CAC in Women and Younger Adults: Sex Differences and the Premenopause Window
Cardiovascular disease in women has historically been understudied, underdiagnosed, and undertreated. The CAC score is one of the few preventive cardiology tools that performs particularly well in women, but interpreting it requires recognizing that women's coronary calcium accumulates roughly a decade later than men's, that the menopausal transition is the inflection point in women's cardiovascular risk, and that the meaning of any given absolute score shifts substantially with sex. This page covers how to think about CAC in women, when it's reasonable to scan in younger adults, and the special situations that warrant earlier-than-default testing.
Table of Contents
- The 10-Year Sex Offset
- Why Women's CV Disease Differs
- Perimenopause as the Turning Point
- Premature Menopause and CV Risk
- CAC in Women in Their 50s
- CAC Under 40
- Familial Hypercholesterolemia in Young Adults
- Markedly Elevated Lp(a)
- Pregnancy History as Risk Modifier
- Research Papers and References
- Connections
- Featured Videos
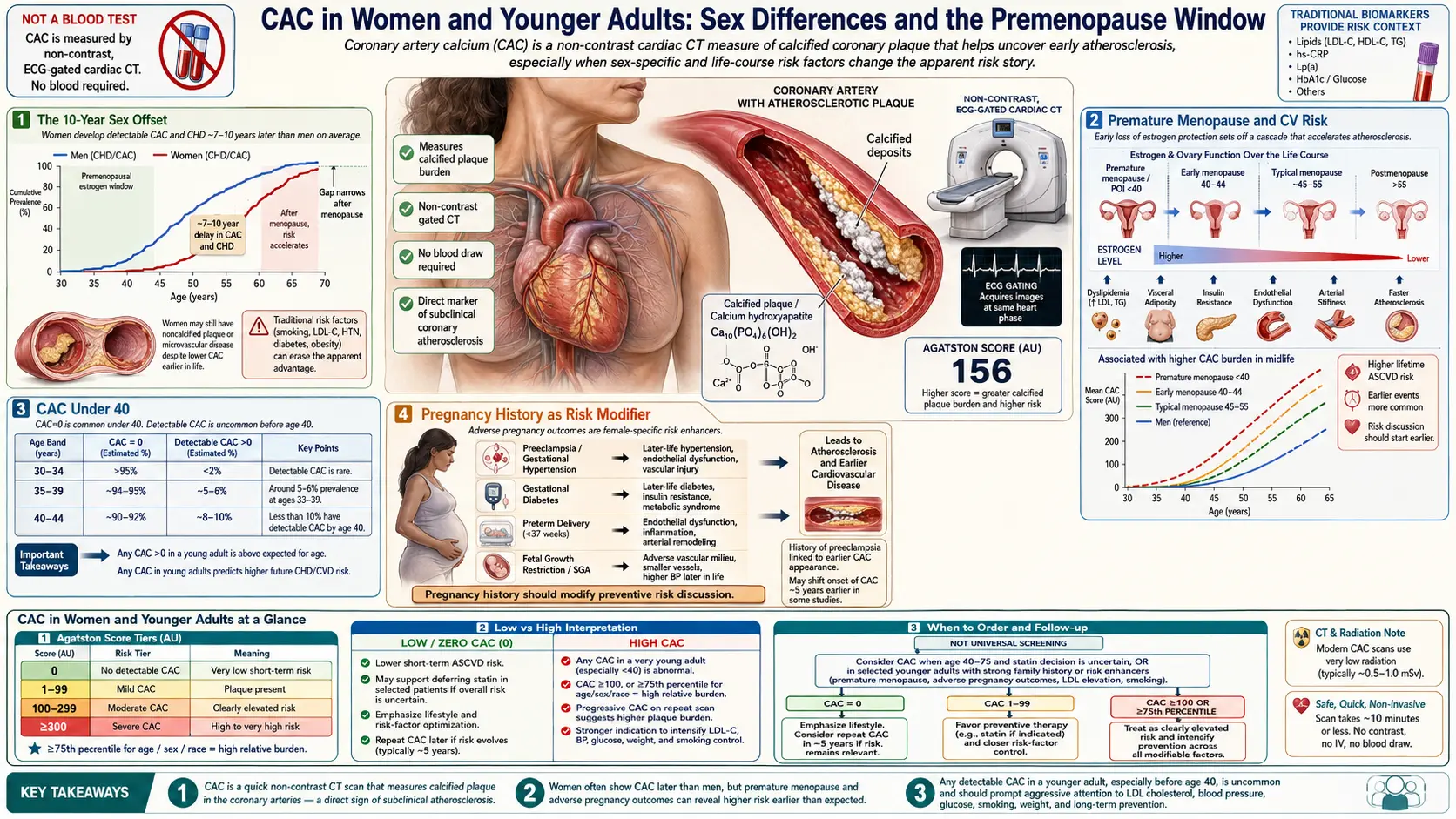
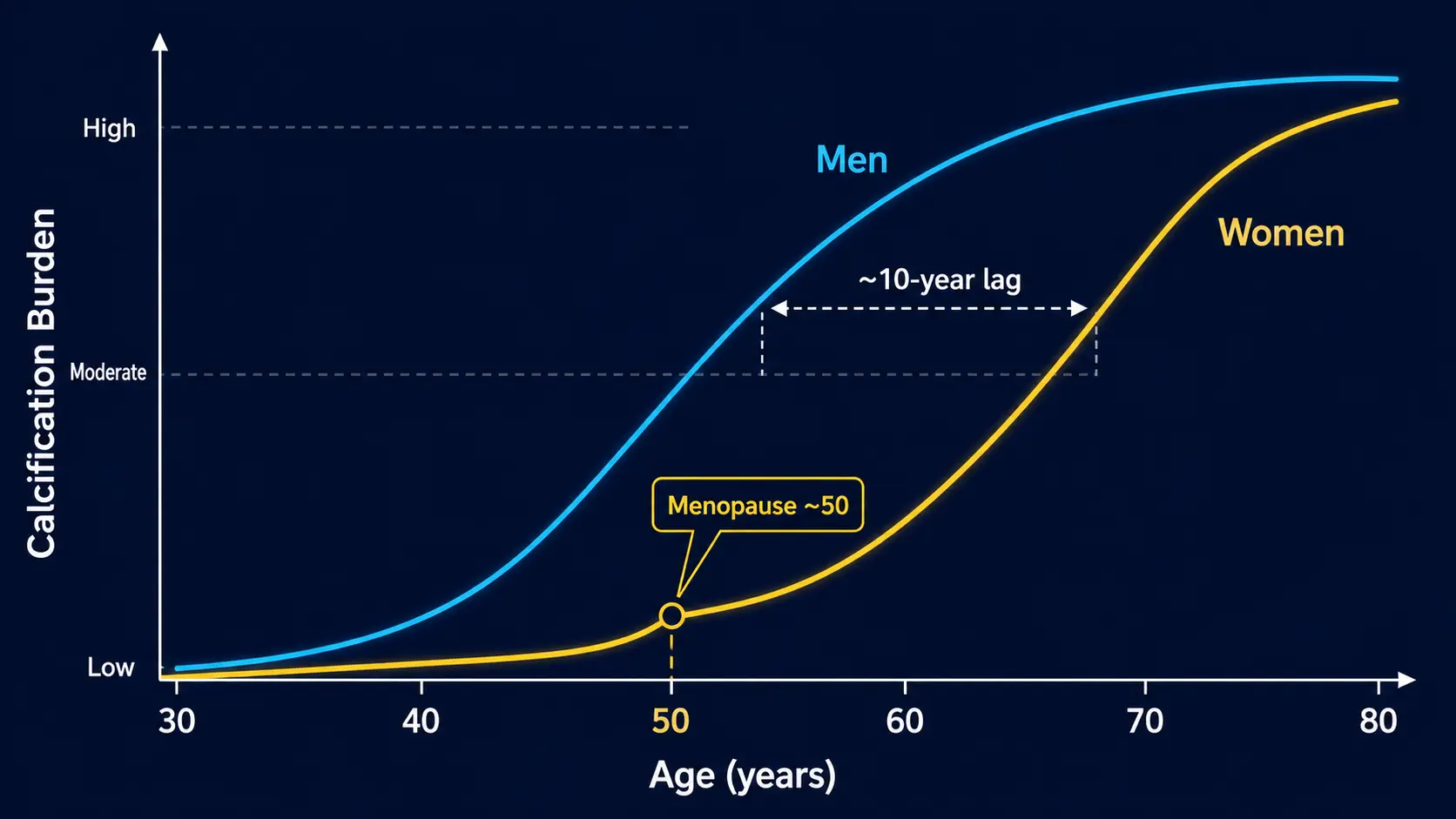
The 10-Year Sex Offset
Women on average develop calcified coronary plaque about 10 years later than men. The MESA cohort and other large datasets show:
- Median CAC at age 50: 0 in women, ~5 in men
- Median CAC at age 60: ~5 in women, ~30 in men
- Median CAC at age 70: ~50 in women, ~150 in men
- 90th-percentile CAC at 50: ~25 in women, ~100 in men
- 90th-percentile CAC at 60: ~120 in women, ~400 in men
The clinical implication: a CAC score that would be reassuring in a 55-year-old man might be alarming in a 55-year-old woman. The same MESA percentile calculator handles this automatically by sex-adjusting the reference distribution — always check the percentile, not just the absolute number.
