Urinary Tract Infections
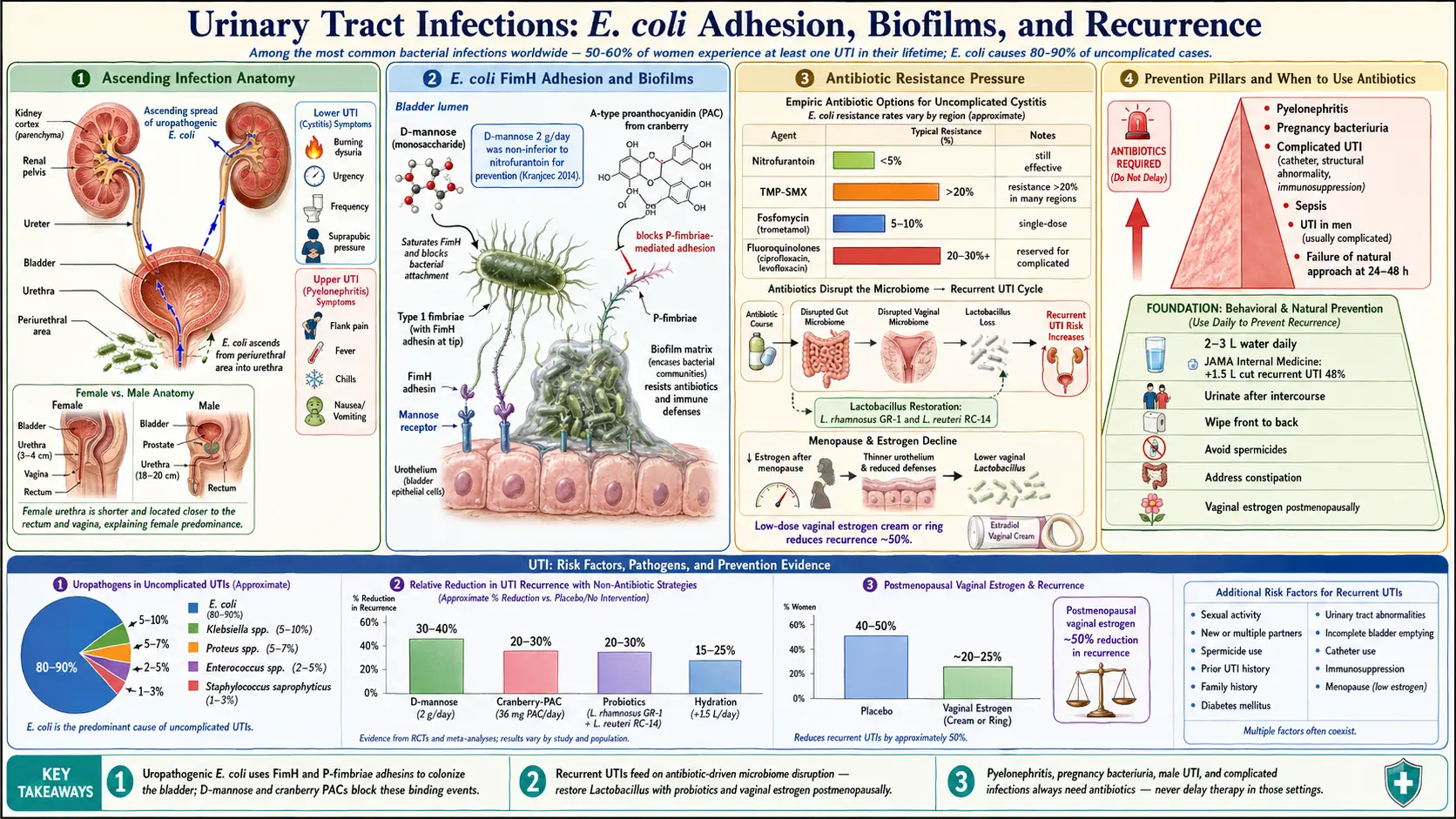
