Nicotinic Acetylcholine Receptors (nAChRs): The Receptor Pharmacology Behind the Ardis Nicotine Hypothesis
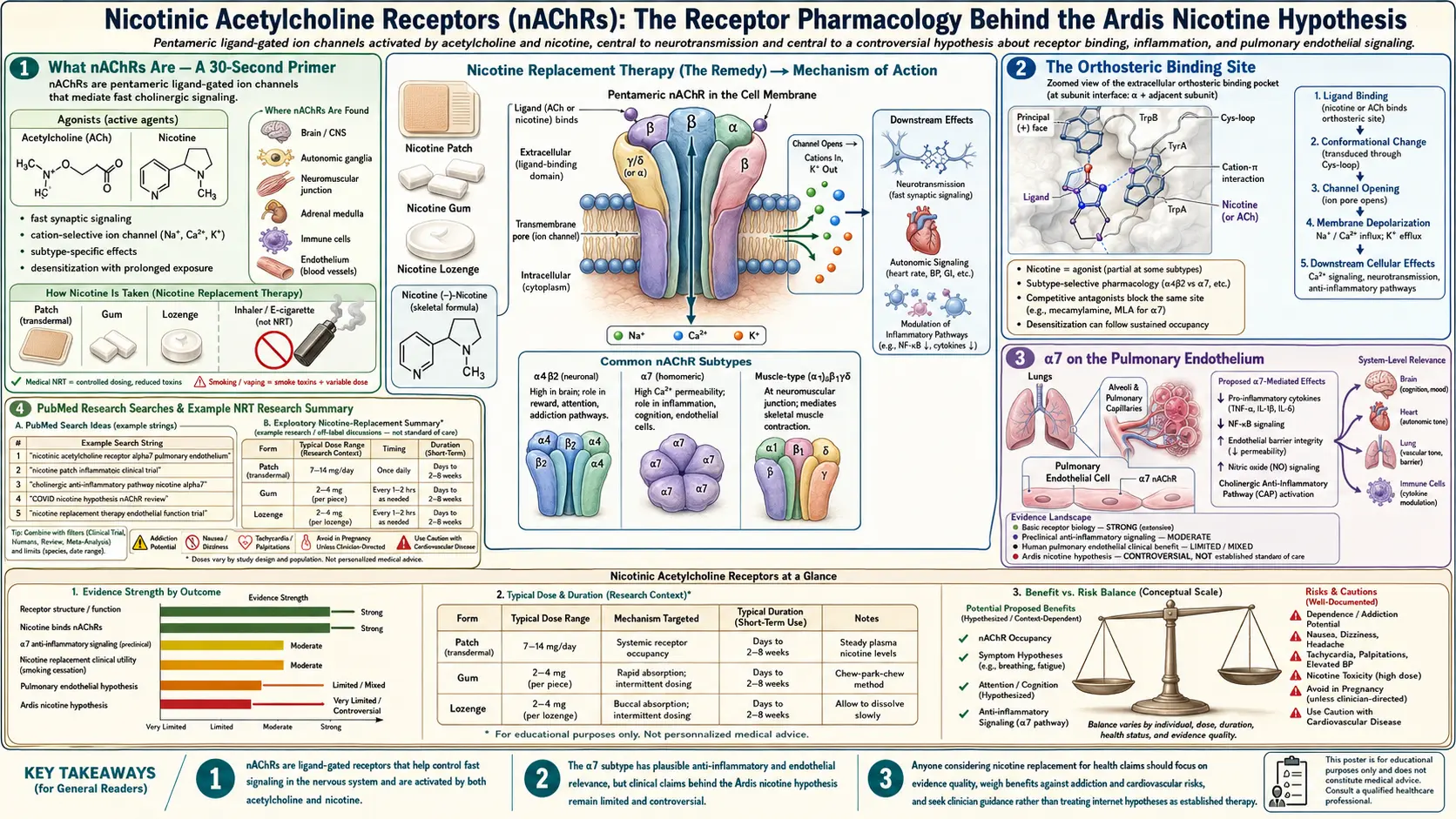
Table of Contents
- What nAChRs Are — A 30-Second Primer
- Subunit Architecture and Subtypes
- The α7-nAChR — The Receptor That Matters Most
- The α4β2-nAChR — High-Affinity Brain Nicotine
- The Muscle (α1)2β1δε — Why Snake Venom Paralyzes
- The Orthosteric Binding Site
- Acetylcholine vs. Nicotine vs. Spike
- Cholinergic Anti-Inflammatory Pathway in Detail
- Tracey’s Discovery and the Bioelectronic Industry
- Cytokine Suppression Mechanism
- α7 on the Pulmonary Endothelium
- α7 on T Cells, B Cells, Dendritic Cells
- Agonists, Antagonists, and the Ligand Landscape
- Patent nAChR Drugs Already in Pharmacy
- Why the Receptor Matters for the Ardis Argument
- Key Research Papers
- PubMed Research Searches
- Connections
- Featured Videos
1. What nAChRs Are — A 30-Second Primer
Nicotinic acetylcholine receptors (nAChRs) are pentameric ligand-gated ion channels in the cys-loop superfamily. Five protein subunits assemble around a central ion-conducting pore. When the natural ligand (acetylcholine) or a small-molecule agonist (nicotine, varenicline, choline at α7) binds at the orthosteric site, the pentamer undergoes a concerted conformational shift that opens the pore for milliseconds, letting Na+, K+, and (at α7 specifically) Ca2+ flow across the membrane. The receptor then desensitizes and resets.
