Adrenal Cortisol & Mineral Metabolism
One of the most common functional-medicine diagnoses of the past two decades is “adrenal fatigue.” Patients arrive exhausted at 7 AM, wired at 11 PM, salt-craving, dizzy on standing, anxious, and unable to handle stress that they used to absorb without noticing — and a clinician somewhere told them their adrenals were “burned out.” Mainstream endocrinology, with some justification, pushes back: the only adrenal failure they recognize is Addison’s disease, an autoimmune destruction of the adrenal cortex that requires lifelong hydrocortisone replacement, and they correctly point out that the “adrenal fatigue” literature has not produced reproducible diagnostic criteria. Morley Robbins agrees with the endocrinologists on a narrow point and disagrees on a much bigger one. He agrees that the adrenals are not “burning out” in any literal histological sense. He disagrees that nothing is happening. His reformulation: the adrenals cannot burn out, but the cofactors the adrenals need to make hormones can and do — and what the world calls adrenal fatigue is, underneath the symptoms, a mineral-exhaustion syndrome.
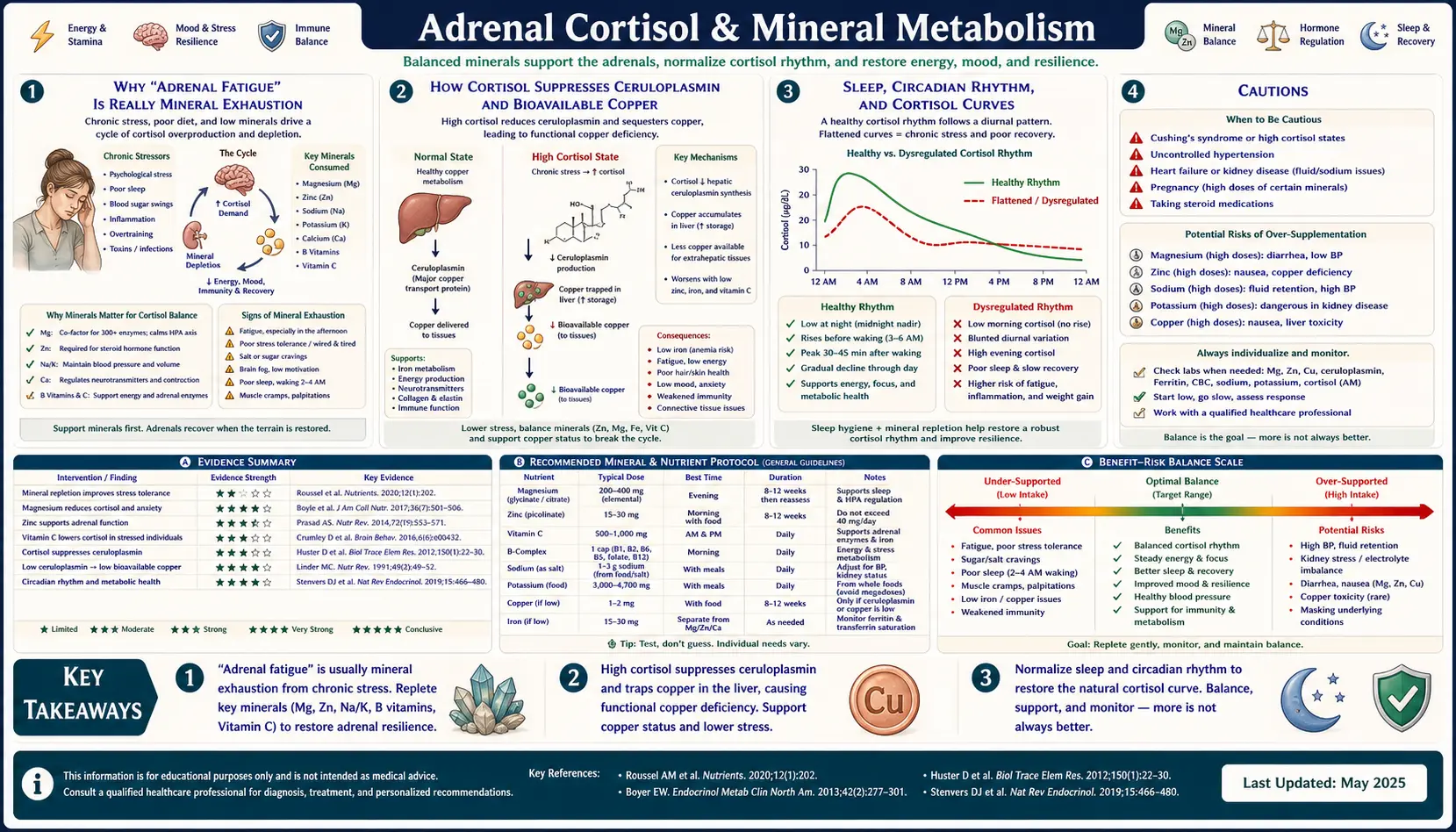
This page lays out the HPA axis in plain language, walks through how cortisol consumes magnesium and suppresses ceruloplasmin / bioavailable copper, gives the exact recipe for the “Adrenal Cocktail” Robbins teaches, lists the whole foods that rebuild adrenal cofactors, explains the cortisol curve and how to read a 4-point salivary cortisol panel, and ends with the lifestyle resets that consistently move the needle. It is a long page on purpose: this is one of the most-asked, most-confused topics in functional health, and the reader deserves enough information to make an informed decision about their own protocol.
Table of Contents
- Why “Adrenal Fatigue” Is Really Mineral Exhaustion
- The HPA Axis in Plain Language
- How Cortisol Burns Through Magnesium
- How Cortisol Suppresses Ceruloplasmin and Bioavailable Copper
- The Adrenal Cocktail: Recipe and Rationale
