Morley Robbins and the Root Cause Protocol


Morley Robbins, MA, CHC, is the founder of the Root Cause Protocol (RCP) — a mineral-balancing framework built around a single, contrarian thesis: that most modern chronic fatigue, inflammation, and metabolic dysfunction trace back to bioavailable copper deficiency driving iron dysregulation, compounded by magnesium depletion and aggressive vitamin D supplementation. After more than thirty years as a hospital administrator, Robbins came to believe that the medical system’s focus on iron as the cure for fatigue had it backwards — that iron without copper’s ferroxidase activity becomes a Fenton-reaction oxidant rather than a cellular asset, and that the “tired and inflamed” population is suffering from copper, magnesium, and retinol depletion masked by hidden iron overload.
This hub is a comprehensive, sourced summary of Robbins’s teaching: the core protocol (the “Stops” and “Starts”), the copper–iron antagonism hypothesis, the role of ceruloplasmin as the master regulator of iron metabolism, the magnesium “silent epidemic,” the unusual position on vitamin D supplementation, the whole-food sources the RCP emphasizes (beef liver, oysters, cacao, bee pollen), the adrenal–mineral feedback loop, and his 2021 book Cure Your Fatigue. Robbins’s positions are heterodox in several places — particularly on iron supplementation and on cholecalciferol — and we present them clearly, alongside where mainstream physiology agrees and where it diverges. The reader is the audience; this hub does not endorse a specific protocol.
Deep-Dive Articles
1. The Root Cause Protocol — Stops & Starts
The full RCP framework: the four “Stops” (industrial iron, synthetic ascorbic acid, calcium, vitamin D), the five “Starts” (whole-food vitamin C, cod liver oil, magnesium, bee pollen, beef liver), the “Adrenal Cocktail,” and the philosophy of restoring mineral balance instead of chasing symptoms.
2. Copper–Iron Dysregulation: The Central Hypothesis
The Robbins thesis in detail: how unbound iron drives the Fenton reaction, why ceruloplasmin’s ferroxidase activity is the lynchpin of iron homeostasis, and why “low iron, give iron” misses the underlying copper deficiency that prevents iron from being safely loaded into hemoglobin.
3. Ceruloplasmin: The Master Regulator of Iron
What ceruloplasmin is, how to read your labs, the “% bioavailable copper” calculation Robbins uses (serum copper × 3.15 − ceruloplasmin × 3 / serum copper × 100), and why a “normal” total copper can hide a profound functional copper deficiency.
4. Iron Overload & Hidden Iron Toxicity
Why ferritin is an inflammation marker, not a true iron-storage gauge; how unbound iron accumulates in the liver, brain, and heart; why blood donation is therapy; and how the iron-fortified American food supply has shifted the population toward chronic iron overload rather than deficiency.
5. Magnesium: The Silent Epidemic
Why nearly everyone is magnesium-deficient (modern soil, glyphosate, stress, sugar, caffeine, fluoride, vitamin D supplementation), the forms Robbins favors (glycinate, taurate, malate, threonate; not oxide), the “Mag Burn Rate” concept, and topical magnesium oil.
6. The Vitamin D Controversy
Robbins’s most heterodox position: that synthetic D3 supplementation depletes magnesium and retinol, suppresses ceruloplasmin, and drives iron dysregulation — while sunlight and dietary cholesterol-derived D do not. The “steroid hormone, not a vitamin” argument, side-by-side with mainstream endocrinology.
7. Whole-Food Copper Sources
The RCP food list ranked by bioavailable copper: beef liver (3-oz serving = ~14 mg copper, ~700% RDA), oysters, shiitake and crimini mushrooms, cacao and dark chocolate, bee pollen, sesame seeds, and cashews. Weekly targets, sourcing, recipes, and why isolated copper supplements are discouraged.
8. Adrenal Cortisol & Mineral Metabolism
How chronic stress hijacks copper, magnesium, and retinol; why the adrenals require ceruloplasmin to make cortisol; the “Adrenal Cocktail” recipe (orange juice + sea salt + cream of tartar) Robbins teaches; and why “adrenal fatigue” is really a mineral-exhaustion problem.
9. Cure Your Fatigue: The Book
A chapter-by-chapter summary of Robbins’s 2021 book Cure Your Fatigue (Morgan James Publishing): the four-question diagnostic, the iron paradox, the magnesium crisis, the “Stop the Madness” chapter, the protocol layout, the Magnesium Advocacy Group (MAG), where to buy it, and the surrounding ecosystem.
10. Glyphosate, Copper Chelation & the Iron-Overload Cascade
The 1964 chelator patent that predates Roundup’s herbicide use, the log K stability constants for glyphosate–Cu²⁺ (~11.9), pre-harvest desiccation of wheat / oats / pulses, the Eker and Cakmak field studies on plant micronutrient stripping, the Mills 2017 JAMA paper on rising urinary glyphosate, the Motta 2018 PNAS study on bee gut microbiome, the IARC vs. EPA carcinogenicity divide, and the cascade from agricultural residues to copper deficiency to ceruloplasmin failure to iron overload.