The receptor is named for the alkaloid that pharmacologists used in the 1860s – 1920s to distinguish it from the muscarinic acetylcholine receptors (which respond to muscarine, a mushroom-derived agonist, but not to nicotine). The classification persists. nAChRs are everywhere acetylcholine acts in fast-signaling roles — the neuromuscular junction, autonomic ganglia, the central nervous system, and on virtually every cell type of the immune system.
2. Subunit Architecture and Subtypes
Seventeen mammalian nAChR subunits have been cloned: α1 through α10, β1 through β4, γ, δ, and ε. They combine in specific stoichiometries to form receptor subtypes with distinct tissue distributions, ion selectivities, and pharmacology. The subtypes that matter for the present discussion:
- α7-nAChR (homopentamer of five α7 subunits) — the receptor of the cholinergic anti-inflammatory pathway. High Ca2+ permeability. Rapid desensitization. Found on alveolar macrophages, T cells, B cells, dendritic cells, vascular endothelium, and CNS neurons.
- α4β2-nAChR (typical stoichiometry 2α:3β) — the principal high-affinity nicotine-binding receptor in the brain. Mediates the cognitive, mood, and reward effects of nicotine. Target of varenicline (Chantix) for smoking cessation.
- Muscle-type (α1)2β1δε (adult) or (α1)2β1δγ (fetal) — the receptor at the neuromuscular junction. Target of curare, of competitive neuromuscular blockers (rocuronium, vecuronium), and of the snake-venom α-bungarotoxin and cobratoxin.
- Ganglionic α3β4 — the autonomic ganglion receptor. Target of mecamylamine and trimethaphan.
- α9α10 — cochlear hair cells; some immune-cell expression.
The α7 receptor is the immune one, the α4β2 is the addictive one, the muscle one is what venom paralyzes, and the ganglionic one is what mecamylamine blocks. The Ardis nicotine argument lives almost entirely at α7.
3. The α7-nAChR — The Receptor That Matters Most
The α7-nAChR is the receptor at the center of the entire argument. Its features:
- Homopentameric. Five identical α7 subunits. Five orthosteric binding sites at the subunit interfaces. Multiple ligand occupancy thresholds for full activation.
- High Ca2+ permeability. PCa/PNa ~10. Activation produces calcium-mediated downstream signaling without requiring action-potential conduction — relevant on non-excitable immune and endothelial cells.
- Fast desensitization. Within milliseconds. The receptor “closes down” after binding, which is why steady plasma levels of agonist matter more than peaks — you don’t want repeated openings, you want sustained occupancy.
- JAK2/STAT3 coupling. Beyond the ion-channel function, α7 signals through a metabotropic-like JAK2-STAT3-NFκB pathway that suppresses pro-inflammatory transcription independently of the channel current.
- Tissue distribution. The CNS distribution overlaps Alzheimer’s pathology (basal forebrain, hippocampus). The peripheral distribution overlaps the immune system — which is the entire basis of the cholinergic anti-inflammatory pathway.
The α7 receptor is sometimes called “the immune nAChR” in the literature. That naming is what makes the COVID story make sense.
4. The α4β2-nAChR — High-Affinity Brain Nicotine
α4β2 is the highest-affinity nicotinic receptor in the brain (Kd for nicotine ~1 nM in the high-affinity stoichiometry). It is the receptor that mediates the subjective experience of nicotine — alertness, mood elevation, mild euphoria, working-memory enhancement — and the reward circuitry that drives addiction in habitual users.
