Titanium Dioxide (E171): The Whitening Agent Banned in Europe
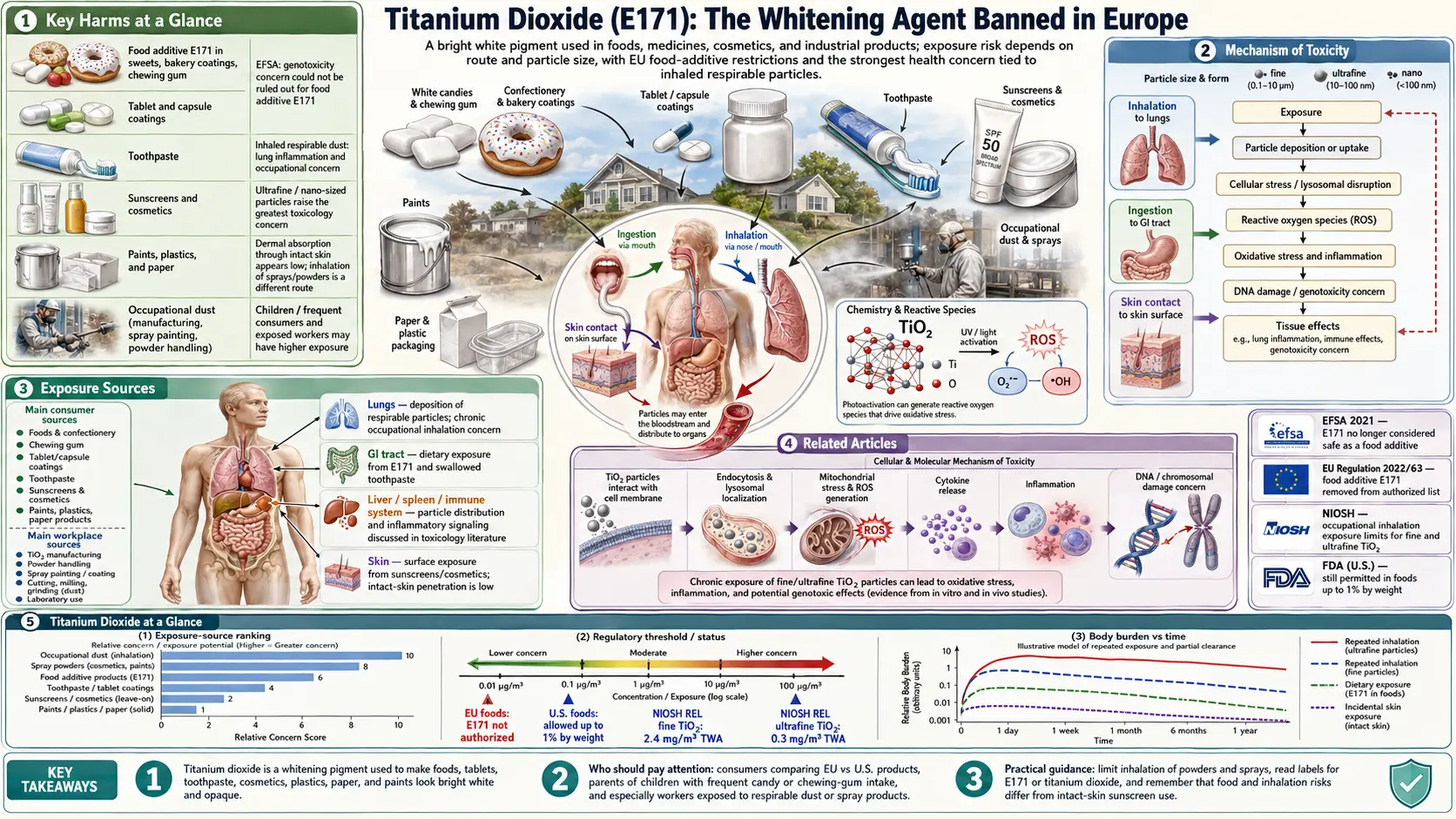
Titanium dioxide is one of the most widely used food additives in the world — found in everything from candy coatings to chewing gum — yet it was banned from all food products in the European Union in 2022 after safety authorities concluded it could no longer be considered safe. The substance remains fully approved in the United States.