Who Is Morley Robbins?
Morley Robbins holds an MA in Health Care Administration and worked as a hospital and physician-practice executive for more than thirty years before retraining as a Certified Health Coach (CHC, Wellcoaches School of Coaching, 2009). His own clinical pivot came when he was diagnosed with frozen shoulder in 2009, did not improve on a conventional inflammatory protocol, and was shown by colleague Dr. David L. Watts (Trace Elements, Inc.) that his hair tissue mineral analysis (HTMA) showed copper deficiency — the opposite of the “copper toxicity” story he had been told. The recovery experience launched the work that became the Root Cause Protocol.
Robbins runs the Magnesium Advocacy Group (MAG), hosts the Cure Your Fatigue podcast, has trained roughly 1,500 RCP Consultants worldwide, and authored Cure Your Fatigue: How Balancing 3 Minerals and 1 Protein Is the Solution You’re Looking For (Morgan James, 2021). His three minerals are copper, magnesium, and retinol-bound iron; his one protein is ceruloplasmin.
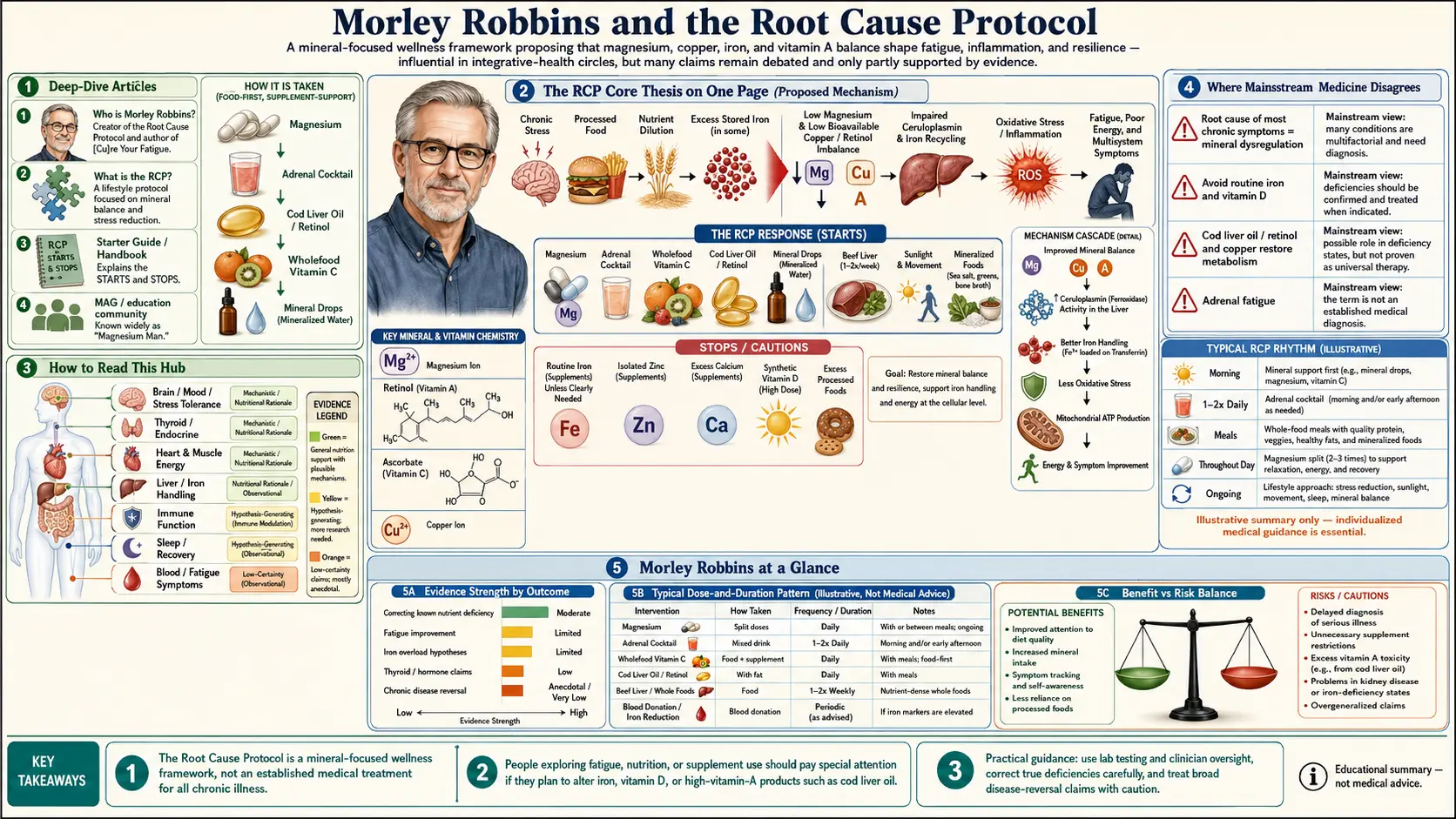
The RCP Core Thesis on One Page
- Iron is not the enemy — unregulated iron is. Iron in tissues that exceeds the binding capacity of transferrin and ferritin generates hydroxyl radicals via the Fenton reaction. Healthy iron biology requires ceruloplasmin’s ferroxidase activity to oxidize Fe²⁺ to Fe³⁺ so it can be loaded onto transferrin.
