Chanca Piedra Safety, Drug Interactions, and Cautions
Chanca Piedra is generally well-tolerated, with a strong traditional safety record and a low acute toxicity in animal studies (LD50 > 5,000 mg/kg). The clinically meaningful safety issues are not toxicity but drug interactions — particularly through cytochrome P450 inhibition (especially CYP3A4) and P-glycoprotein effects — and a few hard contraindications (pregnancy, pre-surgical, certain comorbidities). This page is the practical safety reference.
Table of Contents
- General Safety Profile
- Common Side Effects
- Hard Contraindications
- CYP450 Drug Interactions
- P-Glycoprotein Interactions
- Diabetes Medications
- Antihypertensives
- Anticoagulants and Antiplatelets
- Lithium
- Pregnancy and Breastfeeding
- Pre-Surgical Discontinuation
- Research Papers and References
- Connections
- Featured Videos
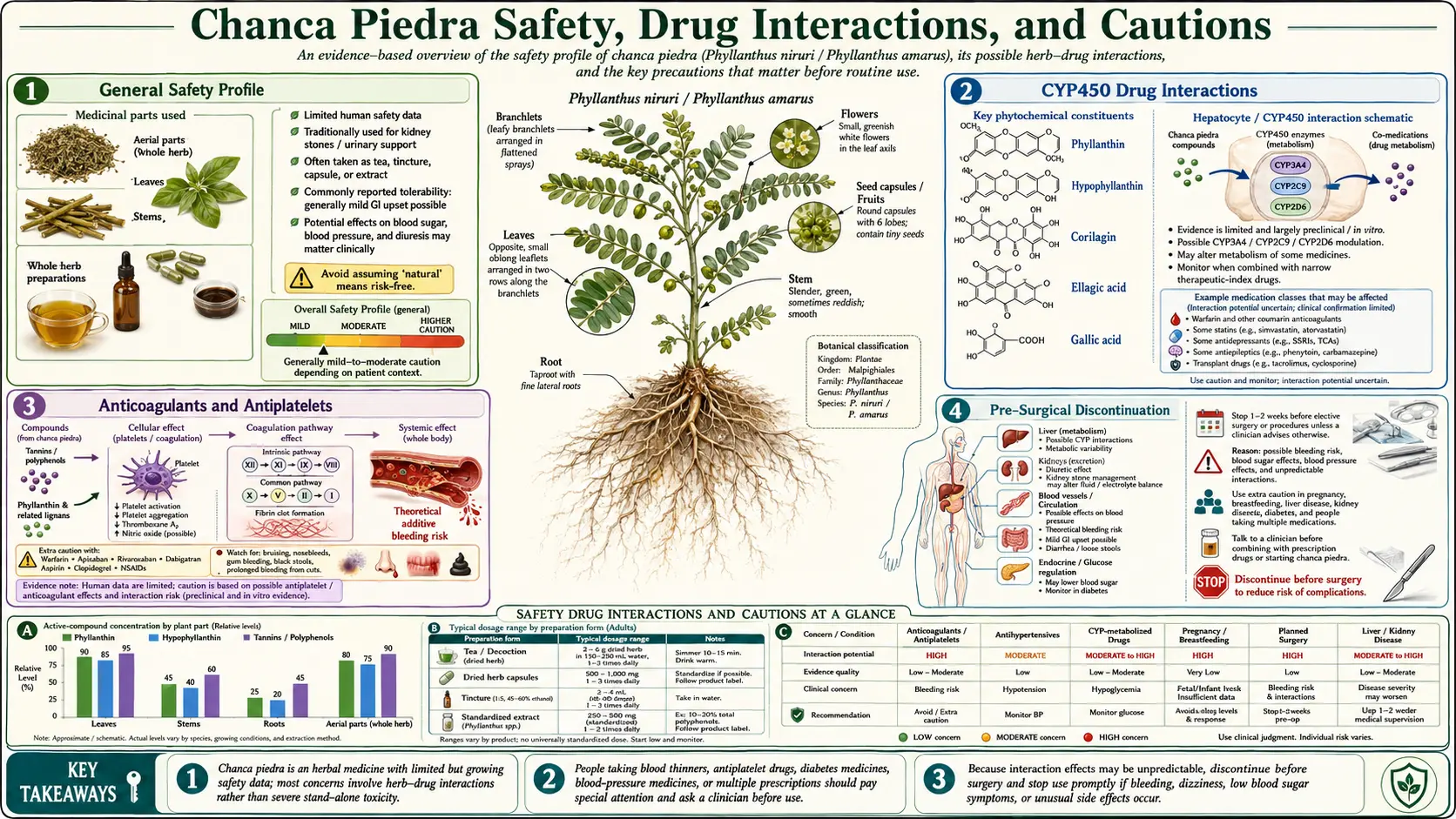
General Safety Profile
Chanca Piedra has been used traditionally for centuries with no documented pattern of serious adverse effects. Modern clinical trials (ranging from 30 days to 12 months) have reported tolerability comparable to placebo in most studies. Acute toxicity in animal models is very low: LD50 > 5,000 mg/kg in rodent studies, well above any clinical dose.
The safety concerns that do exist relate not to direct toxicity but to drug interactions and certain physiologic effects (uterine stimulation, mild hypotension, mild hypoglycemic effect) that warrant caution in specific populations.
Common Side Effects
Reported in clinical trials and postmarketing surveillance, generally mild and infrequent:
- Stomach upset, mild GI discomfort
- Mild diarrhea, especially at higher doses
- Headache
- Occasional dizziness or postural hypotension (related to mild diuretic and ACE-like effects)
- Mild fatigue (rare)
- Allergic reactions (rare)