- Whole-Food Adrenal Support
- Sleep, Circadian Rhythm, and Cortisol Curves
- Saliva Cortisol Testing (DUTCH and Standard 4-Point)
- Lifestyle Resets That Move the Needle
- Cautions
- Key Research Papers
- Connections
- Featured Videos
1. Why “Adrenal Fatigue” Is Really Mineral Exhaustion
The phrase “adrenal fatigue” was popularized in 1998 by James Wilson, ND, and has since been adopted by enough alternative practitioners that it has become a category of self-diagnosis. Mainstream endocrinology, including a 2016 BMC Endocrine Disorders systematic review, found no consistent biochemical or histological evidence for the entity, and most reviews conclude that “adrenal fatigue” is not a recognized medical diagnosis. True adrenal failure is Addison’s disease — an autoimmune destruction of the adrenal cortex that produces low cortisol, low aldosterone, hyperpigmentation, salt craving, severe fatigue, and life-threatening adrenal crisis if untreated. Addison’s is rare (4–6 per 100,000), has clear lab signatures (low morning cortisol, elevated ACTH, failed cosyntropin stimulation test), and requires hormone replacement; it is not what the “adrenal fatigue” tribe is describing.
So what is the patient experiencing? Robbins’s reformulation, drawn from his work with the Magnesium Advocacy Group and his Root Cause Protocol consultants, is straightforward: the HPA axis cannot manufacture adequate cortisol, aldosterone, DHEA, or epinephrine without specific cofactors — copper, magnesium, retinol (vitamin A), B vitamins, and cholesterol. When those cofactors are depleted, the adrenal cortex can’t keep up with stress demand. The hypothalamus and pituitary keep shouting (CRH and ACTH go up), but the adrenal output sputters. The patient runs on adrenaline (norepinephrine surge) to compensate for inadequate cortisol — hence the “wired and tired” presentation. Restore the minerals, restore the function. As Robbins puts it: “You can’t burn out your adrenals — you can only burn out the cofactors that adrenals need.”
