Polysorbate 80: The Emulsifier Destroying Your Gut Barrier
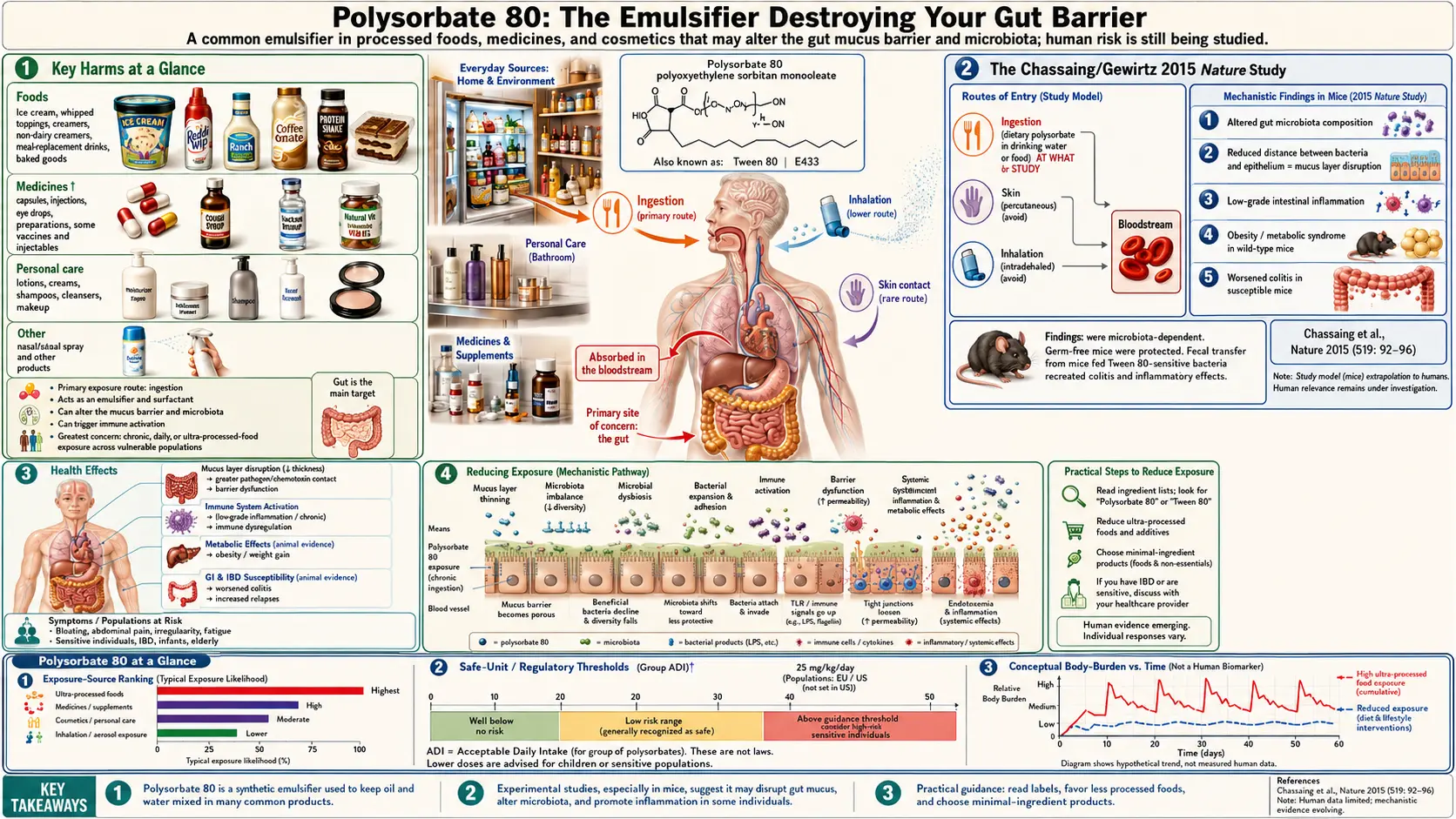
Table of Contents
- Key Harms at a Glance
- Overview
- Sources
- The Chassaing/Gewirtz 2015 Nature Study
- Mechanism of Toxicity
- Health Effects
- The Human Trial
- Regulatory Status
- Reducing Exposure
- Research Papers and References
- Connections
- Featured Videos
Key Harms at a Glance
- Erodes the protective gut mucus layer — demonstrated in mice at concentrations below FDA-permitted limits (Chassaing et al., Nature 2015).
