Can You Reverse Coronary Calcium? Plaque Stabilization vs Reversal

The honest answer to "can I reverse my coronary calcium" is unsatisfying: calcium volume is rarely reduced, but plaque stabilization and event reduction are very achievable. The interventions that have most reliably reduced cardiovascular events — statins, plant-predominant diets, exercise, smoking cessation, blood-pressure control — tend to increase calcium density on follow-up CAC scans even as they slash event rates. The right framing is not "can I reverse my CAC" but "can I prevent the cardiovascular event that the CAC predicts." This page covers what the evidence actually shows about plaque modification, the famous diet-and-lifestyle studies (Esselstyn, Ornish, Pritikin), exercise data, and the realistic best-case lifestyle outcome.
Table of Contents
- Calcium Volume vs Total Plaque Burden
- What Plaque Stabilization Means
- Statins and the Density Increase
- Esselstyn Plant-Based Diet Study
- Ornish Lifestyle Heart Trial
- Pritikin Program Data
- Exercise Effects on Plaque
- The Combined Lifestyle Stack
- Realistic Best-Case Outcome
- Research Papers and References
- Connections
- Featured Videos
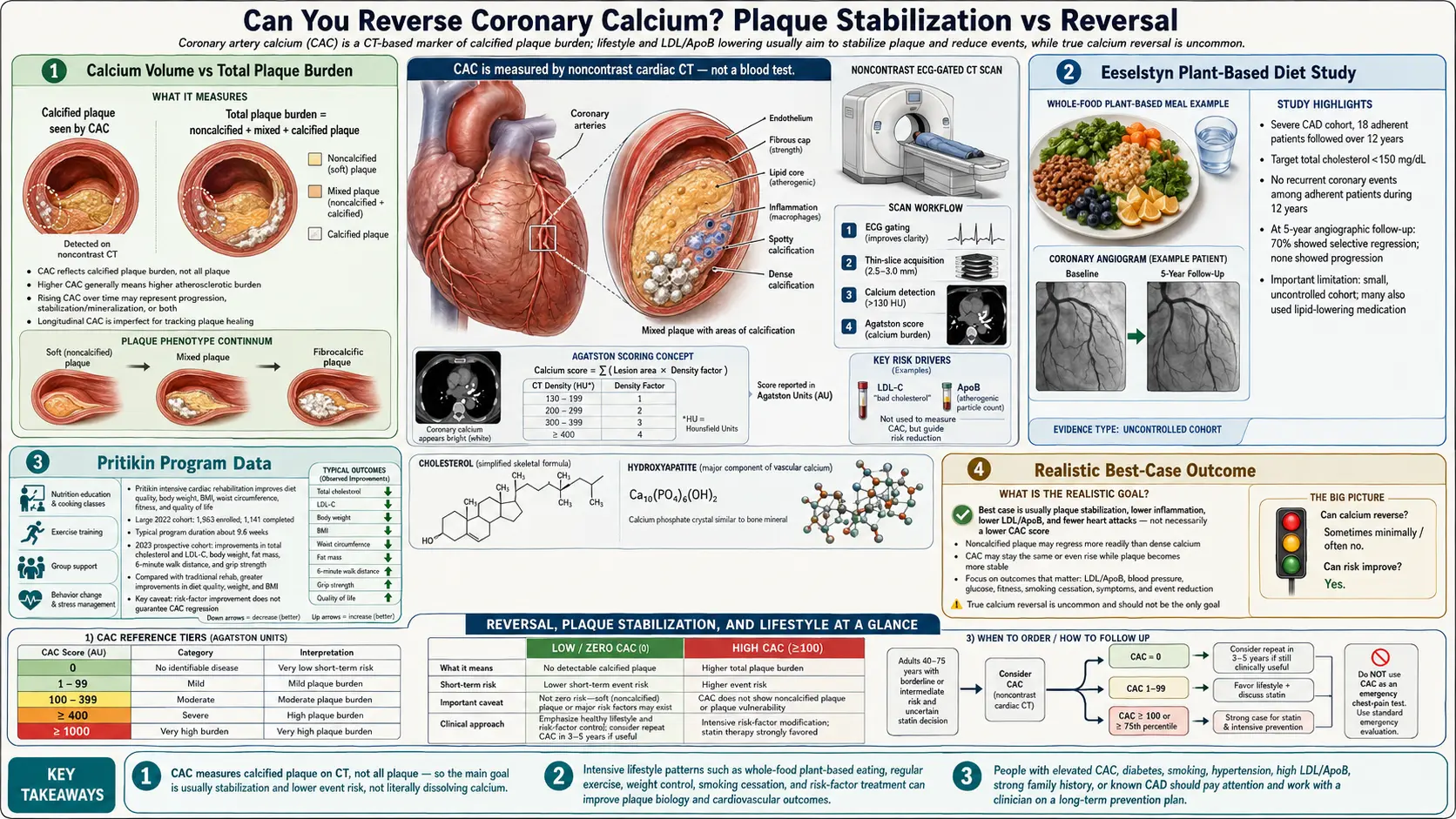
Calcium Volume vs Total Plaque Burden
Coronary calcium and total atherosclerotic plaque are related but not identical:
- Calcium volume — the mineralized portion; visible on non-contrast CT
- Soft plaque — lipid core, fibrous cap, macrophage infiltrate; visible on CCTA, not on CAC
- Total plaque burden — sum of all plaque types
Lifestyle and pharmacologic interventions can:
- Reduce soft plaque volume (regression of the lipid-rich component)
- Stabilize remaining plaque (denser fibrous cap, less inflammatory infiltrate)
- Increase calcium density as part of stabilization (calcium is deposited in the residual stable plaque)
- Result in an Agatston score that is the same or slightly higher even though total plaque burden has decreased and event risk has dropped substantially
This is why a follow-up CAC after years of intensive lifestyle change can be confusingly "no better." The Agatston score isn't the right metric for tracking lifestyle response — clinical event rates and lipid markers are.
What Plaque Stabilization Means
A "stable" atherosclerotic plaque has features that make it less likely to rupture and cause an acute coronary event:
- Thick fibrous cap (>65 µm) — resists mechanical and inflammatory stress
- Smaller lipid core — less mass to spill if the cap ruptures
- Reduced macrophage infiltrate — less protease activity weakening the cap
- Higher smooth-muscle-cell content — structural stability
- More dense calcification — physical reinforcement
- Less neovascularization — fewer fragile new vessels prone to intraplaque hemorrhage
Plaque rupture, not stenosis severity, is what causes most heart attacks. Two patients with identical 50% stenoses can have very different event risks depending on plaque stability. Stable plaque is the goal; calcium volume is a side-effect of stability rather than a driver of it.