This is not as fringe as it sounds. The adrenal cortex contains the highest concentration of vitamin C in the human body. Cortisol synthesis requires NADPH (B-vitamin–dependent) and a copper-containing electron transfer step. Aldosterone is synthesized by CYP11B2, an iron- and copper-coupled enzyme. The chronic-stress “burnout” phenotype maps cleanly onto a copper–magnesium–retinol depletion pattern. The mainstream view (“there’s nothing wrong with your adrenals”) and the popular view (“your adrenals are burned out”) are both incomplete. Robbins’s view — that the adrenal output reflects the cofactor balance at the gland, and that the gland itself is fine — is a more useful working model.
2. The HPA Axis in Plain Language
HPA stands for Hypothalamus – Pituitary – Adrenal. It is the body’s slow-acting stress response system, layered on top of the fast-acting sympathetic-nervous-system (fight-or-flight) response. Here’s the chain in plain English:
- Hypothalamus (deep in the brain) senses a stressor — physical, emotional, infectious, hypoglycemic, or blood-pressure drop — and releases CRH (corticotropin-releasing hormone).
- Pituitary (just below the hypothalamus) receives CRH and secretes ACTH (adrenocorticotropic hormone) into the bloodstream.
- Adrenal cortex (the outer layer of the adrenal glands, which sit on top of the kidneys) receives ACTH and produces three hormone families from three zones:
- Zona glomerulosa → aldosterone (regulates sodium retention and potassium excretion in the kidney)
- Zona fasciculata → cortisol (raises blood glucose, suppresses inflammation, mobilizes fat and protein)
- Zona reticularis → DHEA and androgens (precursors to sex hormones, modulators of immunity)
- Adrenal medulla (the inner core, embryologically related to nervous tissue) produces epinephrine and norepinephrine in seconds during acute stress.
- Negative feedback: cortisol travels back to the hypothalamus and pituitary and shuts down further CRH and ACTH release. Chronic stress disrupts this loop.
A few cofactor facts that matter: all steroid hormones start from cholesterol. Pregnenolone is made from cholesterol; from pregnenolone the body branches into cortisol, aldosterone, DHEA, progesterone, testosterone, and estradiol. Very-low-cholesterol diets (or aggressive statin protocols) can leave the HPA axis short on raw material. Cortisol synthesis uses CYP enzymes that require iron-sulfur clusters, copper-containing electron carriers, and NADPH (regenerated by B-vitamin–dependent pathways). Aldosterone synthesis goes through CYP11B2, the same enzyme family. None of this is exotic biochemistry; it’s in any standard endocrinology textbook. What Robbins adds is the practical observation that the cofactors are routinely depleted by modern life, and restoring them — rather than adding adaptogens on top of a deficient foundation — is the order of operations.
3. How Cortisol Burns Through Magnesium
Magnesium is the second-most-abundant intracellular cation after potassium and is required for more than 300 enzymatic reactions, most of them ATP-dependent. ATP is biologically active only as Mg-ATP — the magnesium ion stabilizes the high-energy phosphate bonds. Every cortisol surge does the following to magnesium reserves:
- Activates ATP-dependent enzymes across the gluconeogenic pathway — glucose-6-phosphatase, fructose-1,6-bisphosphatase, PEPCK, pyruvate carboxylase — all magnesium-dependent.
- Drives gluconeogenesis in the liver, raising blood glucose so the “fight or flight” response has fuel. Each glucose molecule synthesized from amino acids consumes ATP (i.e., consumes Mg).
- Increases urinary magnesium excretion via cortisol-driven changes in renal tubular handling. The “mag-leaky kidney” under chronic cortisol load is well documented.
- Activates the sympathetic nervous system, which further increases catecholamine-driven cellular Mg consumption.
- Suppresses parathyroid hormone’s magnesium-sparing actions, contributing to bone mineral resorption and renal Mg loss.