Side effects are typically dose-dependent and resolve with dose reduction or discontinuation.
Hard Contraindications
- Pregnancy — uterine-stimulating activity in animal studies; avoid entirely
- Breastfeeding — insufficient safety data
- Children under 18 — no pediatric dosing established
- Pre-surgical (stop 2 weeks before) — may affect bleeding (mild antiplatelet activity) and blood sugar
- Active hypotension or volume depletion — may worsen low blood pressure
- Severe hepatic or renal impairment — not because the herb is harmful, but because metabolism and clearance change unpredictably; consult clinician
CYP450 Drug Interactions
Chanca Piedra inhibits multiple cytochrome P450 enzymes, with CYP3A4 inhibition being mechanism-based (irreversible enzyme suicide). This is the most clinically significant interaction pathway, because CYP3A4 metabolizes about 50% of clinically prescribed drugs.
CYP3A4 substrates — caution required:
- Statins (atorvastatin, simvastatin most affected; pravastatin and rosuvastatin less affected)
- Calcineurin inhibitors (tacrolimus, cyclosporine) — narrow therapeutic window; do not combine without specialist guidance
- HIV protease inhibitors (ritonavir, atazanavir, darunavir)
- Tamoxifen (activation pathway affected)
- Many calcium-channel blockers (amlodipine, diltiazem, verapamil)
- Certain anticonvulsants (carbamazepine)
- Some chemotherapy agents (docetaxel, paclitaxel, vincristine)
- Oral contraceptives (theoretical efficacy reduction or alteration)
- Some benzodiazepines (alprazolam, midazolam)
CYP2C9 substrates:
- Warfarin — can raise INR; monitor weekly during initiation
- Phenytoin
- NSAIDs (ibuprofen, celecoxib)
- Some sulfonylureas
Other CYPs (lesser inhibition): CYP1A2, CYP2D6, CYP2E1 — relevant for caffeine clearance, certain antidepressants, acetaminophen toxicity threshold respectively.