- Ceruloplasmin requires bioavailable copper, magnesium, and retinol (vitamin A) to be made. A deficiency in any of these proteins/cofactors collapses ferroxidase activity even when total serum copper looks “fine.”
- Modern life depletes all three. Iron-fortified flour, fluoride, glyphosate, refined sugar, caffeine, chronic stress, EMF, ascorbic acid (synthetic vitamin C), high-dose D3 supplementation, and excessive zinc supplementation all reduce ceruloplasmin expression or accelerate magnesium burn.
- Symptoms cluster by mineral pattern, not by disease label. Fatigue, anxiety, “low iron” anemia that doesn’t respond to iron, hypothyroid lab values, hair loss, joint pain, and brain fog often share a copper–magnesium–retinol depletion signature with iron dysregulation.
- The fix is whole food, not isolated supplements. Beef liver, oysters, cacao, bee pollen, real cod-liver oil, whole-food vitamin C (acerola, camu camu), and magnesium glycinate replace synthetic mineral pills. Sunlight replaces D3 capsules.
How to Read This Hub
If you are new to Robbins’s work, start with the Root Cause Protocol overview, then the copper–iron hypothesis page. If you have lab results in hand, jump straight to Ceruloplasmin for the calculation. If you take or have been told to take vitamin D, read The Vitamin D Controversy first — and read it alongside our Vitamin D3 page so you see both sides. For practical change, go to Whole-Food Copper Sources and the Adrenal Cocktail recipe.
Where Mainstream Physiology Already Agrees
- Ceruloplasmin is the major plasma ferroxidase and is essential for loading iron onto transferrin (Hellman & Gitlin, Ann Rev Nutr 2002).
- Aceruloplasminemia — a rare genetic absence of ceruloplasmin — produces iron overload in the brain and pancreas, confirming the copper–iron link in the extreme case.
- Magnesium is required for activation of vitamin D — both 25-hydroxylation and 1α-hydroxylation depend on magnesium-dependent enzymes (Uwitonze & Razzaque, JAOA 2018).
- Iron-mediated oxidative stress via the Fenton reaction is uncontroversial chemistry and a recognized contributor to neurodegeneration.
- Magnesium deficiency is widespread — the U.S. NHANES data put roughly half of Americans below the EAR for magnesium intake.
Where Mainstream Medicine Disagrees
- On vitamin D supplementation. Endocrine Society guidelines and the IOM both recommend cholecalciferol supplementation for deficiency (25-OH-D < 20 ng/mL), and large RCTs (VITAL, D2d) have not shown the harms Robbins describes at typical doses (1,000–4,000 IU/day). Robbins’s critique applies most strongly to high-dose protocols (10,000+ IU/day without magnesium and retinol cofactors).
- On routine iron supplementation. Iron-deficiency anemia in menstruating women, pregnancy, and confirmed low ferritin with low transferrin saturation is treated with oral iron and is well-supported by RCT evidence. Robbins argues many of these “deficiencies” are mislabeled; mainstream hematology disagrees with that broad framing while acknowledging functional iron deficiency exists.
- On ascorbic acid. The bulk of the vitamin C literature uses ascorbic acid; Robbins’s claim that synthetic ascorbic acid is harmful is not supported by mainstream nutritional epidemiology.
The Vitamin D Controversy page lays out both sides with citations. Anyone considering changes to their iron, copper, or vitamin D regimen on the basis of RCP teaching should discuss it with a qualified physician familiar with mineral metabolism.
Connections
- Root Cause Protocol
- Copper-Iron Dysregulation
- Ceruloplasmin and Bioavailable Copper
- Relationship Between Hemoglobin and Ceruloplasmin — why ceruloplasmin (the copper ferroxidase) is required to load iron into hemoglobin, and why "iron-deficiency anemia" is often functional copper deficiency.
- Magnesium Replenishment
- Iron Overload and Hidden Toxicity
- Vitamin D Controversy
- Whole Food Copper Sources
- Adrenal Cortisol and Mineral Connection
- Cure Your Fatigue
- Glyphosate and Copper Chelation
- Copper
- Iron
- Magnesium
- Vitamin A
- Vitamin C
- Vitamin D3
- Vitamin D Test
- Bee Pollen