The cumulative effect: chronic stress produces chronic magnesium drain. Galland (1991) and many subsequent reviews documented this pattern. The drained patient becomes more anxious — because magnesium is required for NMDA-receptor regulation, GABAergic tone, and parasympathetic vagal function — and the increased anxiety produces more cortisol, which produces more magnesium loss. This is a self-reinforcing vicious cycle, and it explains why the chronically stressed patient is also chronically deficient in magnesium even when their diet looks reasonable on paper. Replenishing magnesium is the single most leveraged intervention in this loop. Robbins favors magnesium glycinate for general repletion (well absorbed, calming on the nervous system), magnesium taurate for cardiovascular support, magnesium malate for energy and muscle pain, and magnesium threonate for cognition. He avoids magnesium oxide (poorly absorbed, primarily a laxative) and is cautious about magnesium citrate at high doses (gastrointestinal effects). Topical magnesium (oil or flakes in a footbath) is added for severe deficiency.
4. How Cortisol Suppresses Ceruloplasmin and Bioavailable Copper
Ceruloplasmin is the copper-carrying protein in plasma and the enzyme that performs ferroxidase activity — oxidizing iron from Fe²⁺ to Fe³⁺ so it can be loaded onto transferrin. (See the Ceruloplasmin deep-dive for the full story.) Ceruloplasmin is synthesized in the liver, and its production is responsive to several upstream signals: copper supply, retinol (vitamin A) signaling, magnesium-dependent cellular energy state, and — importantly — glucocorticoids.
The picture is nuanced. Acute, short-lived cortisol surges increase ceruloplasmin as part of the acute-phase response (ceruloplasmin behaves as a positive acute-phase reactant in inflammation). But chronic high cortisol — the “stuck-on” pattern of ongoing stress, chronic inflammation, or steroid medication — produces a different effect: hepatic ceruloplasmin synthesis becomes dysregulated, the protein is increasingly produced in an apo (copperless) form, and the functional ferroxidase activity drops. Cortisol also drives intracellular shifts of copper and zinc that pull copper out of the bioavailable pool. Robbins’s argument: the chronically “wired and tired” person is in a state where the adrenals are demanding cortisol, the cofactors aren’t there to make it efficiently, the body upregulates ACTH, ceruloplasmin’s enzymatic activity is impaired, iron starts to dysregulate, and the patient runs on adrenaline (norepinephrine) instead. The result is the classic presentation: tired in the morning, wired at night, anxious, salt-craving, and no longer able to handle even moderate stress.
Practically, what this means for the patient: addressing chronic stress is not an optional add-on to mineral repletion — it’s a structural part of it. You cannot copper-load your way out of cortisol-driven copper sequestration. The cortisol pattern has to come down for the ceruloplasmin to come back up.
5. The Adrenal Cocktail: Recipe and Rationale
The “Adrenal Cocktail” is the single best-known practical recommendation in the Root Cause Protocol. It is not a stimulant, not a supplement stack, and not a meal replacement — it is a small mineral- and glycogen-replenishing drink taken twice between meals to support adrenal cofactor availability when cortisol is naturally dipping.
The basic recipe (one serving):
- 4 oz fresh-squeezed orange juice — provides ~190 mg potassium, whole-food vitamin C as ascorbic acid plus the flavonoid matrix, and fructose for liver glycogen replenishment. Bottled juice is acceptable but fresh is preferred. Robbins is emphatic that the whole-food matrix matters — the adrenal cortex sits in the highest vitamin-C concentration in the body, and synthetic ascorbic acid alone is not the same as the orange.
- ¼ tsp cream of tartar (potassium bitartrate) — about 470 mg of potassium per quarter teaspoon. Cream of tartar is a baking-aisle staple, cheap, and is one of the most concentrated potassium sources available outside of supplements.
- ¼ tsp Celtic Sea Salt — provides ~580 mg of sodium plus 60–80 trace minerals from the salt’s mineral complex. Robbins specifies real salt rather than refined sodium chloride; the trace minerals (chromium, magnesium, manganese, zinc, etc.) are the point.
