat the underlying disease — thyroid replacement in autoimmune thyroiditis, somatostatin analogs for carcinoid, alpha-blockade for pheochromocytoma.
When to Seek Medical Care
- Difficulty breathing, throat tightness, hoarseness, or tongue swelling — suspect anaphylaxis, use epinephrine, call 911.
- Fainting, drop in blood pressure, or rapid pulse with hives.
- Hives with high fever, joint pain, or weight loss (consider urticarial vasculitis or systemic disease).
- Individual lesions lasting more than 24 hours, painful, or leaving bruises.
- Hives in a pregnant woman with abdominal pain, jaundice, or pruritus without rash (rule out cholestasis of pregnancy).
- Sustained flushing with diarrhea, weight loss, or wheezing (rule out carcinoid).
- Paroxysmal flushing with hypertension, palpitations, headache (rule out pheochromocytoma).
Connections
- MCAS
- Alpha-Gal Syndrome
- Allergies
- Brain Fog
- Rosacea
- Eczema
- Hashimoto's Thyroiditis
- Bloating
- POTS
- Food Intolerance
- POTS/MCAS/EDS Triad
- Alpha-Gal Natural History
- Asthma
- Pheochromocytoma
- Celiac Disease
- Anaphylaxis Emergency Plan
References & Research
Historical Background
Urticaria has been recognized since Hippocrates as "knidosis," from the Greek for nettle. The discovery of histamine in 1910 and IgE in 1966 established the basic mechanism. Chronic spontaneous urticaria as an autoimmune disease was characterized in the 1990s. Mast cell activation syndrome was formalized as a distinct clinical entity in 2010, and alpha-gal syndrome was identified after lone-star-tick exposures in the U.S. Southeast in 2009.
Key Research Papers
- Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA2LEN/EDF/WAO guideline for the definition, classification, diagnosis and management of urticaria. Allergy. 2018;73(7):1393-1414.
- Maurer M, Rosen K, Hsieh HJ, et al. Omalizumab for the treatment of chronic idiopathic or spontaneous urticaria. New England Journal of Medicine. 2013;368(10):924-935.
- Akin C, Valent P, Metcalfe DD. Mast cell activation syndrome: proposed diagnostic criteria. Journal of Allergy and Clinical Immunology. 2010;126(6):1099-1104.
- Commins SP, Satinover SM, Hosen J, et al. Delayed anaphylaxis, angioedema, or urticaria after consumption of red meat in patients with IgE antibodies specific for galactose-α-1,3-galactose. Journal of Allergy and Clinical Immunology. 2009;123(2):426-433.
- Valent P, Akin C, Bonadonna P, et al. Proposed diagnostic algorithm for patients with suspected mast cell activation syndrome. Journal of Allergy and Clinical Immunology: In Practice. 2019;7(4):1125-1133.
- Saini SS, Kaplan AP. Chronic spontaneous urticaria: the devil's itch. Journal of Allergy and Clinical Immunology: In Practice. 2018;6(4):1097-1106.
- Khan DA. Chronic urticaria: diagnosis and management. Allergy and Asthma Proceedings. 2008;29(5):439-446.
- Wilson JM, Schuyler AJ, Workman L, et al. The IgE response to alpha-gal: clinical relevance and pathophysiology. Annals of Allergy, Asthma & Immunology. 2018;120(2):137-143.
- Maintz L, Novak N. Histamine and histamine intolerance. American Journal of Clinical Nutrition. 2007;85(5):1185-1196.
- Izikson L, English JC III, Zirwas MJ. The flushing patient: differential diagnosis, workup, and treatment. Journal of the American Academy of Dermatology. 2006;55(2):193-208.
PubMed Topic Searches
- Chronic spontaneous urticaria
- Mast cell activation syndrome diagnosis
- Alpha-gal syndrome and meat allergy
- Histamine intolerance and DAO deficiency
- Omalizumab for chronic urticaria
- Carcinoid syndrome flushing