Gerson Therapy Research and Evidence
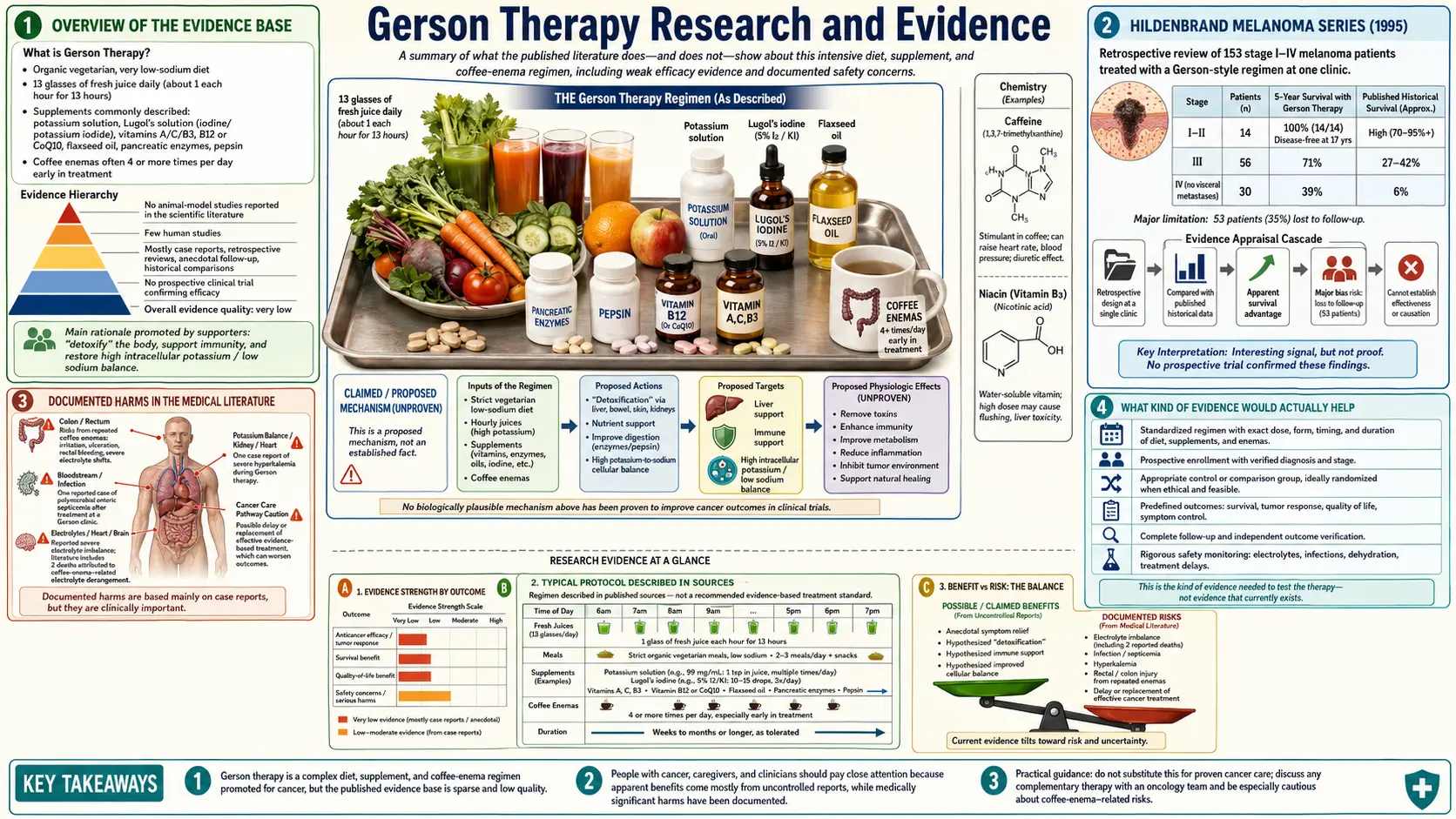
Table of Contents
- Overview of the Evidence Base
- The Sauerbruch–Herrmannsdorfer–Gerson Tuberculosis Trial (1929)
- Gerson’s Fifty Cases (1958)
- Hildenbrand Melanoma Series (1995)
- Molassiotis and Peat Survey (2007)
- The Cassileth Critique (2010)
- The Green JAMA Critique (1992)
- Documented Harms in the Medical Literature
- Evidence on Individual Components
- Systematic Reviews and Major-Body Statements
- What Kind of Evidence Would Actually Help
- Key Research and Sources
- Featured Videos
Overview of the Evidence Base
The published evidence on the Gerson Therapy as a complete protocol consists almost entirely of case reports, case series, and clinical narratives. There are no published randomized controlled trials of the full Gerson protocol against any comparator. There are no published prospective cohort studies with rigorous follow-up. The evidence on individual components — high-vegetable diets, low-sodium diets, juicing, coffee, the supplement schedule — is much larger and is mostly drawn from research outside the Gerson framework.