Why Women's CV Disease Differs
Women's cardiovascular disease has several distinguishing features that affect both the timing and the interpretation of CAC:
- Estrogen protection — until menopause, endogenous estrogen has lipid-favorable, vascular-protective, and anti-inflammatory effects that delay atherosclerosis
- Microvascular and small-vessel disease — more common in women; not detected by CAC
- Spontaneous coronary artery dissection (SCAD) — 90% of cases occur in women, often peripartum or perimenopausal; CAC does not predict SCAD
- Coronary vasospasm — more common in women; not detected by CAC
- Atypical symptom presentation — women more likely to present with fatigue, dyspnea, jaw pain, nausea rather than classic chest pressure
- Underdiagnosis and undertreatment — persistent treatment gaps, particularly in younger women presenting with chest pain
The result: CAC alone is a less complete picture in women than in men. It is still highly useful for risk stratification but should be interpreted alongside symptoms, lipid markers, and reproductive history.
Perimenopause as the Turning Point
The perimenopausal transition (typically ages 45–55) is the inflection point where women's cardiovascular risk begins to converge with men's. Within 5–10 years post-menopause, the protective lipid and vascular profile of premenopause is largely gone:
- LDL-C rises 10–15% on average
- HDL-C falls slightly
- Triglycerides rise
- Visceral adiposity increases
- Insulin sensitivity decreases
- Blood pressure rises
For most women, the late 40s to mid-50s is the right window for first-time CAC scoring, especially if any traditional risk factors are present (family history, hypertension, dyslipidemia, prediabetes). A baseline CAC at age 50 in a woman gives a personalized number to anchor the next two decades of cardiovascular care.
Premature Menopause and CV Risk
Premature menopause (before age 40) and early menopause (40–45) are independent risk factors for accelerated cardiovascular disease. The mechanism is loss of estrogen exposure decades earlier than the population average. Major drivers of premature menopause include:
- Surgical menopause (oophorectomy, often with hysterectomy for benign disease)
- Chemotherapy-induced ovarian failure
- Radiation therapy to the pelvis
- Autoimmune ovarian failure
- Genetic causes (Turner syndrome, fragile X premutation)
- Idiopathic
Women with premature or early menopause should be considered for earlier CAC scoring (at age 40–45 rather than 50–55), aggressive lipid management, and consideration of hormone replacement therapy in appropriate cases (the timing-of-initiation hypothesis suggests HRT started within 10 years of menopause may have cardiovascular benefit).