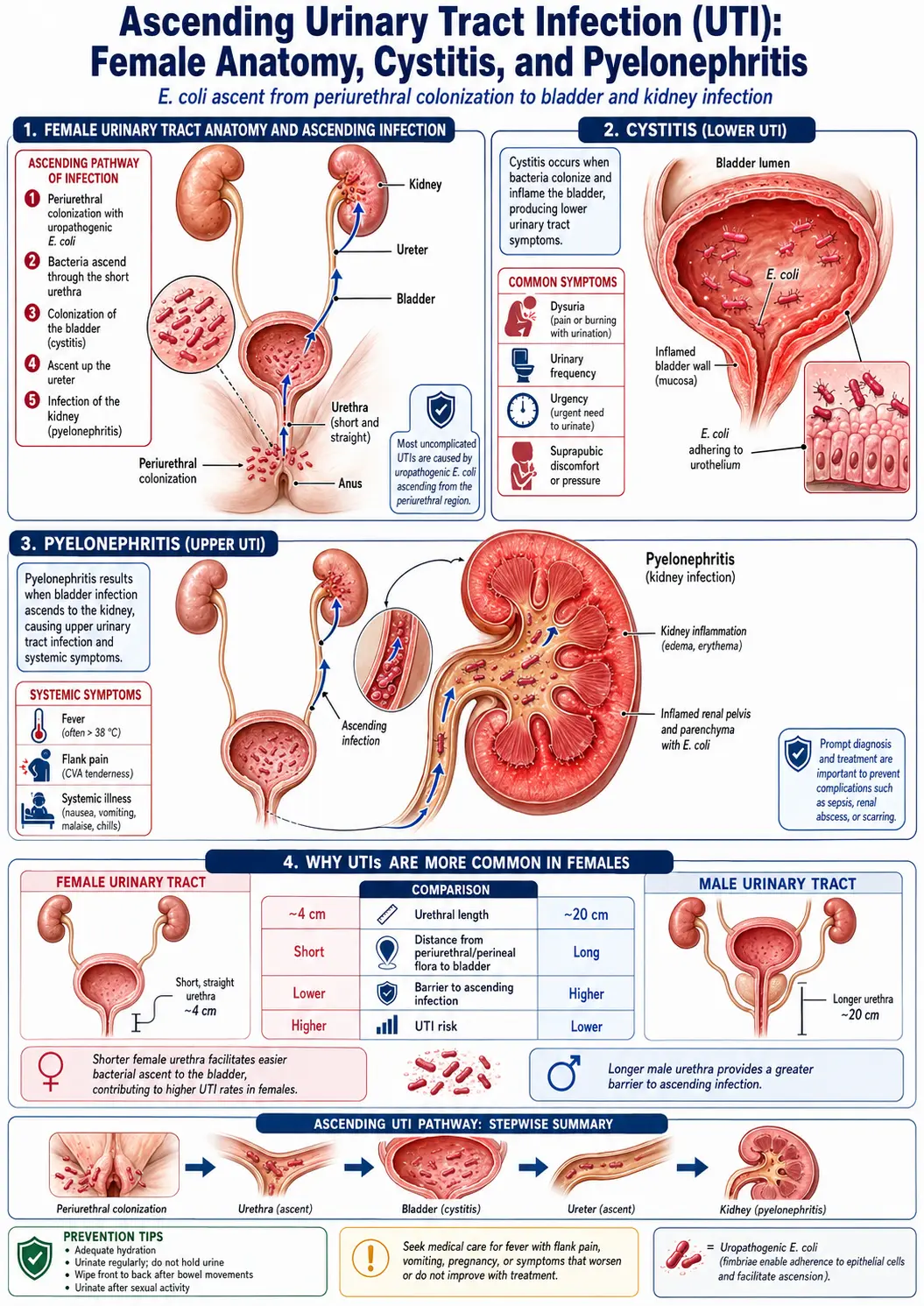
Table of Contents
- What Are Urinary Tract Infections?