This page summarizes what is in the published record, organized by document, so a reader can see the actual primary sources and their methodological strengths and limitations.
The Sauerbruch–Herrmannsdorfer–Gerson Tuberculosis Trial (1929)
The largest single body of clinical evidence Gerson generated was for skin tuberculosis (lupus vulgaris), not cancer. Conducted at Ferdinand Sauerbruch’s Munich clinic, the trial enrolled 450 patients on the diet, with the published outcome that 446 of 450 healed. The results appeared in the German medical literature in 1929 and were sufficient for the diet to be added to German tuberculosis-treatment guidelines until antibiotic therapy displaced dietary approaches in the 1950s.
By the standards of the 1920s the trial was credible. By modern standards it was not blinded, did not have rigorous controls, did not use modern diagnostic criteria, and was not externally audited. Nevertheless, it remains the single best-documented Gerson outcome and is a useful reminder that the diet has empirical support in at least one indication that is now obsolete.
Gerson’s Fifty Cases (1958)
Gerson’s capstone book presents fifty cancer cases with biopsy reports, imaging, and follow-up notes. The methodological problems — selection bias, no controls, incomplete follow-up, dependence on outside-clinic pathology — are described in detail on the Cancer Treatment page. The cases include genuine documented long-term remissions that cannot simply be explained away, but also do not establish a response rate.
Hildenbrand Melanoma Series (1995)
The Hildenbrand 1995 retrospective review of 153 melanoma patients treated at a Mexican Gerson-style clinic between 1975 and 1990 is the most-cited modern Gerson outcome study. It reported five-year survival rates substantially higher than historical SEER comparators across stages I through IVA. The methodological critiques (self-selected cohort, incomplete follow-up, non-matched historical controls, different staging definitions) are summarized on the Cancer Treatment page. The study is published and citable; whether its conclusions can be carried into clinical decision-making is a separate question.
Molassiotis and Peat Survey (2007)
Molassiotis and Peat published a survey-style examination of patients undergoing Gerson Therapy in Europe in 2007 (Integrative Cancer Therapies). Patients self-reported quality of life, fatigue, mood, and general well-being. The study was descriptive and uncontrolled but found that patients on the protocol generally reported acceptable quality-of-life and a sense of agency in their care — outcomes that have value independent of any anti-tumor effect. The study did not assess survival or tumor response.
The Cassileth Critique (2010)
Barrie Cassileth, then chief of the Integrative Medicine Service at Memorial Sloan Kettering, published a 2010 review in Oncology (Williston Park) describing the Gerson regimen as “not based on accepted scientific principles” and warning against its use as a substitute for evidence-based cancer treatment. Cassileth’s review summarizes the prior literature, the harms documented in case reports, and the failure of the protocol to meet evidence standards for efficacy claims. It is the most-cited mainstream-medicine consolidation of the case against Gerson.
The Green JAMA Critique (1992)
Saul Green’s 1992 critique in JAMA, “A critique of the rationale for cancer treatment with coffee enemas and diet,” remains the most thorough examination of the Gerson rationale by a biomedical scientist. Green addresses the sodium–potassium theory, the bile flow argument, the GST induction claim, and the case-series literature point by point. The article is contentious and the Gerson Institute has published rebuttals, but Green’s arguments have not been substantively answered in the peer-reviewed literature.
Documented Harms in the Medical Literature
Several specific harms have been documented in case reports:
- Eisele and Reay (1980, JAMA) — two deaths directly attributed to coffee enemas, both from severe electrolyte derangement and one with seizures.
- Margolin and Green (1984, Western Journal of Medicine) — polymicrobial enteric septicemia from coffee enemas.
- Keum et al. (2010) — rectal mucosal injury from coffee enemas in a single-center Korean series.
- Lee et al. (2008) — case report of severe proctocolitis from frequent coffee enema use.
- Case reports of hyponatremia, hypokalemia, dehydration, and cardiac arrhythmia in Gerson patients on multiple-times-daily enema schedules.
- The most consistently documented harm in mainstream-medicine reviews: delayed presentation for effective conventional cancer treatment in patients whose cancer was potentially curable at the time they chose Gerson.