Table of Contents
- Key Harms at a Glance
- Overview
- Regulatory History
- Mechanism of Toxicity
- Health Effects
- Exposure Sources
- Children's Vulnerability
- Safer Alternatives
- Related Articles
- Research Papers and References
- Connections
- Featured Videos
Key Harms at a Glance
- EFSA 2021: no longer considered safe — genotoxicity concerns prevent establishing an ADI.
- EU-wide food ban (2022) — removed from all food products under Regulation 2022/63.
- Nanoparticle translocation — crosses gut epithelium via Peyer's-patch M cells.
- DNA strand breaks and chromosomal aberrations — demonstrated in vitro and in vivo.
- NLRP3 inflammasome activation — drives IL-1beta-mediated intestinal inflammation.
- Accumulates in Peyer's patches — age-dependent deposition in human intestinal immune tissue.
- Children 3–5x higher exposure per kg — candy, gum, and powdered pastries dominate pediatric intake.
1. Overview
Titanium dioxide (TiO2), designated E171 in the European food additive numbering system, is an inorganic compound used as a white colorant and opacifier in processed foods, pharmaceuticals, cosmetics, and industrial products. It is derived primarily from ilmenite ore through either the sulfate or chloride process and is known for producing an exceptionally bright, clean white appearance.
In food applications, titanium dioxide exists as microscopic particles ranging from roughly 100 to 400 nanometers in diameter — with a significant fraction falling into the nanomaterial range (below 100 nm). This nano-sized fraction is of particular toxicological concern because particles at this scale behave very differently from bulk materials: they exhibit higher surface reactivity, greater capacity to penetrate biological membranes, and different biodistribution patterns in the body.
Key uses of titanium dioxide include:
- Confectionery: hard candies, candy-coated chocolates, chewing gum, and powdered sugar coatings
- Baked goods: powdered donuts, frosting, cake decorations
- Dairy products: coffee creamers, whipped toppings
- Condiments: salad dressings, sauces
- Personal care products: toothpaste, sunscreen, cosmetics
- Pharmaceuticals: tablet coatings, capsule shells, liquid medications
Its appeal as an additive stems from its chemical inertness (it does not react with food components), extremely high refractive index (2.6, the highest of any known substance), and low cost. These properties make it ideal for producing bright white or opaque appearances in products where visual appeal drives consumer preference.
2. Regulatory History
The regulatory trajectory of titanium dioxide illustrates a growing divide between European and American food safety approaches.
United States
The U.S. Food and Drug Administration (FDA) approved titanium dioxide as a food color additive in 1966. It is listed under 21 CFR 73.575 and classified as Generally Recognized As Safe (GRAS) for use in food with a maximum concentration of 1% by weight of the finished food. This approval has not been substantially revisited despite decades of new scientific evidence.
France — First National Ban (2020)
France became the first country to act when it banned titanium dioxide from food products effective January 1, 2020, citing precautionary principle concerns and preliminary evidence of genotoxicity. This was implemented under Article L. 5311-1 of the French Public Health Code.
EFSA Opinion — 2021
The European Food Safety Authority (EFSA) issued a landmark reassessment in May 2021, concluding that "titanium dioxide can no longer be considered safe as a food additive." The panel's critical finding was that it could not rule out genotoxicity — the ability to damage DNA — and that this concern prevented the establishment of any acceptable daily intake. The 2021 opinion explicitly cited the nanoparticle fraction as a key driver of concern.
EU-Wide Ban — August 2022
Following the EFSA opinion, the European Commission issued Regulation (EU) 2022/63, which removed E171 from the list of permitted food additives across all EU member states. The ban took effect on August 7, 2022, with a 6-month transition period for products already on shelves. This effectively prohibited titanium dioxide from all food products sold in the EU, regardless of origin.
Current Global Status
Despite the EU ban, the United States, Canada, Australia, and many other countries continue to permit E171 in food. The International Agency for Research on Cancer (IARC) classified inhaled titanium dioxide as a Group 2B carcinogen (possibly carcinogenic to humans) in 2006, though this assessment concerned occupational inhalation exposure rather than dietary ingestion.