Statins and the Density Increase
Multiple randomized trials and longitudinal studies have shown that patients on statins have higher calcium scores at follow-up than statin-naïve controls, despite lower clinical event rates. Mechanistic studies show statins:
- Reduce LDL-C and lipid accumulation in plaque
- Reduce inflammatory drive (decrease oxidized LDL, decrease macrophage activity)
- Promote fibrous-cap thickening
- Promote intra-plaque calcification as part of fibrocalcific stabilization
- Result in 10–20% per year average increase in Agatston score
This is the clearest example in cardiovascular medicine of an effective intervention producing a "worse-looking" surrogate marker. The lesson: don't track Agatston score on serial scans as a treatment-response metric. Track LDL-C/ApoB, blood pressure, A1c, and clinical events instead. See the Statin Threshold page.
Esselstyn Plant-Based Diet Study
Caldwell Esselstyn at the Cleveland Clinic published a long-term observational study of 198 patients with established cardiovascular disease who adopted a strict whole-food plant-based diet (low-fat, no added oils, no animal products, minimal nuts/avocados). Reported findings:
- Among the 177 adherent patients, 0.6% had an event over 3.7 years of follow-up
- Among the 21 non-adherent patients, 62% had events
- Some patients had angiographic regression of stenoses
- Calcium scores were not the primary tracked endpoint; lipid and event outcomes were
The Esselstyn study is observational, not randomized, and the patient cohort is highly self-selected for motivation. Its limitations as evidence are real. But the magnitude of the reported event-rate difference is striking, and the underlying biology — LDL-C in the 70–80 mg/dL range achievable on this diet — aligns with what statin trials show at similar LDL endpoints. The diet is hard to sustain; about 70% of patients in the cohort were able to adhere long-term, which is consistent with other intensive-diet studies.
Ornish Lifestyle Heart Trial
Dean Ornish's Lifestyle Heart Trial (1990, Lancet) randomized 48 patients with documented CAD to either an experimental intensive-lifestyle group (low-fat plant-based diet + meditation + group support + moderate aerobic exercise + smoking cessation) or a usual-care control group. Five-year findings:
- Quantitative coronary angiography showed regression of stenosis in the experimental group, progression in controls
- Mean coronary stenosis decreased 7.9% relative in experimental vs increased 27.8% in controls
- Cardiac event rates were lower in the experimental group
- The lifestyle program was Medicare-approved as cardiac rehabilitation in 2010 (CMS code G0422/G0423)
Like Esselstyn, the Ornish program is highly intensive and difficult to sustain. The integrated approach — diet, stress management, exercise, social support — may be why effects are stronger than diet alone in some studies.