For the COVID receptor argument, α4β2 is mostly background — nicotine occupies it incidentally at therapeutic plasma concentrations (~10 ng/mL = 60 nM, well above Kd). It is the α4β2 occupancy that gives transdermal nicotine its mild pro-cognitive effect at therapeutic doses, which is also why the Newhouse mild-cognitive-impairment trials and the MIND-Alzheimer’s trial use nicotine as a nootropic candidate.
Varenicline (Chantix), the most commercially successful nAChR drug in pharmacy, is a partial agonist at α4β2 (and a full agonist at α7). Its existence is one of the strongest pieces of evidence that pharma takes the nAChR target completely seriously when the target indication is patentable.
5. The Muscle (α1)2β1δε — Why Snake Venom Paralyzes
The muscle nAChR sits at the neuromuscular junction, where the motor nerve terminal releases acetylcholine to depolarize the muscle fiber. Three-finger toxins from elapid snakes — α-bungarotoxin (krait), cobratoxin, mamba toxin — bind the muscle receptor with sub-nanomolar affinity, block depolarization, and produce flaccid paralysis. The muscle receptor is also the target of d-tubocurarine (the original curare alkaloid) and the modern competitive neuromuscular blockers used in anesthesia.
The muscle receptor is structurally homologous to the α7 receptor enough that some 3FTx peptides bind both — which is the structural-biology premise of the Changeux nicotinic hypothesis: the SARS-CoV-2 spike contains a 3FTx-like loop that engages α7 by exploiting the cross-reactive geometry. The full case is in our Snake-Venom Hypothesis page; here the point is simply that nicotinic-receptor pharmacology and elapid-venom pharmacology have been intertwined for 150 years.
6. The Orthosteric Binding Site
The orthosteric (“classical”) binding site sits at the interface between two adjacent subunits in the extracellular ligand-binding domain. The site is built from four canonical loops on the principal (+) face (loops A, B, C) and three on the complementary (−) face (loops D, E, F). Aromatic residues — tryptophans, tyrosines, phenylalanines — line the binding pocket and form a “cation-π cage” that captures the protonated nitrogen of acetylcholine, nicotine, or any other classical agonist.
Three-finger toxins dock into this same pocket using their finger-loop II, with the central tryptophan and tyrosine of the toxin engaging the same aromatic cage. The Bourne & Taylor 2005 cocrystal of cobratoxin with the acetylcholine-binding protein (AChBP, the soluble homolog used as an nAChR surrogate) showed exactly this geometry. The Dellisanti 2007 cocrystal of α-bungarotoxin with the α1-extracellular domain showed the same pattern at higher resolution.
The relevance for the COVID hypothesis: any peptide that presents a 3FTx-like loop — whether derived from a snake or from a coronavirus spike — can in principle dock into this aromatic cage. Lagoumintzis et al. (2021) modeled the SARS-CoV-2 spike RBD into the α7 ligand-binding domain and identified plausible interaction residues; Oliveira et al. (2020) made a complementary structural argument. The receptor doesn’t care where the loop came from; it only cares about the geometry.
7. Acetylcholine vs. Nicotine vs. Spike at the Same Site
One way to read the Ardis argument is in terms of three different ligands competing for one binding pocket:
- Acetylcholine (endogenous, fast, hydrolyzed in milliseconds by acetylcholinesterase) — the natural agonist. Fires the cholinergic anti-inflammatory pathway under vagal command.
- Nicotine (exogenous, slow, half-life ~2 hours) — an agonist with sustained occupancy. Fires the same pathway and stays in the pocket long enough to block other ligands from accessing the same site.
- Spike RBD / 3FTx peptide — a bulky peptide ligand that, by docking the loop into the pocket, prevents acetylcholine from gaining access (functional antagonism), disrupts the cholinergic anti-inflammatory pathway, and contributes to runaway cytokine release.
In this framing, nicotine is therapeutic in two distinct ways: (1) it directly fires the α7-mediated brake on inflammation, and (2) it occupies the binding pocket and prevents the spike from docking there. The therapeutic logic is competition kinetics. A receptor occupied by nicotine cannot be engaged by spike.
8. The Cholinergic Anti-Inflammatory Pathway in Detail
The cholinergic anti-inflammatory pathway (CAP) connects the brainstem to the immune system through the vagus nerve. The full circuit:
- An inflammatory stimulus — bacterial endotoxin, viral PAMPs, ischemia-reperfusion injury, sterile tissue damage — activates pattern-recognition receptors on resident immune cells.