3. Mechanism of Toxicity
The toxicological mechanisms of titanium dioxide are driven primarily by its nanoparticle fraction and its behavior within the gastrointestinal tract.
Nanoparticle Translocation Across the Gut Epithelium
After ingestion, TiO2 particles are not efficiently absorbed by the small intestine in the traditional sense, but nano-sized particles can translocate across the gut epithelium through transcytosis, particularly via M cells overlying Peyer's patches — the lymphoid follicles of the intestinal immune system. Once inside these structures, nanoparticles accumulate and persist, potentially triggering chronic immune stimulation.
Oxidative Stress
TiO2 nanoparticles generate reactive oxygen species (ROS) both through direct photocatalysis (under UV light) and through interaction with cellular components. Intracellular ROS production leads to lipid peroxidation, protein oxidation, and mitochondrial dysfunction. The gut epithelium, with its high cell turnover rate, is particularly vulnerable to oxidative damage.
Genotoxicity and DNA Damage
Multiple in vitro and in vivo studies have demonstrated that TiO2 nanoparticles can cause DNA strand breaks, chromosomal aberrations, and micronucleus formation — classic markers of genotoxicity. The EFSA panel's inability to rule out genotoxicity was based on this body of evidence. While the exact mechanism remains under investigation, ROS-mediated oxidative damage to DNA appears to be a primary pathway. Clastogenic effects (chromosome breakage) have been observed in several mammalian cell studies.
Disruption of the Intestinal Barrier
Chronic exposure to TiO2 has been shown to impair the integrity of the intestinal tight junctions — the protein complexes that seal the spaces between epithelial cells. This "leaky gut" effect allows bacterial products and other luminal antigens to translocate into systemic circulation, triggering inflammatory responses. Studies in rodent models show reduced expression of tight junction proteins such as occludin and claudin-1 following TiO2 exposure.
NLRP3 Inflammasome Activation
TiO2 nanoparticles activate the NLRP3 inflammasome — a multiprotein complex that drives inflammatory signaling via IL-1β and IL-18 release. This pathway plays a central role in intestinal inflammation and has been implicated in the pathogenesis of inflammatory bowel diseases including Crohn's disease and ulcerative colitis.
Accumulation in Peyer's Patches
Post-mortem human tissue studies have confirmed that titanium dioxide accumulates in Peyer's patches, with concentrations increasing with age. This finding suggests that dietary TiO2 is not simply excreted but deposits in intestinal immune tissue over time, with potential for cumulative effects.
4. Health Effects
Gut Microbiome Disruption
Animal studies have demonstrated that oral TiO2 exposure significantly alters the gut microbiome composition, reducing microbial diversity and shifting the ratio of beneficial to potentially harmful bacteria. Specifically, researchers have observed reductions in Lactobacillus and Bifidobacterium species alongside increases in pro-inflammatory taxa. Microbiome dysbiosis may amplify the inflammatory effects of TiO2 in the gut.
Intestinal Inflammation and IBD-Like Effects
Long-term oral exposure studies in rodents have produced histological changes resembling early-stage inflammatory bowel disease, including villous atrophy, crypt hyperplasia, and increased immune cell infiltration in the lamina propria. Epidemiological work has found elevated TiO2 concentrations in the gut tissue of patients with Crohn's disease and ulcerative colitis, though causality has not been established.
Potential Carcinogenicity
IARC classified titanium dioxide as Group 2B — possibly carcinogenic to humans in 2006, based on sufficient evidence of carcinogenicity in experimental animals (primarily via inhalation) and inadequate evidence in humans. For dietary exposure, animal studies using gavage (forced feeding) have produced equivocal carcinogenicity data, but genotoxic potential and chronic intestinal inflammation are both recognized precursors to colorectal cancer development.
Immune System Effects
TiO2 nanoparticles deposited in Peyer's patches interact directly with macrophages and dendritic cells, skewing immune responses. Studies have observed both immunosuppressive and pro-inflammatory effects depending on particle size, dose, and duration of exposure. Chronic stimulation of gut-associated lymphoid tissue may contribute to systemic immune dysregulation.