- Causes and Pathophysiology
- Risk Factors
- Symptoms
- Conventional Treatment and Antibiotic Resistance
- D-Mannose
- Cranberry and Proanthocyanidins (PACs)
- Herbal Antimicrobials
- Probiotics for Recurrent UTIs
- Hygiene Practices and Prevention
- Hydration and Urinary Health
- Estrogen and Postmenopausal UTIs
- When Antibiotics Are Necessary
- Cautions and Safety Considerations
- References & Research
- Research Papers
- Connections
- Featured Videos
What Are Urinary Tract Infections?
A urinary tract infection (UTI) is an infection that occurs in any part of the urinary system, including the kidneys, ureters, bladder, and urethra. UTIs are among the most common bacterial infections worldwide, accounting for millions of healthcare visits each year. Women are disproportionately affected, with approximately 50-60% of women experiencing at least one UTI in their lifetime.
Types of UTIs
- Cystitis (bladder infection): The most common type, characterized by bladder inflammation, urgency, frequency, and discomfort. Most uncomplicated UTIs fall into this category.
- Pyelonephritis (kidney infection): A more serious upper urinary tract infection that can involve fever, flank pain, nausea, and vomiting. Pyelonephritis requires prompt medical treatment to prevent complications such as sepsis or permanent kidney damage.
- Urethritis: Infection of the urethra, often associated with sexually transmitted organisms.
Causes and Pathophysiology
The vast majority of UTIs are caused by Escherichia coli (E. coli), a bacterium that normally resides in the intestinal tract. E. coli accounts for approximately 80-90% of uncomplicated UTIs. Other causative organisms include Klebsiella, Proteus, Enterococcus, and Staphylococcus saprophyticus.
Bacterial Biofilms
One of the reasons UTIs frequently recur is the formation of bacterial biofilms. These are structured communities of bacteria that adhere to the bladder wall and encase themselves in a protective matrix. Biofilms are highly resistant to both antibiotics and immune defenses. Uropathogenic E. coli can also invade bladder epithelial cells and form intracellular bacterial communities that persist as reservoirs for future infections.
From a naturopathic perspective, addressing biofilm formation is a critical aspect of managing recurrent UTIs. Agents such as N-acetylcysteine (NAC), lactoferrin, and certain enzymes may help disrupt biofilm structures.
Risk Factors
- Female anatomy: Women have a shorter urethra, placing the bladder closer to sources of bacteria from the rectum and vagina
- Sexual activity: Intercourse can introduce bacteria into the urinary tract. New sexual partners increase risk
- Menopause: Declining estrogen levels lead to changes in vaginal flora and thinning of urethral tissue, increasing susceptibility
- Catheter use: Indwelling urinary catheters are a major risk factor for hospital-acquired UTIs
- Urinary retention: Incomplete bladder emptying allows bacteria to multiply
- Diabetes: Elevated blood sugar impairs immune function and promotes bacterial growth
- Spermicide use: Disrupts normal vaginal flora and increases UTI risk
- History of previous UTIs: The strongest predictor of future UTIs
- Constipation: Particularly in children, constipation can impair bladder emptying and promote bacterial colonization
- Immunosuppression: Any condition or medication that weakens immune defenses
Symptoms
Lower UTI (Cystitis) Symptoms
- Burning or pain during urination (dysuria)
- Increased urinary frequency and urgency
- Cloudy, dark, or strong-smelling urine
- Blood in urine (hematuria)
- Pelvic pressure or lower abdominal discomfort
- Low-grade fever (sometimes)
Upper UTI (Pyelonephritis) Symptoms
- High fever and chills
- Flank pain (pain in the side or back, below the ribs)
- Nausea and vomiting
- All symptoms of lower UTI may also be present
Conventional Treatment and Antibiotic Resistance
Conventional treatment for uncomplicated UTIs typically involves a short course of antibiotics. Common first-line options include nitrofurantoin, trimethoprim-sulfamethoxazole (TMP-SMX), and fosfomycin. Fluoroquinolones are reserved for complicated infections due to their side-effect profile.