Evidence on Individual Components
The components of the Gerson Therapy taken individually have very different evidence profiles:
- Plant-rich, low-sodium, organic diet: Substantial supporting evidence from cardiovascular epidemiology (DASH, Mediterranean), cancer epidemiology, and metabolic-syndrome research. The strongest component of the protocol.
- Heavy juicing: Modest evidence for general nutritional density; little evidence for unique effect beyond what the equivalent whole-food diet would provide.
- High potassium intake: Supporting evidence in hypertension and cardiovascular disease; risks well documented in patients with renal impairment.
- High-dose iodine: Limited supporting evidence; significant risks; controversial.
- Thyroid replacement: Supported in patients with documented hypothyroidism; not supported as a generic intervention.
- Coffee enemas: Mechanistic plausibility; no human outcome trials; documented harms.
- Pancreatic enzymes for cancer: Negative trial in pancreatic cancer (Chabot 2010); insufficient evidence in other cancers.
- Niacin (B3): Evidence for cardiovascular use; not specific to cancer.
- CoQ10: Modest evidence in cardiovascular and possibly breast cancer adjunctive use.
Systematic Reviews and Major-Body Statements
Major systematic reviews and position statements:
- National Cancer Institute PDQ entry on Gerson Therapy (current).
- American Cancer Society Complementary and Alternative Methods review (current).
- Memorial Sloan Kettering Integrative Medicine entry on Gerson and on coffee enemas (current).
- Cancer Research UK patient information on Gerson Therapy (current).
- Cochrane review database: no completed systematic review of Gerson Therapy as of the most recent search; the absence reflects the lack of trial data eligible for systematic review.
- NIH National Center for Complementary and Integrative Health: no separate Gerson position statement; categorizes the protocol under unproven cancer interventions.
What Kind of Evidence Would Actually Help
The Gerson controversy is unlikely to be resolved by another retrospective case series. The studies that would settle the question are:
- A prospective cohort study with rigorous documentation of stage at entry, conventional treatment received (or refused), and complete follow-up to event or end of study, comparing Gerson Therapy to declined conventional care in matched populations.
- A randomized comparison of full Gerson plus standard-of-care versus standard-of-care alone in a specific cancer type with poor conventional outcomes — pancreatic cancer, glioblastoma, or refractory metastatic melanoma might be appropriate where adjunctive use carries low downside risk.
- A pharmacokinetic study of rectal versus oral administration of coffee diterpenes in healthy volunteers, to settle the portal-circulation hypothesis.
- A controlled trial of the Gerson diet alone (without enemas, without supplements) versus an equivalent Mediterranean diet in chronic disease populations, to test whether the most controversial components add value over a more conventional plant-based dietary pattern.
None of these studies has been done. Until they are, the published evidence on Gerson will remain what it is: a body of compelling individual case histories that have not been validated against controlled comparators, plus a body of well-documented harms that has been validated against controlled comparators.
Key Research and Sources
- Sauerbruch F, Herrmannsdorfer A, Gerson M (1929). Reports on the dietary treatment of skin tuberculosis. Münchener Medizinische Wochenschrift.
- Gerson M (1958). A Cancer Therapy: Results of Fifty Cases.
- Hildenbrand GL et al. (1995). Alternative Therapies in Health and Medicine. PMID: 9359807
- Molassiotis A, Peat P (2007). “Surviving against all odds: analysis of 6 case studies of patients with cancer who followed the Gerson therapy.” Integrative Cancer Therapies. PMID: 17351029
- Cassileth B (2010). Gerson regimen. Oncology (Williston Park). PMID: 20361473
- Green S (1992). A critique of the rationale for cancer treatment with coffee enemas and diet. JAMA. PMID: 1610542
- Eisele JW, Reay DT (1980). Deaths related to coffee enemas. JAMA. PMID: 7362851
- Margolin K, Green M (1984). Western Journal of Medicine. PMID: 6730482
- Chabot JA et al. (2010). Journal of Clinical Oncology. PMID: 19687327
- National Cancer Institute PDQ. Gerson Therapy. cancer.gov
- PubMed search: “Gerson therapy”
- PubMed search: “coffee enema adverse”
Connections
- Cancer Treatment
- Gerson Therapy
- Coffee Enemas
- Detoxification
- History of Max Gerson
- Diet Protocol
- Supplements
- Juicing
- Niacin and Vitamin B3
- Cancer
- Tuberculosis
- Potassium
- Coffee
- Cardiovascular Disease
- Lupus