- Promotes colitis — accelerates inflammatory bowel disease in genetically susceptible mouse models.
- Metabolic syndrome — drives adiposity, glucose intolerance, and insulin resistance in animal studies.
- Microbiome dysbiosis — shifts gut communities toward pro-inflammatory flagellated species.
- Human RCT confirmation (2022) — dietary-level exposure alters microbiome and raises gut inflammation in healthy volunteers.
- Potential colon-cancer promotion — chronic inflammation-driven tumor-promoting environment.
- Dual-route exposure — food additive and pharmaceutical excipient, creating additive daily dose.
Overview
Polysorbate 80, chemically named polyoxyethylene (20) sorbitan monooleate, is listed as E433 in the European Union and is widely known in pharmaceutical and laboratory contexts by its trade name Tween 80. It is a synthetic emulsifier produced by reacting sorbitol with ethylene oxide and oleic acid — a fully industrial process yielding a compound with no natural dietary precedent.
The "80" in polysorbate 80 refers to the fatty acid component (oleic acid, an 18-carbon monounsaturated fat), while the "20" in its chemical name indicates the average number of oxyethylene units in the polyoxyethylene chain. This amphiphilic (simultaneously water- and fat-loving) molecular structure is what makes it an effective emulsifier: the oleic acid tail dissolves in fat droplets while the polyoxyethylene chains extend into the surrounding water phase, stabilizing the interface and preventing oil-water separation.
Beyond food manufacturing, polysorbate 80 has a well-established role as a pharmaceutical excipient, used to solubilize poorly water-soluble drugs and to stabilize protein biologics and injectable formulations. This dual role — food additive and pharmaceutical excipient — means that polysorbate 80 exposure occurs through multiple routes simultaneously for many people.
Sources
Polysorbate 80 is found in a wide array of processed foods, most commonly products where oil and water must be kept uniformly mixed:
- Ice cream — the most common and highest-exposure food source; polysorbate 80 is used alongside polysorbate 65 to improve texture, allow slower melting, and create a smoother mouthfeel by controlling fat crystallization and emulsification during freezing
- Salad dressings — particularly creamy dressings (ranch, caesar, thousand island) where stable emulsification of oil and aqueous components is essential
- Sauces and condiments — mayonnaise-based sauces, pasta sauces, and gravies may use polysorbate 80 for emulsion stability during storage
- Baked goods — used as a dough conditioner and to improve the emulsification of fat into batter, resulting in softer texture and extended shelf life in commercial cakes, muffins, and breads
- Whipped toppings — non-dairy whipped cream products depend on emulsifiers including polysorbate 80 to form and stabilize the fat foam structure
- Shortening — commercial shortenings for baking applications frequently contain polysorbate 80 to improve their emulsifying performance in batter systems
- Chewing gum — included in the gum base as a plasticizer and emulsifier
- Gelatin desserts and puddings — used to prevent fat bloom and maintain uniform texture
- Medications — polysorbate 80 is a common excipient in oral and injectable drug formulations, serving as a solubilizing and wetting agent
The cumulative daily exposure from food alone can be substantial for individuals consuming multiple processed food products, and this is additive with pharmaceutical exposures.
The Chassaing/Gewirtz 2015 Nature Study
The scientific understanding of dietary emulsifiers as a class of gut-disrupting agents was transformed by a landmark 2015 paper published in Nature by Benoit Chassaing, Andrew Gewirtz, and colleagues at Georgia State University. The study examined polysorbate 80 (P80) and carboxymethylcellulose (CMC) — two of the most widely used food emulsifiers — in mouse models using concentrations intended to approximate human dietary exposure.
The key findings were striking and unexpected in their magnitude:
- Mice consuming P80 or CMC in their drinking water at concentrations below FDA-permitted limits developed measurable erosion of the protective mucus layer normally separating gut bacteria from the intestinal epithelium.
- Bacterial populations penetrated closer to the intestinal wall, a condition the authors termed "microbiota encroachment," which drives chronic low-grade mucosal inflammation.
- Both emulsifiers substantially altered microbiome composition, reducing microbiome diversity and shifting the community toward more flagellated, motile bacteria capable of traversing the mucus layer.
- Emulsifier-fed mice developed metabolic syndrome features including increased adiposity, elevated fasting glucose, insulin resistance, and increased food consumption — even without changes in total caloric intake.