CAC in Women in Their 50s
For women in their 50s, the case for CAC testing is increasingly strong:
- The post-menopausal transition has begun or is underway
- Lipid profile is shifting unfavorably
- The 10-year ASCVD risk calculator can underestimate true risk in this age band
- A CAC score gives concrete data to drive statin/lifestyle decisions
- The decision to start HRT is sometimes informed by knowledge of underlying CV burden (high CAC may shift toward non-hormonal alternatives)
A reasonable schedule for an asymptomatic woman with no major risk factors:
- Lipid panel + ApoB + Lp(a) at age 40, repeat lipids every 3–5 years
- First CAC at age 50 (or earlier with risk factors)
- Re-scan at 5–7 year intervals if first CAC = 0
- Manage based on integrated picture
CAC Under 40
CAC scoring under age 40 is not routine because most healthy young adults have a score of zero. Specific situations where it becomes useful:
- Family history of premature CAD (male first-degree relative under 55, female under 65)
- Familial hypercholesterolemia, confirmed or suspected
- Markedly elevated Lp(a) (> 100 nmol/L or > 50 mg/dL)
- Long-standing or poorly-controlled type 1 diabetes
- Symptoms suggestive of cardiac etiology (atypical chest pain in young athletes)
- HIV with prolonged antiretroviral exposure
- Cocaine or methamphetamine use history
- Long-term high-dose corticosteroid or immunosuppressant exposure
Note: a CAC = 0 at age 35 is reassuring but not the same as exclusion of soft-plaque disease. In high-risk young adults, complementary CCTA evaluation may be warranted; see the Soft Plaque page.
Familial Hypercholesterolemia in Young Adults
Familial hypercholesterolemia (FH) affects approximately 1 in 250 people. Heterozygous FH typically presents with LDL-C above 190 mg/dL (untreated), tendon xanthomas, and family history of premature MI. CAC in FH:
- Many heterozygous FH patients have detectable calcified plaque by their 30s or 40s
- CAC progression is faster in FH than non-FH controls
- A CAC = 0 in young FH patients does not exclude soft plaque; CCTA may be appropriate
- Treatment is mandatory regardless of imaging findings (high-intensity statin at minimum)
- PCSK9 inhibitors and lomitapide are options when statin + ezetimibe insufficient
FH is a key population where early lipid management trumps imaging-driven decisions. CAC adds risk stratification but does not change the fundamental need for therapy.
Markedly Elevated Lp(a)
