Gerson Therapy and Cancer
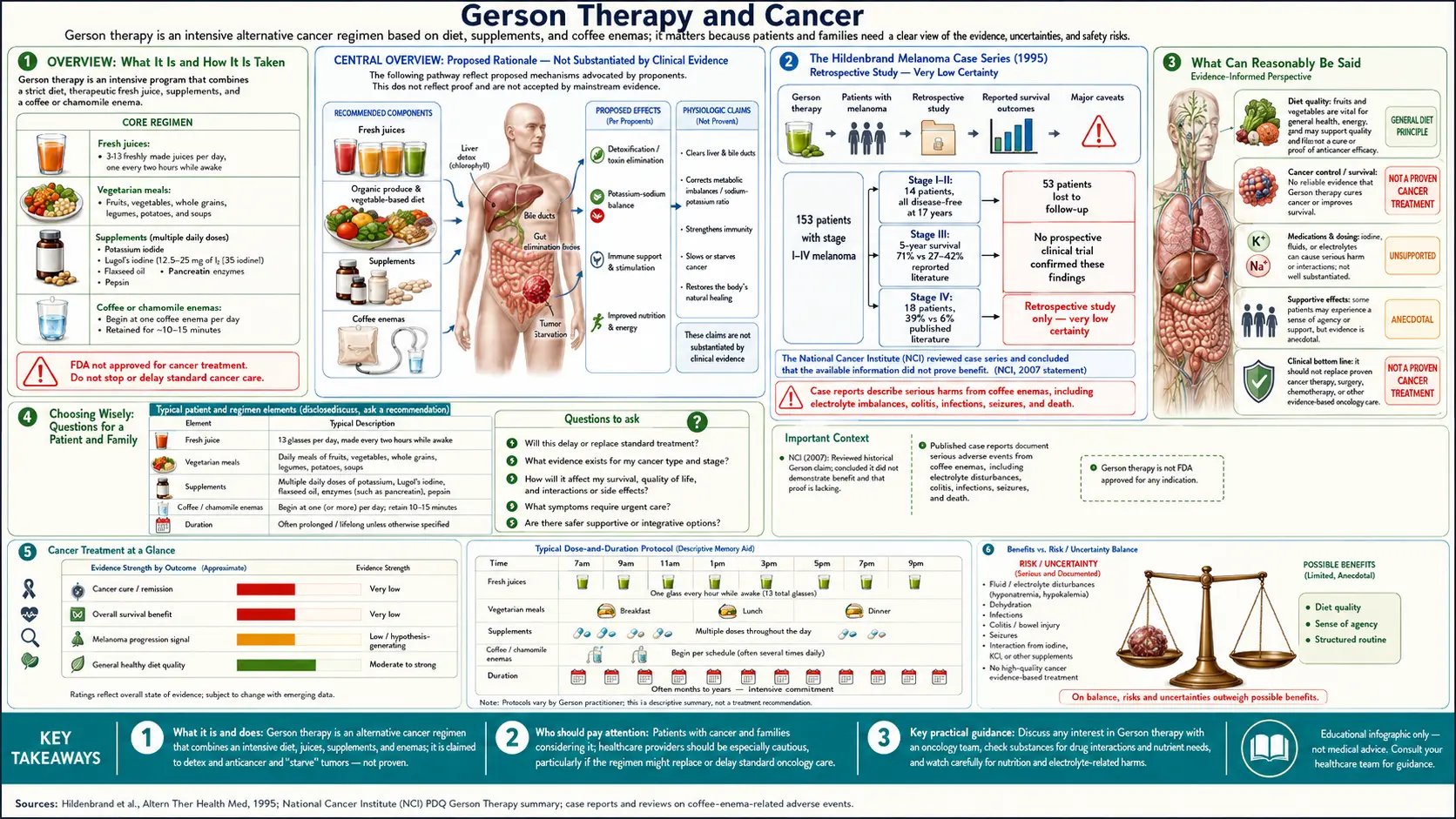
Table of Contents
- Overview
- The Metabolic Theory of Cancer
- Gerson’s Fifty Cases (1958)
- The Hildenbrand Melanoma Case Series (1995)
- The NCI Best Case Series Review
- The Mainstream Oncology Position
- What Can Reasonably Be Said
- Integration with Conventional Care
- The Most Serious Harm: Delayed Effective Treatment
- Choosing Wisely: Questions for a Patient and Family
- Key Research and Sources
- Featured Videos
Overview
Of all the indications for which Gerson Therapy is used, cancer is both the most common and the most contested. The Gerson Institute publishes patient testimonials and case-series data from its affiliated Tijuana clinic claiming long-term remission of advanced cancers, including melanoma, ovarian cancer, lymphoma, and others. The National Cancer Institute, the American Cancer Society, Cancer Research UK, and Memorial Sloan Kettering have each reviewed the protocol and concluded the available evidence does not support efficacy claims and that patients who substitute Gerson for conventional cancer treatment risk significant harm.