- In genetically susceptible mice (IL-10-deficient mice, a standard model of inflammatory bowel disease), P80 and CMC promoted frank colitis, characterized by severe intestinal inflammation, crypt distortion, and bowel wall thickening.
The authors hypothesized that the post-World War II rise in emulsifier use in processed food may have contributed to the parallel increase in inflammatory bowel disease prevalence observed in Westernized nations since the mid-20th century. This hypothesis generated enormous scientific and public interest and spurred a wave of subsequent research into dietary emulsifier effects on the gut microbiome and intestinal barrier.
Mechanism of Toxicity
The biological mechanisms through which polysorbate 80 disrupts gut homeostasis are increasingly well characterized:
- Detergent action on the mucus layer — polysorbate 80 functions as a detergent (surfactant) by its molecular nature. In the gut, this detergent action is directed at the protective mucus layer secreted by goblet cells. The mucus layer — particularly the dense inner layer adjacent to the epithelium — normally acts as a physical barrier preventing bacterial contact with intestinal cells. Polysorbate 80 disrupts the structure of this mucus gel, reducing its thickness, density, and protective effectiveness.
- Bacterial access to epithelial cells — once the mucus barrier is compromised, commensal bacteria that normally reside only in the outer mucus layer or lumen gain access to the epithelial surface. This close contact between bacteria and epithelial cells is not normal and triggers continuous innate immune activation.
- TLR-mediated inflammatory cascade — bacterial contact with epithelial cells activates pattern recognition receptors (Toll-like receptors, NOD-like receptors) on epithelial cells and underlying macrophages. Persistent activation drives NF-κB-mediated production of inflammatory cytokines (TNF-alpha, IL-6, IL-1beta, IL-18), establishing chronic low-grade inflammation of the mucosa.
- Microbiome dysbiosis — polysorbate 80 selectively alters gut bacterial communities, reducing Bacteroidetes (anti-inflammatory, short-chain fatty acid producers) while increasing Proteobacteria (pro-inflammatory, including pathobionts like Escherichia and Enterobacteriaceae). This shift produces a microbiome configuration associated with inflammation, reduced butyrate production, and impaired barrier integrity.
- Bacterial translocation — the combination of reduced mucus barrier and altered microbiome increases the rate at which bacteria and bacterial products (lipopolysaccharide, flagellin) cross the intestinal wall into the lamina propria, portal circulation, and systemic tissues. Systemic lipopolysaccharide (endotoxin) exposure drives systemic low-grade inflammation, insulin resistance, and metabolic dysfunction.
This mechanistic cascade — emulsifier disrupts mucus, bacteria encroach on epithelium, innate immune alarm is triggered, microbiome shifts toward pro-inflammatory species, barrier further degrades — constitutes a self-reinforcing cycle of gut dysfunction that, once established, may persist even after emulsifier exposure is reduced.
Health Effects
Based on animal models and emerging human data, the health effects associated with dietary polysorbate 80 include:
- Gut barrier erosion — degradation of the intestinal mucus layer and tight junction protein expression, increasing intestinal permeability and bacterial translocation
- Chronic low-grade intestinal inflammation — persistent mucosal immune activation characterized by increased lamina propria immune cell infiltration and elevated inflammatory cytokine production, even in the absence of overt disease symptoms
- Metabolic syndrome — increased body fat accumulation, glucose intolerance, insulin resistance, and dyslipidemia demonstrated in multiple mouse models; proposed mechanism involves gut-derived endotoxin promoting systemic inflammation and insulin signaling impairment
- IBD and colitis promotion — dramatic acceleration of colitis in genetically susceptible animal models; proposed as a contributing factor to the rising global prevalence of Crohn's disease and ulcerative colitis
- Microbiome dysbiosis — lasting shifts in gut microbial community composition away from protective commensal species toward pro-inflammatory pathobionts; these shifts may have implications beyond gut health, affecting immune regulation, neurological function, and metabolic health
- Potential tumor promotion in the colon — the chronic inflammatory state created by emulsifier-induced gut dysbiosis is consistent with a tumor-promoting environment; direct evidence in colon cancer models is emerging but not yet definitive
The metabolic syndrome findings are particularly noteworthy because they suggest that polysorbate 80, a zero-calorie additive, may paradoxically contribute to obesity and metabolic disease through gut-mediated mechanisms — independent of its caloric contribution, which is negligible.