P-Glycoprotein Interactions
Phyllanthin and hypophyllanthin are direct P-glycoprotein inhibitors in Caco-2 cells. P-gp inhibition raises plasma levels of P-gp-substrate drugs, potentially increasing both efficacy and toxicity:
- Digoxin (narrow therapeutic window; monitor levels)
- Certain calcium-channel blockers
- Some HIV antiretrovirals
- Certain chemotherapy agents
- Dabigatran (direct oral anticoagulant)
The MRP2 efflux transporter is unaffected, so methotrexate and certain chemotherapy regimens that depend on MRP2 are not affected.
Diabetes Medications
- Insulin and sulfonylureas (glyburide, glipizide, glimepiride) — theoretical additive hypoglycemia; monitor glucose more frequently in the first 2–4 weeks of combination
- Metformin — no documented additive hypoglycemia; mechanistically compatible
- GLP-1 agonists, SGLT2 inhibitors, DPP-4 inhibitors — no documented interactions; theoretical additive effect minor
Antihypertensives
Additive blood-pressure-lowering with most antihypertensive classes:
- ACE inhibitors (lisinopril, enalapril) — mild additive effect
- ARBs (losartan, valsartan) — mild additive effect
- Thiazide diuretics — mild additive diuresis
- Calcium-channel blockers — mild additive plus CYP3A4 effect on amlodipine and others
- Beta-blockers — minimal interaction
Realistic risk: mild hypotension or dizziness, not crisis. Monitor blood pressure for the first 2–4 weeks of combination. Avoid stacking with potassium-sparing diuretics (spironolactone, eplerenone) in CKD — theoretical hyperkalemia risk via the ACE-like mechanism.
Anticoagulants and Antiplatelets
- Warfarin — CYP2C9 inhibition can raise INR. Check INR weekly for the first 3 weeks of any new combination.
- Direct oral anticoagulants (DOACs): apixaban, rivaroxaban, edoxaban — metabolized through CYP3A4 (rivaroxaban, apixaban) and P-gp (all). Theoretical risk of elevated drug levels and bleeding.
- Dabigatran — P-gp substrate; theoretical risk of elevated levels.
- Aspirin and clopidogrel — mild theoretical additive antiplatelet effect; clinically minor in most patients.
- Heparin / LMWH — no documented interaction.
Lithium
Mild diuretic effect of Chanca Piedra could increase lithium reabsorption (similar mechanism to thiazides), raising serum lithium levels and risk of toxicity. Monitor lithium serum levels every 2–4 weeks during initiation if combination is unavoidable; consider dose reduction.
Pregnancy and Breastfeeding
Avoid in both. Animal studies have shown uterine stimulation and possible fetal effects. There are no human pregnancy studies of adequate size to assess safety. Breastfeeding data are insufficient. The mild diuretic and hypotensive effects could also affect maternal hemodynamics and milk production.
Pre-Surgical Discontinuation
Stop Chanca Piedra at least 2 weeks before any planned surgery. Reasons:
- Mild antiplatelet activity could affect surgical bleeding
- Mild hypoglycemic effect could complicate perioperative glucose management
- CYP3A4 inhibition could affect anesthesia drug metabolism (especially benzodiazepines, certain anesthetics)
- Mild diuretic effect could complicate fluid management
This is consistent with general herbal-supplement guidelines: most botanicals with active pharmacology should be discontinued 2 weeks before elective surgery.
Research Papers and References
- Acute toxicity studies — PubMed
- CYP450 inhibition — PubMed
- P-gp interactions — PubMed
- Pregnancy concerns — PubMed
- Long-term human safety — PubMed
- Herbal-drug interactions — PubMed
Connections
- Chanca Piedra Overview
- Kidney Stone Protocol
- Liver Protection and Hepatitis B
- Blood Sugar and Metabolic Effects
- Uric Acid, Gout and Hypertension
- Active Compounds
- Forms, Dosing and Standardization
- Phyllanthus Species Comparison
- History and Traditional Use
- Potassium
- Calcium
- Diabetes
- Blood Sugar
- Comprehensive Metabolic Panel
- GLP-1 Receptor Agonists