Both sets of statements are accurate accounts of what their respective sources publish. The purpose of this page is to lay out the published claims and the published critiques alongside each other, so a reader can form an informed view rather than relying on a one-sided summary from either side.
The Metabolic Theory of Cancer
Gerson’s framing was that cancer is a systemic metabolic disease, not primarily a local disease of mutated cells. He argued that the body’s capacity to recognize and resolve abnormal cell growth depends on cellular sodium–potassium balance, hepatic detoxification capacity, immune competence, and adequate iodine and thyroid function. When these systems failed, tumors grew; when they were restored, tumors regressed.
The metabolic-theory framing was idiosyncratic in 1945 but is not entirely without modern echoes. Otto Warburg’s aerobic-glycolysis observations from the 1920s, the modern interest in the Warburg effect, and Thomas Seyfried’s work on a ketogenic-metabolic approach to cancer, all share the premise that tumor metabolism is a tractable therapeutic target. None of these modern versions endorse the specific Gerson protocol, but the conceptual category is alive.
The mainstream molecular biology of cancer — mutations in oncogenes and tumor suppressors, loss of cell-cycle checkpoints, evasion of apoptosis, induction of angiogenesis, immune escape — is on far stronger empirical ground than the metabolic-theory framing, but it does not exclude the possibility that nutritional and metabolic interventions modify the natural history of cancer in some patients.
Gerson’s Fifty Cases (1958)
Gerson’s book A Cancer Therapy: Results of Fifty Cases presents fifty patient case histories, mostly with biopsy reports, imaging, and follow-up notes. Among the cases are biopsy-confirmed osteosarcoma, melanoma, lymphosarcoma, breast adenocarcinoma, and several others, with reports of complete remissions lasting five years or more. The book is freely available in full from the Gerson Institute website and is widely cited in alternative-medicine literature.
The methodological problems are the ones that recur across all twentieth-century case-series literature: no controls, selection bias toward favorable outcomes (the unsuccessful cases were not the ones written up in book form), incomplete follow-up, dependence on outside-clinic biopsies of variable quality, and the well-known phenomenon of cancer misdiagnosis at the period’s pathology standards. The cases are not refuted by these limitations — some patients clearly did experience long-term remissions of pathology-confirmed cancer — but they cannot establish a response rate.
The Hildenbrand Melanoma Case Series (1995)
The single most-cited modern Gerson outcome study is Gar Hildenbrand and colleagues’ 1995 retrospective review in Alternative Therapies in Health and Medicine, “Five-year survival rates of melanoma patients treated by diet therapy after the manner of Gerson.” The study reviewed 153 melanoma patients treated at a Mexican Gerson-style clinic between 1975 and 1990. Reported five-year survival figures by stage:
- Stages I and II combined: 100%
- Stage IIIA: 82%
- Stage IIIB: 70%
- Stage IVA: 39%
The authors compared these figures to historical control survival rates from the era’s SEER and AJCC databases and reported them as substantially superior. The study has been used widely in patient-facing Gerson literature.
The methodological critiques of the Hildenbrand study are detailed and substantial. Patients were self-selected (those who could afford the Tijuana clinic and who chose Gerson over standard care). Some patients had also received conventional treatment and the contribution of each could not be separated. Follow-up was incomplete — substantial loss to follow-up was not handled in the analysis with modern survival-analysis techniques. The historical-control comparison was drawn from databases of unrelated patients, not contemporaneously matched. And the staging definitions used in the Gerson cohort were not the same as the AJCC definitions used in the comparison — an issue that critics argue inflated the apparent survival difference.
None of these critiques refute the underlying patient outcomes; they refute the comparison to historical controls. What can be said is that some patients with biopsy-confirmed melanoma treated at the Tijuana clinic did experience long-term survival; what cannot be said is that this long-term survival exceeded what would have been seen with conventional treatment in matched patients.
The NCI Best Case Series Review
In the 1990s the National Cancer Institute’s Office of Cancer Complementary and Alternative Medicine reviewed a set of cases submitted by the Gerson Institute under its Best Case Series program, which is designed to identify alternative treatments worth formal investigation. The NCI concluded that the documentation submitted did not meet the program’s standards for case-series review — primarily because of incomplete pathology, incomplete follow-up, and inability to verify diagnosis through original biopsy material in many cases.
The Gerson Institute’s position is that the NCI’s documentation requirements are unrealistic for clinics operating outside the United States and that the agency’s rejection reflected procedural rather than substantive concerns. The NCI’s position is that without verifiable documentation it cannot recommend the protocol for formal trial. The standoff has not been resolved.
The Mainstream Oncology Position
The consolidated position of mainstream oncology, as expressed in formal reviews from the major bodies, is that:
- The available evidence does not support claims that Gerson Therapy cures cancer or extends life in cancer patients.
- Several components of the protocol have biological plausibility (plant-rich diet, low sodium, potassium repletion) and may overlap with general supportive care.