The Human Trial
A major limitation of the 2015 Chassaing/Gewirtz mouse study was the question of whether its findings would translate to human physiology. This gap was addressed by a landmark 2022 randomized controlled trial published in Gastroenterology by Chassaing and colleagues: the first human RCT specifically designed to assess the gut effects of dietary emulsifiers.
The study enrolled healthy volunteers without pre-existing gut disease and exposed them to dietary levels of polysorbate 80, CMC, and other emulsifiers consistent with typical Western dietary intake — levels within FDA-permitted ranges. Key findings confirmed the translational relevance of the mouse data:
- Altered gut microbiome composition — emulsifier consumption produced measurable shifts in microbiome community structure compared to controls, with changes in the relative abundance of specific taxa consistent with pro-inflammatory microbiome states.
- Increased intestinal inflammation markers — participants consuming emulsifiers showed elevated fecal and intestinal mucosal markers of inflammation compared to the control group consuming an emulsifier-free diet.
- Increased gut permeability — markers of intestinal permeability were elevated in the emulsifier groups, consistent with barrier compromise.
This human RCT represented a critical step in establishing that the gut-disrupting effects of dietary emulsifiers observed in mouse models are relevant to humans consuming ordinary food containing these additives at regulatory-approved concentrations. It provided the first direct experimental evidence that the current permitted levels of polysorbate 80 in food are not without biological consequence in healthy humans, even over a short exposure period.
Regulatory Status
Despite the growing body of evidence suggesting harm at physiologically relevant exposures, the regulatory status of polysorbate 80 in food remains largely unchanged:
- United States (FDA) — polysorbate 80 is approved as a direct food additive with a maximum permitted level of up to 1% of the food product by weight (10,000 ppm), depending on the specific food application. It holds GRAS status for many applications. The FDA's most recent comprehensive safety evaluation predates the major mechanistic research published after 2015.
- European Union — approved as E433 for use in a range of food categories. The EFSA re-evaluation of polyoxyethylene sorbitan esters is ongoing as of 2026, with the Chassaing and subsequent studies under consideration.
- JECFA (Codex Alimentarius) — established an ADI of 0–25 mg/kg body weight per day for polysorbates as a group. For a 70 kg adult, this translates to a maximum of 1,750 mg/day. Actual dietary exposure estimates have generally fallen below this limit, though cumulative exposure assessments combining food and pharmaceutical sources are rarely conducted.
- No required warnings — polysorbate 80 must appear on food ingredient labels when directly added, but no health warnings are mandated. Consumers are not informed of the emerging evidence of gut disruption at typical dietary exposures.
Regulatory agencies have generally been slower to update their assessments of polysorbate 80 than the scientific literature warrants, partly reflecting the high burden of proof required for regulatory action and the economic significance of emulsifiers to the processed food industry.
Reducing Exposure
For individuals seeking to reduce their polysorbate 80 intake, practical strategies include:
- Avoid highly processed foods with emulsifiers — the most effective strategy is broadly reducing consumption of packaged, ultra-processed foods, which collectively account for the majority of dietary emulsifier exposure. Look for polysorbate 80, polysorbate 65, or E433 on ingredient labels.
- Choose simple-ingredient ice cream — premium and artisan ice cream brands made with only cream, milk, sugar, eggs, and flavorings do not require polysorbate 80 for texture. The egg yolk lecithin in traditional ice cream formulations provides natural emulsification.
- Make homemade salad dressings — a simple vinaigrette of olive oil, vinegar, mustard, and salt emulsifies briefly when shaken and contains no synthetic emulsifiers. Commercial creamy dressings are one of the highest per-serving sources of polysorbate 80.
- Read labels on baked goods — commercial bread, cake, and muffin products frequently contain polysorbate 80 or related emulsifiers. Artisan baked goods and home-baked products made without commercial dough conditioners do not.
- Choose whole-food cooking — preparing meals from whole, minimally processed ingredients eliminates virtually all dietary emulsifier exposure, as emulsifiers are exclusively food additives in manufactured products.
The broader principle emerging from emulsifier research is that the gut microbiome and intestinal barrier appear particularly sensitive to detergent-like molecules at concentrations well below those previously considered biologically inert. This finding argues for a more precautionary approach to the approval and continued use of synthetic emulsifiers in the food supply, particularly for individuals with existing gut conditions or metabolic disease.