- Mix in 8 oz water (or coconut water) and drink.
Optional additions:
- 1 tablespoon grass-fed collagen (glycine support for liver phase II and cortisol clearance)
- Splash of coconut water instead of plain water (adds 100–200 mg potassium and electrolytes)
- Pinch of magnesium glycinate powder (combines magnesium repletion with the cocktail; some patients find it eases muscle tension within 20–30 minutes)
- ½ tsp shilajit (full-spectrum trace minerals, fulvic acid)
- A squeeze of fresh lemon (additional vitamin C and bioflavonoids)
Timing is non-negotiable in Robbins’s teaching. The cocktail is taken at the two natural cortisol “dips”:
- Mid-morning, around 10:00–10:30 AM (between breakfast and lunch)
- Mid-afternoon, around 3:00–3:30 PM (between lunch and dinner)
These are the windows when adrenal demand outpaces blood-glucose and electrolyte availability for many people, producing the “3 PM crash.” The cocktail front-loads the cofactors before the dip rather than reacting to it with caffeine and sugar.
The rationale, point by point:
- Potassium is the major intracellular cation, depleted by stress, by high cortisol, and by aldosterone-driven kidney potassium losses. Most modern diets are potassium-poor relative to the ancestral diet.
- Sodium is needed for aldosterone-mediated sodium retention, plasma volume, and adrenal blood pressure regulation. Salt-craving is a classic sign of a low-aldosterone state.
- Whole-food vitamin C with flavonoids supports the adrenal cortex (which holds the body’s highest tissue concentration of vitamin C), supports collagen synthesis, and supports copper-dependent enzymes including dopamine beta-hydroxylase.
- Trace minerals from real salt provide cofactor breadth that refined NaCl cannot.
- Fructose from orange juice rebuilds liver glycogen, blunting the cortisol–adrenaline response that would otherwise kick in if blood glucose dropped between meals.
6. Whole-Food Adrenal Support
Beyond the cocktail, the adrenal cortex is rebuilt — or kept intact — by a whole-food diet that supplies cholesterol, fat-soluble vitamins, B vitamins, copper, magnesium, retinol, glycine, and trace minerals. The Robbins-aligned shopping list:
- Whole eggs — cholesterol (steroid hormone substrate), choline, B vitamins, retinol from yolk. Pasture-raised when possible.
- Avocados — potassium (~975 mg per fruit), monounsaturated fat, magnesium, folate.
- Coconut oil and MCT — medium-chain fatty acids that are absorbed without bile and don’t require an insulin spike, supporting steady cortisol-stable energy.
- Grass-fed butter / ghee — vitamin A (retinol), vitamin K2, butyrate, conjugated linoleic acid.
- Bone broth — collagen, glycine (key for cortisol clearance and GABAergic tone), proline, minerals from long-simmered bones.
- Sea vegetables — iodine for the thyroid (which interlocks with the adrenals in the HPT-A axis), trace minerals.
- Pastured liver — the single densest food source of copper, retinol, B5 (pantothenic acid — the “anti-stress vitamin”), B12, folate, and choline. Even 1–2 oz once per week meaningfully shifts the cofactor pool.
- Bee pollen — full-spectrum micronutrients including B vitamins, trace minerals, amino acids; one of the RCP “Starts.”
- Cacao and dark chocolate — magnesium (highest food source by weight), copper, theobromine for gentle vasodilation.
- Wild salmon, sardines, herring — omega-3, vitamin D from sunlight-fed fish, B12, selenium.
- Adaptogens (with caveats): real cordyceps, ashwagandha, rhodiola, holy basil. Robbins is cautious about long-term adaptogen use without a mineral foundation underneath — adaptogens modulate the HPA axis but cannot substitute for missing cofactors. They are layered on top of the mineral protocol, not in place of it.
