Kidney Stones
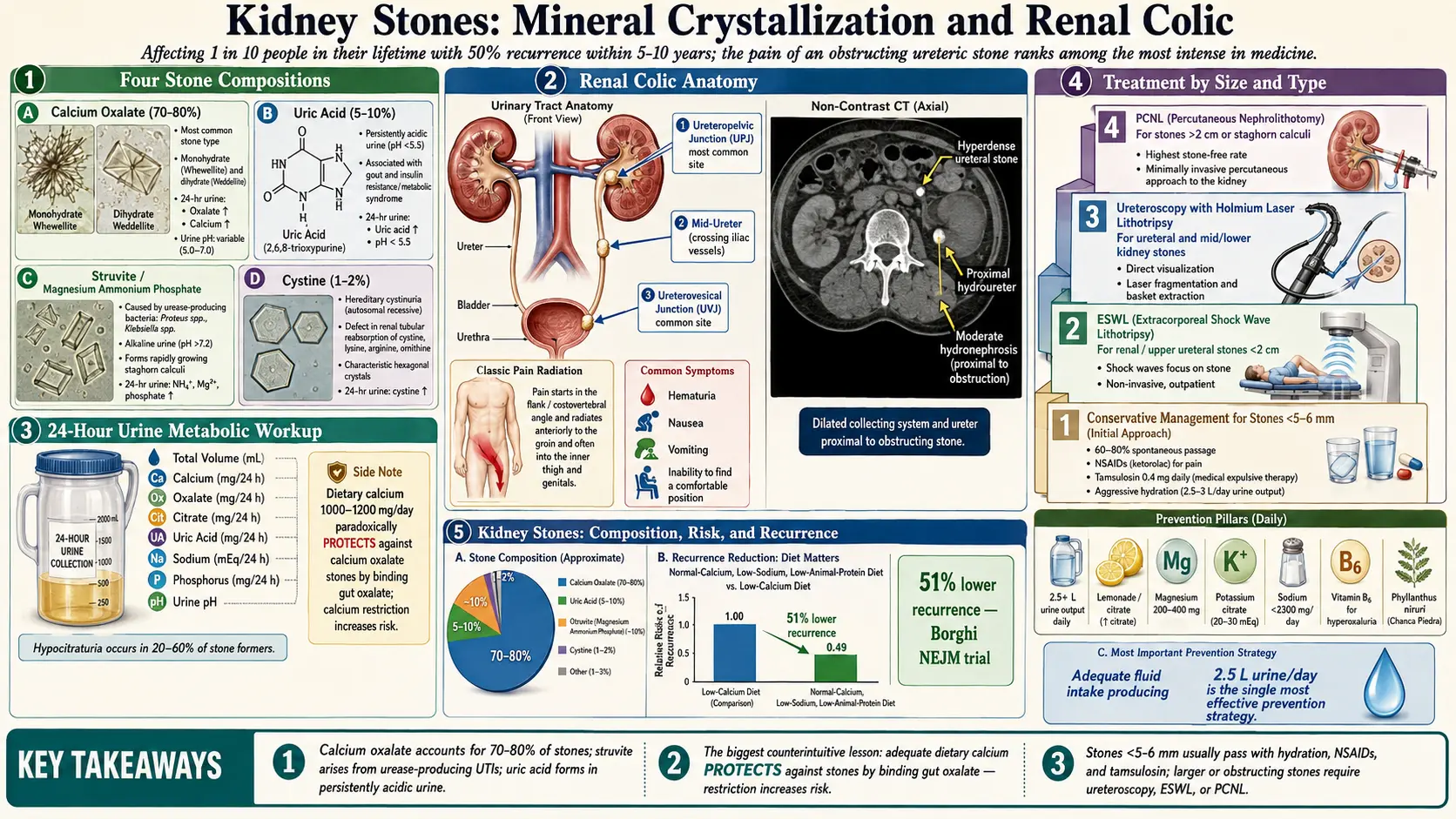
Table of Contents
- Overview
- Types of Kidney Stones
- Causes and Risk Factors
- Symptoms
- Diagnosis
- Conventional Treatment
- Hydration as Prevention
- Natural Prevention Strategies
- Dietary Modifications
- Chanca Piedra (Stone Breaker Herb)
- Apple Cider Vinegar
- Kidney Cleanse Protocols
- Cautions and When to Seek Medical Care
- References & Research
- Research Papers
- Connections
- Featured Videos
Overview
Kidney stones (nephrolithiasis) are hard mineral and salt deposits that form inside the kidneys. They affect approximately 1 in 10 people during their lifetime, and recurrence rates are high, with roughly 50% of stone formers experiencing another episode within five to ten years. The prevalence of kidney stones has been increasing globally, likely due to changes in diet, rising obesity rates, and climate change leading to greater dehydration.