The Antibiotic Resistance Crisis
Antibiotic resistance in uropathogens is a growing global concern. Resistance rates to TMP-SMX exceed 20% in many regions, and multi-drug-resistant E. coli strains are increasingly common. Each course of antibiotics also disrupts the gut and vaginal microbiome, which paradoxically increases vulnerability to future UTIs.
This cycle of recurrent infection and repeated antibiotic use underscores the importance of prevention-focused strategies and evidence-based natural alternatives that can reduce reliance on antibiotics without compromising patient safety.
D-Mannose
D-mannose is a naturally occurring simple sugar closely related to glucose. It is one of the most promising natural agents for UTI prevention and acute treatment support.
How D-Mannose Works
Uropathogenic E. coli use type 1 fimbriae (pili) tipped with FimH adhesins to attach to mannose receptors on bladder epithelial cells. D-mannose acts as a competitive inhibitor by saturating these bacterial adhesins, preventing E. coli from binding to the bladder wall. The bacteria are then flushed out during urination.
Clinical Evidence
A landmark randomized controlled trial published in the World Journal of Urology found that 2 grams of D-mannose daily was as effective as the antibiotic nitrofurantoin in preventing recurrent UTIs over a six-month period, with significantly fewer side effects.
Dosage
- Prevention: 1-2 grams daily
- Acute infection support: 1.5-3 grams every 2-3 hours for 48-72 hours, then taper
- Available in powder or capsule form. Powder dissolved in water is generally preferred for faster absorption
Cranberry and Proanthocyanidins (PACs)
Cranberry has been used for urinary health for centuries. Its benefits come primarily from A-type proanthocyanidins (PACs), which prevent E. coli from adhering to bladder and kidney cells via a different mechanism than D-mannose, targeting P-fimbriae.
Choosing Effective Cranberry Products
- Not all cranberry products are equally effective. The key is PAC content
- A minimum of 36 mg of PACs daily is needed for clinical benefit
- Cranberry capsules or concentrated extracts standardized to PAC content are more reliable than juice
- Cranberry juice cocktails contain excessive sugar and insufficient PACs
- Cranberry works best as a preventive strategy rather than treatment for active infection
Herbal Antimicrobials
Uva Ursi (Arctostaphylos uva-ursi)
Uva ursi, also known as bearberry, contains the active compound arbutin, which is converted to hydroquinone in the urinary tract. Hydroquinone has antimicrobial activity against common uropathogens. Uva ursi is most effective when urine pH is alkaline (above 7), so it is often taken with alkalinizing agents such as sodium bicarbonate. It should be used short-term only (5-7 days) due to potential liver toxicity with prolonged use.
Oregano Oil
Oregano oil contains carvacrol and thymol, potent antimicrobial compounds active against E. coli and other uropathogens, including antibiotic-resistant strains. Emulsified oregano oil capsules (150-200 mg standardized to carvacrol content, taken 2-3 times daily with meals) may be used as part of a comprehensive protocol for acute UTI support. It should not replace antibiotics when they are medically indicated.
Garlic (Allium sativum)
Garlic contains allicin, a sulfur compound with broad-spectrum antimicrobial properties. Research has demonstrated activity against multi-drug-resistant uropathogens, including extended-spectrum beta-lactamase (ESBL)-producing E. coli. Fresh garlic or stabilized allicin supplements can be incorporated into a UTI prevention and treatment protocol.
Probiotics for Recurrent UTIs
The vaginal and urinary microbiome plays a crucial role in defense against UTIs. A healthy vaginal flora dominated by Lactobacillus species creates an acidic environment (pH 3.5-4.5) that inhibits pathogenic bacterial growth.