- Several components have known harms (high-dose iodine, frequent coffee enemas, multi-supplement schedule with drug interactions).
- The most consistently documented harm is the delay or replacement of effective conventional treatment in patients who would have had a high probability of cure or long-term control with standard therapy.
Reviews supporting this position include Cassileth’s 2010 piece in Oncology, the American Cancer Society’s alternative-therapies summary, the National Cancer Institute’s patient-information PDQ entry on Gerson, Memorial Sloan Kettering’s integrative-medicine review, and Cancer Research UK’s patient resources.
What Can Reasonably Be Said
An honest summary of the cancer evidence on Gerson is something like this: there are individual patients with biopsy-confirmed cancer who have undergone the protocol and experienced unexpectedly long survival or apparent complete remission. The number of such cases is unknown. There is no randomized or rigorously controlled comparison establishing that the protocol changes the natural history of any specific cancer, and there is no biological mechanism that the modern evidence-based oncology community accepts as compelling.
If the protocol does have an effect, the most likely candidate mechanisms are: substantial weight stabilization and nutritional repletion in cachectic patients (which can extend survival even without affecting the tumor); high intake of plant phytochemicals with mild anti-inflammatory and pro-immune effects; placebo and patient-engagement effects which are larger in motivated, supported patients; and stabilization of comorbidities (cardiovascular, metabolic) that contribute to mortality in patients with advanced cancer. None of these candidate mechanisms suggest that the protocol replaces effective conventional treatment for treatable disease.
Integration with Conventional Care
A fraction of patients use elements of the Gerson Therapy alongside conventional oncology rather than instead of it — eating the diet, juicing, sometimes performing one to two coffee enemas a day to manage chemotherapy-associated constipation. The Gerson Institute’s formal position is that the protocol is most effective in its full form, but the Institute does work with patients who choose to integrate.
From a conventional-medicine standpoint, the dietary components are largely compatible with chemotherapy and radiation, with caveats about food safety in immunocompromised patients (raw produce poses infection risk during neutropenia). The supplement schedule has many drug interactions and must be coordinated with the oncology team. The coffee enema component is the one most often dropped during active treatment.
The Most Serious Harm: Delayed Effective Treatment
The recurring tragedy in alternative-cancer-medicine case reports is the patient with a highly treatable cancer — early-stage melanoma, hormone-receptor-positive breast cancer, testicular cancer, Hodgkin lymphoma, low-stage colorectal cancer — who chooses Gerson or another alternative protocol in lieu of conventional treatment, and presents months or years later with metastatic, no-longer-curable disease. These patients are not always represented in the published Gerson outcomes, because by the time they reach a hospital they are no longer Gerson patients; they are conventional-oncology patients with advanced incurable disease.
For any patient considering substituting Gerson for conventional care, the single most important information is the prognosis with conventional treatment for their specific cancer at their specific stage. For some advanced cancers with poor conventional outcomes, the calculation differs from for early-stage curable cancers. This conversation belongs with the oncologist.
Choosing Wisely: Questions for a Patient and Family
- What is the conventional-treatment prognosis for this specific cancer at this specific stage?
- Is the conventional treatment curative-intent, life-extending, or palliative?
- Are the costs of the Gerson Therapy — financial, logistical, social — achievable for this household for 18 to 24 months?
- Is there an oncologist willing to co-manage the patient on a combined protocol?
- Is the patient electrolyte-stable, cardiovascularly stable, and free of contraindications to the supplement schedule?
- What is the “decision point” at which the patient and family will reassess if the protocol is not producing the expected response?
These are not easy questions. They are the questions that lead to a decision the patient can stand behind.
Key Research and Sources
- Gerson M (1958). A Cancer Therapy: Results of Fifty Cases.
- Hildenbrand GL et al. (1995). Five-year survival in melanoma patients on Gerson diet therapy. Alternative Therapies in Health and Medicine. PMID: 9359807
- Cassileth B (2010). Gerson regimen. Oncology (Williston Park). PMID: 20361473
- Green S (1992). A critique of the rationale for cancer treatment with coffee enemas and diet. JAMA. PMID: 1610542
- National Cancer Institute. “Gerson Therapy (PDQ): Health Professional Version.” cancer.gov
- Memorial Sloan Kettering. “Gerson Therapy.” mskcc.org
- Cancer Research UK. “Gerson Therapy.” cancerresearchuk.org
- PubMed search: “Gerson therapy cancer”
- PubMed search: “alternative cancer therapy delayed treatment”
Connections
- Gerson Therapy
- Research Evidence
- History of Max Gerson
- Coffee Enemas
- Gerson Detoxification
- Juicing
- Diet Protocol
- Gerson Supplements
- Cancer
- Lymphoma
- Coffee & Cancer Prevention
- Fenbendazole
- Potassium
- Iodine
- Full Body MRI
- Leukemia
- Metastatic Cancers
- Turkey Tail Mushroom