From a naturopathic perspective, kidney stones are largely a condition of metabolic imbalance. Addressing underlying dietary patterns, hydration status, and mineral metabolism can significantly reduce the risk of stone formation and recurrence.
Types of Kidney Stones
Calcium Oxalate Stones
Calcium oxalate stones are the most common type, accounting for approximately 70-80% of all kidney stones. They form when calcium combines with oxalate in the urine. Oxalate is a natural compound found in many foods. Contrary to common belief, restricting dietary calcium actually increases the risk of calcium oxalate stones because calcium in the gut binds oxalate and prevents its absorption.
Uric Acid Stones
Uric acid stones account for about 5-10% of kidney stones. They form when urine is persistently acidic (pH below 5.5). Risk factors include gout, high-purine diets (red meat, organ meats, shellfish), obesity, insulin resistance, and chronic diarrhea. Uric acid stones are unique in that they can sometimes be dissolved by alkalinizing the urine.
Struvite Stones
Struvite stones (magnesium ammonium phosphate) are caused by urinary tract infections with urease-producing bacteria such as Proteus and Klebsiella. These bacteria break down urea into ammonia, which raises urine pH and promotes struvite crystallization. Struvite stones can grow rapidly into large staghorn calculi that fill the renal pelvis and require surgical intervention.
Cystine Stones
Cystine stones are rare, accounting for only 1-2% of kidney stones. They occur in individuals with cystinuria, an inherited genetic disorder that causes excessive excretion of the amino acid cystine in the urine. Cystine stones tend to form at a young age and recur frequently.
Causes and Risk Factors
- Dehydration: The single most important modifiable risk factor. Low urine volume concentrates stone-forming minerals
- Diet: High sodium, high animal protein, and high oxalate diets promote stone formation
- Genetics: Family history of kidney stones significantly increases risk. Cystinuria and primary hyperoxaluria are inherited conditions
- Metabolic conditions: Hyperparathyroidism, renal tubular acidosis, gout, and diabetes all increase stone risk
- Obesity: Associated with insulin resistance, which promotes acidic urine and uric acid stone formation
- Gastrointestinal conditions: Inflammatory bowel disease, gastric bypass surgery, and chronic diarrhea increase oxalate absorption
- Medications: Certain drugs including calcium-based antacids, topiramate, and high-dose vitamin C supplements can contribute to stone formation
- Climate and occupation: Hot climates and occupations involving heat exposure increase dehydration risk
- Sedentary lifestyle: Lack of physical activity may contribute to calcium release from bones
Symptoms
Small kidney stones may pass through the urinary tract without any symptoms. However, when a stone moves into the ureter or obstructs urine flow, it can cause intense pain known as renal colic.
Characteristic Symptoms
- Severe, sharp pain in the flank, side, or lower back that may radiate to the groin and inner thigh. Often described as one of the most intense pains a person can experience
- Pain that comes in waves (colicky), corresponding to ureteral spasm and peristalsis
- Blood in urine (hematuria), which may appear pink, red, or brown
- Nausea and vomiting
- Painful urination (dysuria)
- Urinary urgency and frequency
- Fever and chills (if infection is present, this is a medical emergency)
- Inability to find a comfortable position, with restlessness and constant shifting
Diagnosis
- Non-contrast CT scan: The gold standard for detecting kidney stones, identifying their size, location, and number
- Urinalysis: Reveals blood in urine, crystals, pH, and signs of infection
- Blood tests: Assess kidney function (creatinine, BUN), calcium, uric acid, and parathyroid hormone levels
- 24-hour urine collection: The most valuable test for recurrent stone formers. Measures volume, calcium, oxalate, citrate, uric acid, sodium, phosphorus, and pH to identify specific metabolic abnormalities driving stone formation
- Stone analysis: When a stone is passed or retrieved, laboratory analysis determines its composition and guides targeted prevention
- Ultrasound: A radiation-free alternative, particularly useful in children and pregnant women
Conventional Treatment
Conservative Management
Stones smaller than 5-6 mm often pass spontaneously with supportive care:
- Pain management: NSAIDs (ketorolac, ibuprofen) are first-line. Opioids for severe pain
- Medical expulsive therapy: Alpha-blockers (tamsulosin) relax the ureteral smooth muscle to facilitate stone passage
- Aggressive hydration: IV fluids in acute settings, oral hydration for home management
- Anti-emetics: For nausea and vomiting
Extracorporeal Shock Wave Lithotripsy (ESWL)
ESWL uses focused shock waves from outside the body to fragment kidney stones into smaller pieces that can be passed in the urine. It is most effective for stones under 2 cm located in the kidney or upper ureter. ESWL is non-invasive but may require multiple sessions and has lower success rates for hard stones such as calcium oxalate monohydrate and cystine.