Key Probiotic Strains
- Lactobacillus rhamnosus GR-1 and Lactobacillus reuteri RC-14: The most clinically studied strains for urogenital health. They colonize the vaginal tract and produce hydrogen peroxide, bacteriocins, and biosurfactants that inhibit uropathogens
- Lactobacillus crispatus: The dominant species in a healthy vaginal microbiome. Supplementation may help restore protective flora
Administration
- Oral probiotics containing GR-1 and RC-14 have been shown to migrate from the gut to the vaginal tract
- Vaginal probiotic suppositories offer direct colonization of the urogenital area
- Probiotics are especially important during and after antibiotic therapy to restore microbiome balance
Hygiene Practices and Prevention
- Wipe front to back after using the toilet to prevent fecal bacteria from reaching the urethra
- Urinate after sexual intercourse to flush bacteria that may have been introduced
- Avoid spermicides and diaphragms if prone to recurrent UTIs
- Wear breathable cotton underwear and avoid prolonged use of tight-fitting clothing
- Avoid douching and scented feminine hygiene products, which disrupt vaginal flora
- Do not hold urine for prolonged periods. Void regularly to flush bacteria
- Address constipation, which can contribute to incomplete bladder emptying and bacterial overgrowth
Hydration and Urinary Health
Adequate hydration is one of the simplest and most effective strategies for UTI prevention. Increased fluid intake promotes frequent urination, which physically flushes bacteria from the urinary tract before they can establish infection.
- Aim for 2-3 liters of water daily, adjusting for activity level and climate
- A randomized controlled trial published in JAMA Internal Medicine found that women who increased water intake by 1.5 liters per day had 48% fewer recurrent UTIs compared to the control group
- Herbal teas such as corn silk, marshmallow root, and parsley have traditional use as urinary demulcents and mild diuretics
- Minimize bladder irritants including caffeine, alcohol, carbonated beverages, and artificial sweeteners
Estrogen and Postmenopausal UTIs
Postmenopausal women experience a significant increase in UTI frequency due to declining estrogen levels. Estrogen plays a critical role in maintaining the health of the vaginal and urethral epithelium and supporting colonization by protective Lactobacillus species.
Vaginal Estrogen Therapy
Low-dose vaginal estrogen (cream, ring, or tablet) has been shown to reduce recurrent UTIs in postmenopausal women by up to 50%. Vaginal estrogen restores the vaginal epithelium, lowers vaginal pH, and promotes Lactobacillus recolonization. Vaginal estrogen therapy carries minimal systemic absorption and is generally considered safe even in women with contraindications to systemic hormone therapy.
Natural Alternatives
- Vaginal DHEA: Converts locally to estrogen and testosterone, supporting vaginal tissue health
- Sea buckthorn oil: Contains omega-7 fatty acids that may improve mucosal membrane integrity
- Vitamin E suppositories: Can help maintain vaginal tissue moisture and elasticity
When Antibiotics Are Necessary
While natural approaches are valuable for prevention and support of mild UTIs, antibiotics remain essential in certain situations:
- Pyelonephritis (kidney infection): Always requires antibiotic treatment to prevent serious complications
- UTIs during pregnancy: Even asymptomatic bacteriuria should be treated to prevent preterm labor and pyelonephritis
- Complicated UTIs: Infections in patients with structural abnormalities, catheters, or immunosuppression
- Sepsis or systemic infection: Medical emergency requiring immediate antibiotic therapy
- Symptoms worsening despite natural treatment after 24-48 hours
- UTIs in men: Generally considered complicated and typically warrant antibiotic treatment
Cautions and Safety Considerations
- Do not delay appropriate medical care for a worsening UTI. Untreated kidney infections can lead to sepsis, which is life-threatening
- Uva ursi should not be used for more than one week at a time, during pregnancy, or in children
- Cranberry may interact with warfarin and other blood thinners
- D-mannose is generally very safe but should be used cautiously in individuals with diabetes, as it may affect blood sugar in high doses
- Oregano oil can irritate the gastrointestinal tract. Always use emulsified or enteric-coated formulations and take with food
- High-dose vitamin C (sometimes recommended to acidify urine) can increase oxalate levels and kidney stone risk in susceptible individuals
- Children, pregnant women, and immunocompromised patients with suspected UTIs should always be evaluated by a healthcare provider
- Self-diagnosis can be unreliable. UTI symptoms can overlap with sexually transmitted infections, interstitial cystitis, or other conditions. Urinalysis and culture confirm diagnosis
An integrative approach that combines evidence-based natural prevention with appropriate use of conventional treatment when necessary offers the best outcomes for urinary tract health.