Reproductive Toxicity in Animal Studies
Rodent studies have reported reproductive effects including reduced sperm motility, altered ovarian function, and developmental abnormalities in offspring of TiO2-exposed animals. These effects have generally been observed at higher doses than typical dietary exposure, but the relevance to human dietary exposure — particularly in pregnant women — remains a concern given the lack of an established safe threshold.
5. Exposure Sources
Titanium dioxide enters the diet primarily through highly processed foods where its whitening and brightening properties are commercially valuable:
Candy and Confectionery
- Skittles, M&Ms, Starburst: candy shell coatings rely heavily on TiO2 for their bright white and opaque base layer beneath colored coatings
- Hard candies and lollipops with white or pastel colors
- Marshmallows and candy-coated nuts
Baked and Powdered Products
- Powdered donuts and pastries (the white powdered sugar coating often contains TiO2)
- White cake frosting and fondant
- Confectioner's sugar in some commercial formulations
Dairy and Creamers
- Non-dairy coffee creamers (both powdered and liquid)
- Whipped toppings and some ice cream products
- Processed cheese products
Condiments and Dressings
- Ranch dressing, Caesar dressing, and other creamy salad dressings
- Horseradish sauce, mayonnaise-based products
Pharmaceuticals and Supplements
- Tablet and capsule coatings (widely used as a pharmaceutical excipient)
- Liquid medications and antacids
- Dietary supplement capsules and pressed tablets
Chewing Gum
Many white or light-colored chewing gums contain substantial amounts of TiO2 to achieve their opaque white appearance. Gum is particularly concerning because the additive remains in contact with the oral mucosa for extended periods.
Toothpaste
Nearly all white toothpastes contain titanium dioxide as a whitening pigment. While toothpaste is not intended for ingestion, children routinely swallow small amounts, and some absorption through oral mucosa is possible.
6. Children's Vulnerability
Children face disproportionately higher risk from titanium dioxide exposure for several interconnected reasons:
Higher Per-Kilogram Consumption
Children consume far more candy, gum, powdered donuts, and confectionery items relative to their body weight than adults. Exposure assessments conducted by EFSA found that children's estimated daily intake of TiO2 from food could be 3–5 times higher on a body-weight basis than adult intake.
Developing Gastrointestinal Tract
The intestinal barrier in young children is more permeable than in adults, potentially allowing greater translocation of nanoparticles. The gut microbiome is also still developing and colonizing through early childhood, making it more susceptible to disruption. Intestinal Peyer's patches are proportionally larger and more active in children, representing a larger depot for particle accumulation.
Developing Immune System
The immune system continues to mature through adolescence. Chronic stimulation or dysregulation of gut-associated lymphoid tissue during this critical window may have lasting consequences for immune development and disease susceptibility.
School Snack Foods
Many of the foods most popular with school-age children — candy, gum, powdered pastries, and flavored snack products — are among the highest sources of dietary TiO2. Unlike adults, children have less dietary control and may consume these foods daily.
7. Safer Alternatives
The EU ban prompted significant reformulation efforts among food manufacturers, demonstrating that effective substitutes exist:
Calcium Carbonate
Calcium carbonate (E170) is the most widely adopted substitute for TiO2 in candy coatings and tablet coatings. It provides good whiteness and opacity, is nutritionally benign (it actually adds bioavailable calcium), and has a well-established safety record. The main limitation is slightly lower whitening power compared to TiO2.
Rice Starch
Finely milled rice starch produces a white, matte appearance in food products and functions well as a dusting agent for confectionery. It is clean-label, allergen-free, and widely accepted by consumers seeking natural ingredients.
Corn Starch
Modified corn starch can replace TiO2 in powdered coatings and confectionery applications. It is inexpensive, readily available, and does not carry any toxicological concerns at food-grade concentrations.
Other Natural Whiteners
Additional options include microcrystalline cellulose, talc (in limited applications), and white mineral clay (kaolin), though each has its own limitations in terms of application and regulatory status across different markets. Some manufacturers have achieved comparable whiteness through reformulation of the food matrix itself, reducing the need for a dedicated whitening agent.
8. Related Articles
9. Research Papers and References
Key research papers and authoritative sources. Links resolve to DOI, PubMed, or the issuing agency.