Ureteroscopy
Ureteroscopy involves passing a thin, flexible scope through the urethra and bladder into the ureter to directly visualize and fragment stones, typically using laser lithotripsy (holmium laser). It has high success rates for ureteral stones and mid-to-lower kidney stones. A temporary ureteral stent is often placed afterward.
Percutaneous Nephrolithotomy (PCNL)
For very large stones (over 2 cm) or staghorn calculi, PCNL involves making a small incision in the back and using a nephroscope to directly access and remove stones from the kidney. This is the most invasive option but offers the highest stone-free rates for large stones.
Hydration as Prevention
Adequate hydration is the single most effective strategy for preventing kidney stones of all types. The goal is to produce at least 2.5 liters of urine per day, which typically requires drinking 2.5-3 liters of fluid daily.
- Water should be the primary fluid source
- Urine color is a practical guide: aim for pale yellow to nearly clear
- Increase fluid intake during hot weather, exercise, illness with fever, or diarrhea
- Distribute fluid intake throughout the day, including before bed, to avoid concentrated overnight urine
- Avoid sugar-sweetened beverages: Soda (especially cola) and high-fructose drinks increase stone risk
- Lemonade and other citrus-based drinks increase urinary citrate, a natural stone inhibitor
Natural Prevention Strategies
Lemon Juice and Citrate
Citrate is a potent inhibitor of kidney stone formation. It binds calcium in the urine, reducing the amount available to combine with oxalate. It also directly inhibits calcium oxalate crystal growth and aggregation. Low urinary citrate (hypocitraturia) is found in 20-60% of stone formers.
- Squeeze the juice of 2-3 fresh lemons into 2 liters of water and drink throughout the day
- Lemon juice provides approximately 6-8 grams of citric acid per half cup
- Other citrate sources include lime, orange, and grapefruit juice
Magnesium
Magnesium inhibits calcium oxalate stone formation by binding oxalate in the gut (reducing absorption) and in the urine (reducing crystallization). Many stone formers have suboptimal magnesium intake. Supplementation with 200-400 mg of magnesium citrate or glycinate daily can reduce stone risk. Magnesium-rich foods include pumpkin seeds, dark chocolate, almonds, spinach, and avocados.
Potassium Citrate
Potassium citrate is the standard pharmacological agent for raising urinary citrate and alkalinizing the urine. It is particularly effective for calcium oxalate stones with hypocitraturia and for dissolving or preventing uric acid stones. Natural dietary sources of potassium citrate include fruits (especially citrus, bananas, and avocados) and vegetables.
Vitamin B6 (Pyridoxine)
Vitamin B6 plays a role in oxalate metabolism. It is a cofactor for the enzyme alanine-glyoxylate aminotransferase, which converts glyoxylate to glycine rather than to oxalate. Some studies have shown that vitamin B6 supplementation (25-100 mg daily) can reduce urinary oxalate excretion, particularly in individuals with primary hyperoxaluria or high oxalate production.
Dietary Modifications
Oxalate Management
For calcium oxalate stone formers, moderating (not eliminating) high-oxalate foods can be beneficial:
- Very high oxalate foods to limit: spinach, rhubarb, beets, Swiss chard, nuts (especially almonds and cashews), chocolate, tea, and sweet potatoes
- Cooking (especially boiling) can reduce oxalate content of vegetables by 30-90%
- Pair high-oxalate foods with calcium: Consuming calcium at the same meal binds oxalate in the gut, preventing its absorption and reducing urinary oxalate
- Excessive vitamin C supplementation (over 1000 mg daily) can increase oxalate production
Sodium Reduction
High sodium intake is a significant and often overlooked driver of kidney stone formation. Excess sodium increases urinary calcium excretion (through a shared reabsorption mechanism in the kidney tubule) and decreases citrate excretion.