Pritikin Program Data
The Pritikin Program (started 1976 by Nathan Pritikin) emphasized a high-fiber, low-fat, predominantly plant-based diet with daily exercise. Multiple studies have shown:
- LDL-C reductions of 20–30% within weeks of intensive program participation
- Blood pressure reductions of 10–15 mmHg systolic
- Improvements in HbA1c, weight, exercise capacity
- Reduced angina frequency in patients with established CAD
The Pritikin approach has been extended into other intensive lifestyle programs (e.g., the CHIP/CHIP-style programs). The pattern is consistent: substantial dietary change combined with structured exercise produces measurable cardiovascular benefits, though sustainability is the challenge.
Exercise Effects on Plaque
Exercise has a more complex relationship with CAC than people often assume:
- Master endurance athletes — multiple studies show that long-term, high-volume endurance athletes (marathon runners, cyclists) have higher CAC scores than sedentary controls, by some estimates 1.5–2× higher
- But event rates are lower — the same athletes have substantially lower cardiovascular event rates despite higher calcium scores
- Plaque morphology differs — the calcified plaque in athletes is more dense, more stable, less lipid-rich
This appears to be another example of the density-stabilization-without-volume-change pattern. The "athlete's CAC paradox" reinforces the point that absolute Agatston score can be misleading without context.
Practical guidance:
- Regular moderate-to-vigorous exercise (150 min/week minimum) is unambiguously protective
- Extreme endurance training does not appear to harm cardiovascular outcomes despite higher CAC; if anything, outcomes are better
- For most patients, the absolute event-risk reduction from regular exercise is substantial regardless of what happens to calcium volume
The Combined Lifestyle Stack
The interventions with the strongest combined evidence for cardiovascular event reduction:
- Mediterranean or plant-predominant diet (PREDIMED demonstrated 30% relative reduction in CV events with extra-virgin olive oil + nuts vs control)
- 150–300 minutes/week moderate-intensity exercise
- Smoking cessation (single largest modifiable factor)
- Blood pressure control (target <130/80)
- LDL-C / ApoB reduction (statin if appropriate; lifestyle alone often insufficient at moderate-high CAC)
- HbA1c control if diabetic
- Weight management (especially visceral adiposity)
- Sleep optimization (7–9 hours; treat sleep apnea)
- Stress management (meditation, social connection, structured stress-reduction)
- Moderate alcohol or none
- Air-quality awareness (PM2.5 reduction in heavy-pollution environments)
The cumulative effect of doing 6–8 of these well is large — comparable to or exceeding pharmacologic interventions in many studies. The cardiovascular benefits compound; doing all of them imperfectly outperforms doing one of them perfectly.
Realistic Best-Case Outcome
For someone with elevated CAC who adopts a comprehensive lifestyle stack:
- Soft plaque burden may regress over years (visible on serial CCTA, not CAC)
- Calcium density increases on serial CAC, reflecting stabilization
- Total Agatston score may rise modestly — do not interpret as failure
- Clinical event rate drops substantially — the actual goal
- Quality of life and functional capacity improve — secondary benefits
- Lifespan extension on the order of years — achievable in motivated patients
The mental reframe: calcium reversal is not the goal; not having a heart attack is the goal. Lifestyle measures, medications, and CAC scoring all serve that goal. The number on the report is a tool, not the target.
Research Papers and References
- Esselstyn plant-based diet study — PubMed search
- Ornish Lifestyle Heart Trial — PubMed search
- PREDIMED Mediterranean diet trial — PubMed search
- Master athlete CAC paradox — PubMed search
- Plaque stabilization with statins — PubMed search
- Lifestyle interventions and CV events — PubMed search
- Pritikin program data — PubMed search
Connections
- Coronary Calcium Score
- Statin Threshold and CAC
- Soft Plaque and CAC Limitations
- CAC vs Other Cardiac Tests
- Agatston Score Calculation and Interpretation
- CAC Zero and the Power of Negative Result
- CAC in Women and Younger Adults
- MESA Risk Calculator and Age Percentiles
- ApoB
- Lipoprotein(a)
- Anti-Inflammatory Diet
- Longevity Protocols
- Blood Sugar
- Stress Management
- Omega-3 Fatty Acids
- Nattokinase
- Gerson Therapy
- Calcium