7. Sleep, Circadian Rhythm, and Cortisol Curves
A healthy diurnal cortisol curve is one of the most reliable signs of an intact HPA axis. The pattern looks like this:
- Cortisol Awakening Response (CAR) — cortisol rises by 50% within 30–45 minutes of waking. This is the “turn the engine on” signal.
- Morning peak — 6–8 AM, around 15–20 µg/dL in serum, higher still in salivary readings adjusted to local lab ranges.
- Steady decline through the day — cortisol falls in a smooth taper, with smaller dips around 10 AM and 3 PM.
- Nadir at midnight — below 3 µg/dL serum.
- Slow rise through the early morning hours, peaking again at waking.
HPA dysfunction patterns show up as deviations from this curve:
- Flat curve, high all day — chronic active stress, no clear peak, no clear dip; the patient is constantly in stress-response mode.
- Inverted curve (low AM, high PM) — common in shift workers and severe insomniacs; the body is trying to wake up at night and sleep during the day.
- Low overall (low AM, low PM) — late-stage HPA dysfunction; the cofactors are exhausted and the gland output is low across the board. This is the closest thing to the popular “adrenal fatigue” phenotype, and it’s the one most likely to respond to mineral repletion.
- High AM, low PM (over-shoot then collapse) — an early-stage stress pattern; the morning surge overshoots the receptor capacity and the rest of the day runs flat.
Sleep disruption is both cause and consequence. Cortisol naturally rises around 11 PM if the body is still awake (the “second wind”), making sleep onset harder. Targeting bedtime by 10:30 PM, no blue light after 9 PM, morning sunlight within 30 minutes of waking, and earthing/grounding can reset the curve over weeks. (See the Sleep Hygiene page for the full protocol.)
8. Saliva Cortisol Testing (DUTCH and Standard 4-Point)
Serum cortisol — a single blood draw — tells you almost nothing about HPA dynamics. Cortisol pulses, varies hour-to-hour, and a one-time number captures only a single point on a curve that’s changing across the day. The two functional tools:
- 4-point salivary cortisol — samples taken at waking, 30 minutes after waking (CAR), noon, 4 PM, and bedtime. Plots the diurnal curve. Available through ZRT Laboratory, Genova Diagnostics, and Precision Analytical. Typical out-of-pocket cost: $150–$250 USD. Results show the shape of the curve, not just total cortisol output.
- DUTCH (Dried Urine Total Comprehensive Hormones) — from Precision Analytical. Uses dried urine spots collected at 4–5 timepoints. Adds cortisol metabolites (5α- and 5β-tetrahydrocortisol, etc.) to the picture, which lets the practitioner distinguish between low cortisol production and rapid cortisol clearance — two very different problems with the same surface-level lab value. Also includes DHEA-S, sex hormones, and melatonin metabolites. Cost: $300–$450 USD typical.
For most patients exploring HPA dysfunction, the standard 4-point salivary panel is enough to start. The DUTCH is added when the picture is complex (e.g., mixed sex-hormone symptoms layered on top of cortisol issues, or suspected fast cortisol metabolism).
9. Lifestyle Resets That Move the Needle
The mineral cofactors are necessary but not sufficient. The HPA axis is also trained by daily inputs, and a small set of lifestyle changes consistently moves cortisol curves back toward normal in 4–12 weeks:
- Morning sunlight, 5–15 minutes within 30 minutes of waking. Direct skin and eye exposure (no sunglasses) anchors the suprachiasmatic nucleus and reinforces the cortisol awakening response.
- Stop caffeine after noon. Caffeine’s half-life is 5–6 hours; an afternoon coffee is still 25% present at bedtime. Late caffeine compresses sleep architecture and prevents the deep-sleep cortisol nadir.
- Box breathing or coherent breathing, 5 minutes twice daily. Inhale 4 seconds, hold 4, exhale 4, hold 4. Or 6 seconds in, 6 seconds out. Both activate vagal tone and shift the autonomic balance toward parasympathetic.
- Cold exposure, 1–3 minutes at the end of a shower. Trains norepinephrine response, raises baseline mood and resilience over weeks.