- Aim for less than 2,300 mg of sodium daily (ideally under 1,500 mg for recurrent stone formers)
- Most dietary sodium comes from processed and restaurant foods, not the salt shaker
- Read nutrition labels carefully and choose low-sodium options
The Adequate Calcium Paradox
One of the most counterintuitive aspects of kidney stone prevention is that adequate dietary calcium actually reduces stone risk. A landmark study in the New England Journal of Medicine demonstrated that men on a normal calcium, low-sodium, low-animal-protein diet had a 51% lower recurrence rate compared to those on a low-calcium diet.
- Aim for 1,000-1,200 mg of calcium daily from food sources
- Dairy, leafy greens, sardines, and fortified foods are good calcium sources
- Calcium supplements, if taken, should be consumed with meals to bind dietary oxalate
- Calcium supplements taken between meals or at bedtime increase urinary calcium without the benefit of oxalate binding
Animal Protein
Excessive animal protein intake promotes stone formation through multiple mechanisms:
- Increases urinary calcium and uric acid excretion
- Decreases urinary citrate
- Lowers urine pH, promoting uric acid stone formation
- Limit animal protein to 0.8-1.0 grams per kilogram of body weight per day
- Incorporate more plant-based protein sources such as legumes and tofu
Chanca Piedra (Stone Breaker Herb)
Chanca Piedra (Phyllanthus niruri) is a tropical plant that has been used for centuries in traditional medicine systems across South America, India, and Southeast Asia for kidney and gallbladder stones. Its common name, "stone breaker," reflects its traditional use.
Mechanisms of Action
- Inhibits crystal formation: Laboratory studies show Chanca Piedra interferes with the nucleation and growth of calcium oxalate crystals
- Relaxes smooth muscle: May help relax the ureter, facilitating passage of small stones
- Increases citrate excretion: Raises urinary citrate, a natural stone inhibitor
- Anti-inflammatory and antioxidant: Reduces kidney tissue damage associated with stone formation
Clinical Evidence
Several clinical trials have shown promising results. A randomized controlled trial found that Chanca Piedra taken after ESWL improved stone clearance rates. Other studies have demonstrated reduced stone size and passage time. However, more large-scale trials are needed.
Dosage
- Tea: 1-2 teaspoons of dried herb steeped in hot water, 2-3 times daily
- Capsules: 500-1000 mg standardized extract, 2-3 times daily
- Tincture: As directed by a qualified herbalist
Apple Cider Vinegar
Apple cider vinegar (ACV) is a popular folk remedy for kidney stones. It contains acetic acid and is claimed to help dissolve stones and prevent new ones from forming.
Proposed Mechanisms
- May increase urinary citrate when metabolized
- Acetic acid may help alkalinize the body and urine over time
- Contains potassium, which can support citrate production
Evidence and Usage
Scientific evidence for ACV in kidney stone treatment is limited, consisting primarily of in vitro studies and anecdotal reports. However, it is generally safe when diluted properly.
- Mix 1-2 tablespoons of raw, unfiltered ACV in a large glass of water
- Drink 1-2 times daily, preferably with meals
- Always dilute: Undiluted ACV can erode tooth enamel and damage esophageal tissue
- Use a straw to minimize contact with teeth
Kidney Cleanse Protocols
From a naturopathic perspective, periodic kidney support can help optimize urinary tract function and reduce stone risk. A kidney cleanse protocol may include:
Hydration Focus
- Increase water intake to 3 liters daily for 1-2 weeks
- Add fresh lemon juice to water throughout the day
- Include herbal kidney-support teas
Supportive Herbs
- Dandelion root (Taraxacum officinale): A gentle diuretic that increases urine output and supports kidney filtration
- Corn silk (Zea mays): A traditional urinary demulcent that soothes the urinary tract lining
- Hydrangea root: Used in traditional herbal medicine as a solvent for calcium deposits
- Goldenrod (Solidago virgaurea): Approved by the German Commission E for urinary tract flushing and stone prevention
- Marshmallow root (Althaea officinalis): A mucilaginous herb that soothes inflamed urinary tissue
Dietary Adjustments During a Cleanse
- Emphasize fruits and vegetables, particularly watermelon, celery, cucumber, and asparagus
- Reduce sodium, processed foods, sugar, and animal protein
- Include magnesium-rich foods daily
- Avoid alcohol and caffeine during the cleanse period
Cautions and When to Seek Medical Care
Kidney stones can be a serious medical condition. Natural approaches are best used for prevention and as complementary support, not as replacements for necessary medical intervention.