15. References & Research
Historical Background
Urinary tract infections have been recognized since ancient times, with descriptions of urinary symptoms found in Egyptian papyri. The bacterial cause of UTIs was established in the late 19th century with the work of Theodor Escherich, who first described Escherichia coli in 1885. The development of sulfonamides in the 1930s and subsequent antibiotics revolutionized UTI treatment.
Key Research Papers
- Foxman B. Urinary tract infection syndromes: occurrence, recurrence, bacteriology, risk factors, and disease burden. Infectious Disease Clinics of North America. 2014;28(1):1-13.
- Hooton TM. Uncomplicated urinary tract infection. New England Journal of Medicine. 2012;366(11):1028-1037.
- Hooton TM, Vecchio M, Iroz A, et al. Effect of increased daily water intake in premenopausal women with recurrent urinary tract infections: a randomized clinical trial. JAMA Internal Medicine. 2018;178(11):1509-1515.
- Kranjcec B, Papes D, Altarac S. D-mannose powder for prophylaxis of recurrent urinary tract infections in women: a randomized clinical trial. World Journal of Urology. 2014;32(1):79-84.
- Gupta K, Hooton TM, Naber KG, et al. International Clinical Practice Guidelines for the Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Women (IDSA/ESCMID Guidelines). Clinical Infectious Diseases. 2011;52(5):e103-e120.
- Jepson RG, Williams G, Craig JC. Cranberries for preventing urinary tract infections. Cochrane Database of Systematic Reviews. 2012;10:CD001321.
- Stamm WE, Norrby SR. Urinary tract infections: disease panorama and challenges. Journal of Infectious Diseases. 2001;183(Suppl 1):S1-S4.
- Flores-Mireles AL, Walker JN, Caparon M, Hultgren SJ. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nature Reviews Microbiology. 2015;13(5):269-284.
- Beerepoot MA, ter Riet G, Nys S, et al. Lactobacilli vs antibiotics to prevent urinary tract infections: a randomized, double-blind, noninferiority trial in postmenopausal women. Archives of Internal Medicine. 2012;172(9):704-712.
- Naber KG, Schito G, Botto H, et al. Surveillance study in Europe and Brazil on clinical aspects and antimicrobial resistance epidemiology in females with cystitis (ARESC). European Urology. 2008;54(5):1164-1175.
- Anger J, Lee U, Ackerman AL, et al. Recurrent Uncomplicated Urinary Tract Infections in Women: AUA/CUA/SUFU Guideline. Journal of Urology. 2019;202(2):282-289.
- Raz R, Stamm WE. A controlled trial of intravaginal estriol in postmenopausal women with recurrent urinary tract infections. New England Journal of Medicine. 1993;329(11):753-756.
Research Papers
- Clinical trials on urinary tract infection treatment — PubMed search
- D-mannose for UTI prevention — PubMed search
- Cranberry and proanthocyanidins for UTI — PubMed search
- Recurrent UTI prophylaxis in women — PubMed search
- Vaginal estrogen for postmenopausal UTI — PubMed search
- Probiotics (Lactobacillus) for UTI prevention — PubMed search
- Antibiotic resistance in E. coli UTI — PubMed search
- Increased hydration and UTI recurrence — PubMed search
Connections
- Pyelonephritis (Kidney Infection)
- Interstitial Cystitis
- Probiotics
- E. Coli
- Vitamin C
- Kidney Stones
- Bladder Cancer
- Goldenseal
- Sepsis
- Oregano
- Garlic
- Urinalysis
- Diabetes
- Benign Prostatic Hyperplasia
- Prostate Conditions
- Artificial Sweeteners
- Irritable Bowel Syndrome
- Eucalyptus
- Andrographis
- Prostate Cancer
- Bacterial Vaginosis
- Yeast Infections
- Urinary Incontinence