- Bedtime by 10:30 PM. The body’s second cortisol surge fires around 11 PM if you’re still awake; missing that window is the single most common driver of the “wired at midnight” pattern.
- Magnesium glycinate, 200–400 mg, 30 minutes before bed. Improves sleep onset, deepens sleep architecture, lowers next-day cortisol.
- Adrenal cocktail, 2× daily as described above.
- Real salt on water in the morning — a pinch of Celtic sea salt in 16 oz of water on waking, before food.
- Earthing/grounding — bare feet on grass, sand, or earth for 10–20 minutes daily. Effects on cortisol curves and inflammation markers have been measured (Chevalier et al., several reviews) and the practice is essentially free.
- Resistance training, 2–3× per week, short and intense. Builds adrenal-cortex resilience without overtraining-driven cortisol elevation that endurance running can produce.
- Walks after meals. 10 minutes after lunch and dinner improves glucose disposal and prevents the post-meal cortisol bump.
10. Cautions
- True Addison’s disease (autoimmune adrenal failure, primary adrenal insufficiency) requires hydrocortisone replacement. It is not a “mineral protocol” condition. Lab confirmation is essential: low morning cortisol, elevated ACTH, and a failed cosyntropin (ACTH) stimulation test. If you have unexplained fatigue with hyperpigmentation, salt craving, low blood pressure, low sodium, and high potassium, get tested for Addison’s before pursuing functional protocols.
- Hypertension or kidney disease — the adrenal cocktail contains meaningful sodium and potassium. Patients with stage 3+ chronic kidney disease, on potassium-sparing diuretics, or with poorly controlled hypertension should clear the recipe with their physician. The principle is sound for most people; the doses may need adjustment.
- Hyperaldosteronism (Conn’s syndrome) — high aldosterone with hypertension and low potassium. Sodium loading is the wrong direction here. Test before salting.
- Cushing’s syndrome — cortisol excess (from a pituitary or adrenal tumor, or chronic exogenous steroid use). The opposite condition. Cortisol-lowering interventions, not adrenal-supporting ones, are appropriate.
- Diabetes — orange juice in the standard adrenal cocktail can raise blood glucose meaningfully. A lower-glycemic version: lemon water + Celtic salt + cream of tartar (omit the OJ), or use coconut water with the salt and cream of tartar.
- Pregnancy — the cocktail itself is fine. Adaptogens (ashwagandha, rhodiola) generally are not recommended in pregnancy without practitioner oversight.
- Salivary cortisol testing can be skewed by oral inflammation, recent food or drink, brushing, or steroid mouthwashes. Follow lab instructions exactly; the timing of the morning sample (within 5 minutes of opening eyes) matters more than people realize.
11. Key Research Papers
The PubMed topic searches below open in a new tab and cover the literature that maps to each section of this page. They include both the mainstream endocrinology view (where it converges with Robbins on mechanism) and the functional/integrative literature.
- Cortisol & magnesium depletion
- Glucocorticoids & ceruloplasmin
- Adrenal fatigue — systematic review
- Cortisol awakening response (CAR)
- Salivary cortisol & circadian rhythm
- Adaptogens (ashwagandha) & cortisol
- Potassium, aldosterone & sodium balance
- DHEA & adrenal supplementation
- Stress, HPA axis & cofactors
- Magnesium, anxiety & cortisol
- Addison’s disease — diagnosis
- Cushing’s syndrome — diagnosis
Connections
- Morley Robbins
- Root Cause Protocol
- Ceruloplasmin and Bioavailable Copper
- Copper-Iron Dysregulation
- Magnesium Replenishment
- Iron Overload and Hidden Toxicity
- Vitamin D Controversy
- Whole Food Copper Sources
- Cure Your Fatigue
- Magnesium
- Copper
- Potassium
- Vitamin C
- Vitamin A
- Adrenal Fatigue
- Sleep Hygiene
- Stress Management
- Ashwagandha