- Fever with kidney stone symptoms is a medical emergency indicating possible infected obstructed kidney (pyonephrosis). This requires immediate emergency care
- Complete urinary obstruction can cause permanent kidney damage if not relieved promptly
- Stones larger than 6-7 mm are unlikely to pass spontaneously and typically require intervention
- Uncontrollable pain, nausea, or vomiting warrants emergency evaluation
- Chanca Piedra may interact with blood thinners, diabetes medications, and lithium. Consult a healthcare provider before use
- Herbal diuretics should be used cautiously in individuals with kidney disease, heart failure, or those taking diuretic medications
- Potassium citrate supplementation requires monitoring in individuals with kidney disease or those taking potassium-sparing medications (ACE inhibitors, ARBs, spironolactone)
- Stone analysis is essential for guiding prevention. A strategy effective for calcium oxalate stones may be inappropriate for uric acid or cystine stones
- 24-hour urine testing should be performed in all recurrent stone formers to identify the specific metabolic abnormalities driving stone formation
Working with both a urologist and a naturopathic physician ensures comprehensive stone prevention that addresses the root causes of stone formation while maintaining appropriate medical surveillance.
14. References & Research
Historical Background
Kidney stones have afflicted humans for millennia, with evidence found in a 7,000-year-old Egyptian mummy. Hippocrates described renal colic and stone disease around 400 BCE, and the Hippocratic Oath famously includes a prohibition against "cutting for the stone." The modern era of kidney stone management began with the introduction of extracorporeal shock wave lithotripsy (ESWL) by Christian Chaussy in 1980.
Key Research Papers
- Coe FL, Evan A, Worcester E. Kidney stone disease. Journal of Clinical Investigation. 2005;115(10):2598-2608.
- Zisman AL, Evan AP, Coe FL, Worcester EM. Kidney stones: pathophysiology and medical management. The Lancet. 2015;386(10001):1265-1276.
- Pearle MS, Goldfarb DS, Assimos DG, et al. Medical Management of Kidney Stones: AUA Guideline. Journal of Urology. 2014;192(2):316-324.
- Borghi L, Schianchi T, Meschi T, et al. Comparison of two diets for the prevention of recurrent stones in idiopathic hypercalciuria. New England Journal of Medicine. 2002;346(2):77-84.
- Khan SR, Pearle MS, Robertson WG, et al. Kidney stones. Nature Reviews Disease Primers. 2016;2:16008.
- Turk C, Petrik A, Sarica K, et al. EAU Guidelines on Diagnosis and Conservative Management of Urolithiasis. European Urology. 2016;69(3):468-474.
- Fink HA, Wilt TJ, Eidman KE, et al. Medical Management to Prevent Recurrent Nephrolithiasis in Adults: A Systematic Review for an ACP Clinical Guideline. Annals of Internal Medicine. 2013;158(7):535-543.
- Scales CD Jr, Smith AC, Hanley JM, Saigal CS. Prevalence of kidney stones in the United States. European Urology. 2012;62(1):160-165.
- Stamatelou KK, Francis ME, Jones CA, et al. Time trends in reported prevalence of kidney stones in the United States: 1976-1994. Kidney International. 2003;63(5):1817-1823.
- Assimos D, Krambeck A, Miller NL, et al. Surgical Management of Stones: AUA/Endourological Society Guideline. Journal of Urology. 2016;196(4):1153-1160.
- Curhan GC, Willett WC, Rimm EB, Stampfer MJ. A prospective study of dietary calcium and other nutrients and the risk of symptomatic kidney stones. New England Journal of Medicine. 1993;328(12):833-838.
- Qaseem A, Dallas P, Forciea MA, et al. Dietary and pharmacologic management to prevent recurrent nephrolithiasis in adults: a clinical practice guideline from the American College of Physicians. Annals of Internal Medicine. 2014;161(9):659-667.
Research Papers
- Clinical trials on kidney stone prevention — PubMed search
- Dietary calcium and oxalate stones — PubMed search
- Potassium citrate for stone prevention — PubMed search
- Hydration and kidney stone risk — PubMed search
- Extracorporeal shock wave lithotripsy (ESWL) — PubMed search
- Ureteroscopy for kidney stones — PubMed search
- Chanca piedra (Phyllanthus niruri) for urolithiasis — PubMed search
- DASH diet and kidney stone risk — PubMed search
Connections
- Beans for Kidney Health
- Potassium
- Urinary Tract Infections
- Magnesium
- Chanca Piedra
- Calcium
- Vitamin B6
- Gout
- Hyperparathyroidism
- Uric Acid
- Kidney Disease
- Kidney Function
- Diabetes
- Insulin Resistance
- Urinalysis
- Magnesium Replenishment
- Spinach
- Sickle Cell Disease
- Kidney Cancer
- Polycystic Kidney Disease