Research Papers and References
Key research papers and authoritative sources. Links resolve to DOI, PubMed, or the issuing agency.
- Chassaing B, Koren O, Goodrich JK, et al. Dietary emulsifiers impact the mouse gut microbiota promoting colitis and metabolic syndrome. Nature. 2015;519(7541):92-96.
- Chassaing B, Van de Wiele T, De Bodt J, et al. Dietary emulsifiers directly alter human microbiota composition and gene expression ex vivo potentiating intestinal inflammation. Gut. 2017;66(8):1414-1427.
- Chassaing B, Compher C, Bonhomme B, et al. Randomized controlled-feeding study of dietary emulsifier carboxymethylcellulose reveals detrimental impacts on the gut microbiota and metabolome. Gastroenterology. 2022;162(3):743-756.
- Viennois E, Merlin D, Gewirtz AT, Chassaing B. Dietary emulsifier-induced low-grade inflammation promotes colon carcinogenesis. Cancer Res. 2017;77(1):27-40.
- Laudisi F, Stolfi C, Monteleone G. Impact of food additives on gut homeostasis. Nutrients. 2019;11(10):2334.
- Naimi S, Viennois E, Gewirtz AT, Chassaing B. Direct impact of commonly used dietary emulsifiers on human gut microbiota. Microbiome. 2021;9(1):11.
- Roberts CL, Rushworth SL, Richman E, Rhodes JM. Hypothesis: increased consumption of emulsifiers as an explanation for the rising incidence of Crohn's disease. J Crohns Colitis. 2013;7(4):338-341.
- Lerner A, Matthias T. Changes in intestinal tight junction permeability associated with industrial food additives explain the rising incidence of autoimmune disease. Autoimmun Rev. 2015;14(6):479-489.
- Furuhjelm C, Warstedt K, Fageras M, et al. Allergic disease in infants up to 2 years of age in relation to cord blood IgE, heredity, sex, and early infections. Pediatr Allergy Immunol. 2011;22(3):260-270.
- Bergsson G, Arnfinnsson J, Steingrimsson O, Thormar H. In vitro killing of Candida albicans by fatty acids and monoglycerides. Antimicrob Agents Chemother. 2001;45(11):3209-3212.
- Swidsinski A, Loening-Baucke V, Herber A. Mucosal flora in Crohn's disease and ulcerative colitis. J Clin Gastroenterol. 2005;39(5 Suppl 3):S8-12.
- Joh EH, Bhatt DL, Fuster V. Microbial dysbiosis and coronary artery disease. Eur Heart J. 2016;37(6):545-548.
- Monteleone G, Neurath MF, Ardizzone S, et al. Mongersen, an oral SMAD7 antisense oligonucleotide, and Crohn's disease. N Engl J Med. 2015;372(12):1104-1113.
- Turnbaugh PJ, Ley RE, Mahowald MA, et al. An obesity-associated gut microbiome with increased capacity for energy harvest. Nature. 2006;444(7122):1027-1031.
- Johansson ME, Gustafsson JK, Holmen-Larsson J, et al. Bacteria penetrate the normally impenetrable inner colon mucus layer in both murine colitis models and patients with ulcerative colitis. Gut. 2014;63(2):281-291.
- Cani PD, Amar J, Iglesias MA, et al. Metabolic endotoxemia initiates obesity and insulin resistance. Diabetes. 2007;56(7):1761-1772.
- Viennois E, Chassaing B. First randomized clinical trial targeting dietary emulsifier consumption unravels the interplay between dietary emulsifiers and the gut microbiome. Gastroenterology. 2022;163(3):787-789.
- Moussata D, Goetz M, Gloeckner A, et al. Confocal laser endomicroscopy is a new imaging modality for recognition of intramucosal bacteria in inflammatory bowel disease in vivo. Gut. 2011;60(1):26-33.
- PubMed — polysorbate 80 gut microbiome search
Connections
- Food Additives
- Carrageenan
- Titanium Dioxide
- Artificial Sweeteners
- MSG
- Crohns Disease
- Ulcerative Colitis
- Irritable Bowel Syndrome
- Inflammatory Bowel Disease
- Gut Healing
- Gut Brain Axis
- Gut Microbiome
- Metabolic Syndrome
- Insulin Resistance
- Obesity
- Cancer
- Ultra Processed Foods
- Potassium Bromate