Lipoprotein(a) is a genetically determined LDL-like particle whose level is essentially fixed for life. Approximately 20% of the population has elevated Lp(a) (> 50 mg/dL or > 100 nmol/L). Lp(a) is independent of LDL-C and is associated with:
- Premature coronary atherosclerosis
- Calcific aortic stenosis
- Increased thrombotic risk
- Higher event rates at any given LDL-C
For young adults with markedly elevated Lp(a), CAC scoring earlier than the standard age-50 threshold is reasonable, with an understanding that CAC = 0 doesn't exclude soft-plaque burden. Management focus is on getting LDL-C/ApoB very low (because the additive effect of Lp(a) compounds at higher LDL levels) plus aggressive lifestyle. Lp(a)-targeted RNA therapies are in late-phase trials and may reach market in 2026–2028.
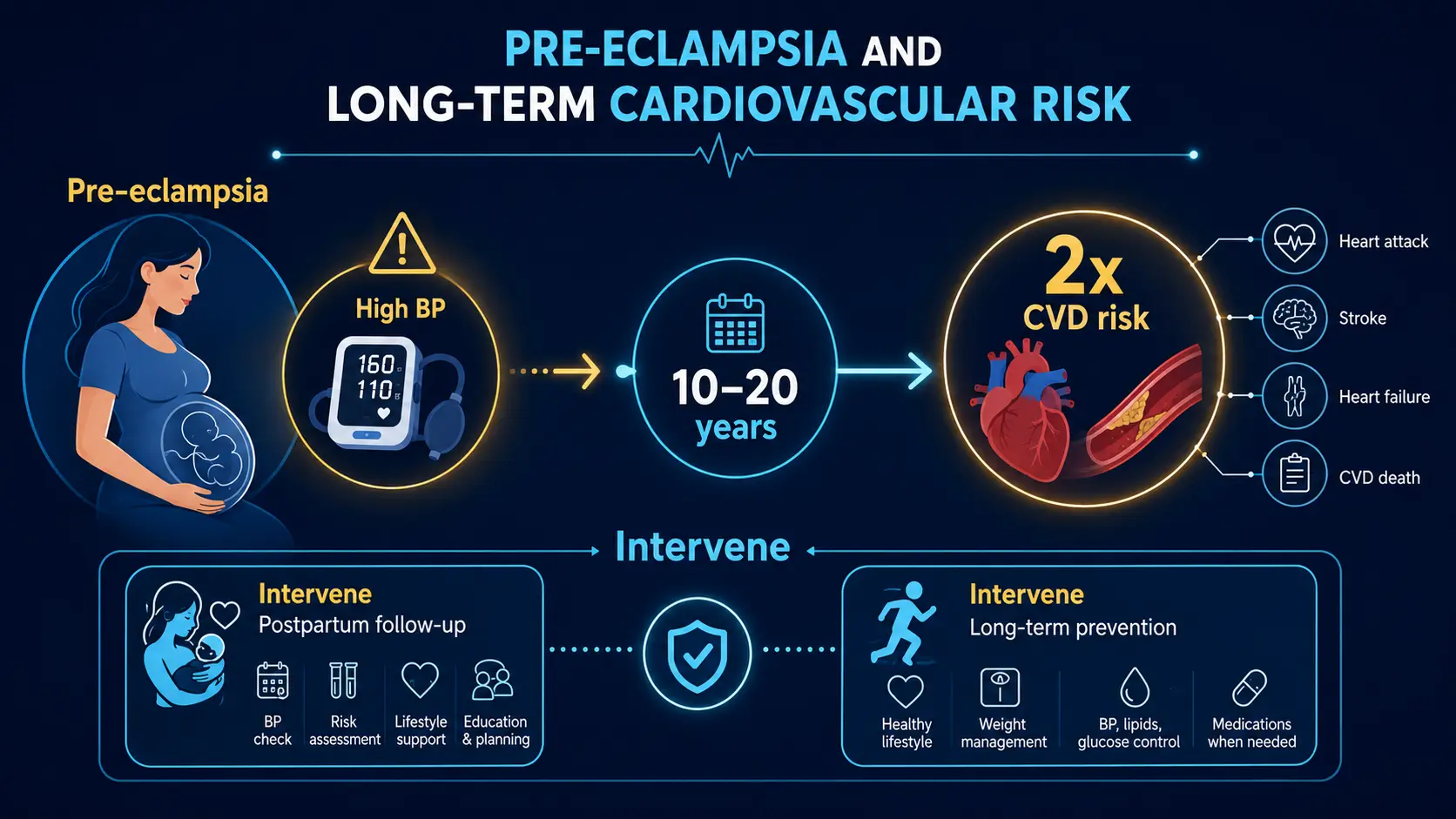
Pregnancy History as Risk Modifier
Several pregnancy complications are independent risk factors for future cardiovascular disease and should inform CAC timing:
- Preeclampsia / eclampsia — doubles long-term CV risk; consider earlier CAC in 40s
- Gestational diabetes — markedly increased lifetime risk of T2DM and CV events
- Gestational hypertension — predicts chronic hypertension and elevated CV risk
- Preterm birth — associated with increased maternal CV risk
- HELLP syndrome — severe variant; markedly elevated future CV risk
- Recurrent miscarriage — some association with vascular dysfunction (especially in antiphospholipid syndrome)
Women with these histories should mention them to their primary care physician or cardiologist; they may justify earlier CAC scoring (40s rather than 50s) and more aggressive risk-factor management.
Research Papers and References
- Sex differences in CAC — PubMed search
- Premature menopause and CV risk — PubMed search
- Preeclampsia and long-term CV risk — PubMed search
- SCAD in women — PubMed search
- Lp(a) in young adults — PubMed search
- FH and CAC progression — PubMed search
- HRT timing and CV outcomes — PubMed search
Connections
- Coronary Calcium Score
- Soft Plaque and CAC Limitations
- MESA Risk Calculator and Age Percentiles
- Agatston Score Calculation and Interpretation
- CAC Zero and the Power of Negative Result
- Statin Threshold and CAC
- ApoB
- Lipoprotein(a)
- Lipid Panel
- Cardiovascular Disease
- Atherosclerosis
- Hypertension
- Perimenopause
- Preeclampsia
- Calcium
- CAC vs Other Cardiac Tests
- Can You Reverse Coronary Calcium? Plaque Stabili
- Insurance Cost and Access