- EFSA Panel on Food Additives and Flavourings (FAF). Re-evaluation of titanium dioxide (E 171) as a food additive. EFSA Journal. 2021;19(5):e06585.
- European Commission. Commission Regulation (EU) 2022/63 of 14 January 2022 amending Annexes II and III to Regulation (EC) No 1333/2008. Official Journal of the European Union. 2022.
- Bettini S, Boutet-Robinet E, Cartier C, et al. Food-grade TiO2 impairs intestinal and systemic immune homeostasis, initiates preneoplastic lesions and promotes aberrant crypt development in the rat colon. Scientific Reports. 2017;7:40373.
- Pele LC, Martin-Ortigosa S, Cook R, et al. Particle and molecular size of food-grade titanium dioxide and its effects on colonic DNA damage, biomarkers of inflammation and gene expression. Mutagenesis. 2015;30(6):803–813.
- Urrutia-Ortega IM, Garduno-Balderas LG, Delgado-Buenrostro NL, et al. Food-grade titanium dioxide exposure exacerbates tumor formation in colitis associated cancer model. Food and Chemical Toxicology. 2016;93:20–31.
- Ruiz PA, Morón B, Blumberg RS, et al. Titanium dioxide nanoparticles exacerbate DSS-induced colitis by promoting oxidative stress in murine intestinal epithelium. Nanomedicine: Nanotechnology, Biology and Medicine. 2017;13(5):1763–1782.
- Heringa MB, Geraets L, van Eijkeren JC, et al. Risk assessment of titanium dioxide nanoparticles via oral exposure, including toxicokinetic considerations. Nanotoxicology. 2016;10(10):1515–1525.
- Lomer MC, Thompson RP, Powell JJ. Fine and ultrafine particles of the diet: influence on the mucosal immune response and association with Crohn's disease. Proceedings of the Nutrition Society. 2002;61(1):123–130.
- Nogueira CM, de Azevedo WM, Dagli ML, et al. Titanium dioxide induced inflammation in the small intestine. World Journal of Gastroenterology. 2012;18(34):4709–4719.
- Cao X, Han Y, Gu M, et al. Foodborne titanium dioxide nanoparticles induce stronger adverse effects in obese mice than non-obese mice: Gut microbiota dysbiosis, colitis, and colorectal cancer. Small. 2020;16(36):e2001858.
- Rompelberg C, Heringa MB, van Donkersgoed G, et al. Oral intake of added titanium dioxide and its nanofraction from food products, food supplements and toothpaste by the Dutch population. Nanotoxicology. 2016;10(10):1404–1414.
- IARC. Titanium Dioxide. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, Vol. 93. Lyon: International Agency for Research on Cancer; 2006.
- Szakal C, Roberts SM, Westerhoff P, et al. Measurement of nanomaterials in foods: integrative consideration of challenges and future prospects. ACS Nano. 2014;8(4):3128–3135.
- Weir A, Westerhoff P, Fabricius L, et al. Titanium dioxide nanoparticles in food and personal care products. Environmental Science and Technology. 2012;46(4):2242–2250.
- U.S. Food and Drug Administration. CFR — Code of Federal Regulations Title 21, Part 73.575: Titanium Dioxide. U.S. FDA; 2023.
- Gao X, Topping VD, Croley TR, et al. Simulated gastrointestinal digestion of titanium dioxide nanoparticles: influence on NP dispersion and cytotoxicity. Food and Chemical Toxicology. 2017;109:286–294.
- Pinget G, Tan J, Janac B, et al. Impact of the food additive titanium dioxide (E171) on gut microbiota-host interaction. Frontiers in Nutrition. 2019;6:57.
- PubMed — titanium dioxide E171 intestinal search
Connections
- Food Additives
- Food Dyes
- Banned Additives
- Crohn's Disease
- Ulcerative Colitis
- Carrageenan
- Polysorbate 80
- Inflammatory Bowel Disease
- Cancer
- Gut Brain Axis
- Oxidative Stress
- Calcium
- MSG
- Artificial Sweeteners
- Irritable Bowel Syndrome
- US vs EU Food Safety
- Food Dyes Banned Worldwide
- Heavy Metals in Cosmetics