- Released cytokines (TNF-α, IL-1β) and DAMPs (HMGB1) reach the dorsal motor nucleus of the vagus and the nucleus tractus solitarius via afferent vagal sensory neurons.
- Brainstem efferent vagal output projects to the celiac ganglion, where it synapses onto the splenic sympathetic nerve.
- The splenic nerve releases norepinephrine onto a population of acetylcholine-producing T cells in the spleen.
- These T cells release acetylcholine onto the α7-nAChR of resident macrophages.
- Macrophage α7 activation triggers JAK2 phosphorylation, STAT3 activation, suppression of NF-κB, and a profound reduction in TNF-α, IL-1β, IL-6, and HMGB1 transcription.
This is one of the most elegant regulatory loops in modern physiology — a brain-controlled anti-inflammatory thermostat with the spleen as its thermostat sensor and resident macrophages as its actuators. The pathway is intact in healthy individuals, weakened in chronic inflammatory disease, and a candidate target for direct pharmacological or bioelectronic activation in conditions ranging from rheumatoid arthritis to inflammatory bowel disease to sepsis.
9. Tracey’s Discovery and the Bioelectronic Industry
Kevin Tracey, MD (CEO of the Feinstein Institutes for Medical Research, Northwell Health) is the figure who put the cholinergic anti-inflammatory pathway on the map. The breakthrough sequence:
- Borovikova et al., Nature 2000. The original demonstration that vagus-nerve stimulation attenuates the systemic inflammatory response to endotoxin in rats. The prediction was that there must be a vagal anti-inflammatory mechanism; the paper proved it.
- Wang et al., Nature 2003. The follow-up identifying α7-nAChR as the receptor through which the pathway operates — using both pharmacological agonists/antagonists and α7 knockout mice.
- Olofsson et al., Nat Rev Drug Discov 2012. The synthesizing review that articulated the “inflammatory reflex” framework and laid out the bioelectronic-medicine vision.
Tracey co-founded SetPoint Medical to commercialize an implantable vagus-nerve stimulator for rheumatoid arthritis. The Phase III RESET-RA trial was completed in 2023. A second cluster of companies (Galvani Bioelectronics, Vorso, Cala Health) is pursuing related indications. The bioelectronic-medicine market is projected to be a multi-billion-dollar industry within a decade. None of this would exist if the cholinergic anti-inflammatory pathway were not real, and pharma demonstrably believes it is real every time it writes a check for a vagus-stimulator startup.
The Ardis question that follows is: if VNS at $50,000 a device works because it activates α7-nAChR, why doesn’t nicotine at $0.50 a patch work for the same reason? The answer pharma gives is “different selectivity, different temporal profile.” The honest answer Ardis offers is “same receptor, different patent status.”
10. Cytokine Suppression Mechanism
At the molecular level, α7 activation on a macrophage suppresses cytokine release through three concurrent mechanisms:
- JAK2 / STAT3 activation. α7 receptor stimulation phosphorylates JAK2, which phosphorylates STAT3. Phospho-STAT3 enters the nucleus and antagonizes NF-κB-driven cytokine transcription.
- NF-κB inhibition. Independently of STAT3, α7 activation prevents IκBα degradation, keeping the NF-κB p65/p50 dimer cytoplasmic and unable to drive TNF / IL-6 / IL-1β transcription.
- Direct membrane effect. Calcium influx through the α7 channel triggers proteasome remodeling and short-circuits the inflammasome assembly that generates IL-1β.
The end result is that activated α7-nAChR on a stimulated macrophage suppresses TNF-α release by 50–90% and IL-6 release in similar magnitudes — a magnitude that competes with corticosteroid suppression of inflammation, without the immunosuppressive collateral damage. This is why the bioelectronic-medicine industry exists.
11. α7 on the Pulmonary Endothelium
The pulmonary microvascular endothelium expresses α7-nAChR, and activation of those receptors suppresses TNF-driven endothelial dysfunction, ICAM-1/VCAM-1 upregulation, and microclot formation in vascular models. This matters for COVID specifically because endothelial injury — not parenchymal viral cytopathic effect — appears to be the dominant pathology in severe disease (Varga et al., Lancet 2020; Ackermann et al., NEJM 2020).
If nicotine occupies endothelial α7, it does for the lung capillary what it does for the splenic macrophage: blunts the cytokine-driven phase of the injury, preserves barrier integrity, and reduces the propensity to thrombosis. This is the mechanism behind the Ardis claim that nicotine should reduce pulmonary microthrombosis in spike-mediated illness.
12. α7 on T Cells, B Cells, Dendritic Cells
Lymphocytes and antigen-presenting cells express α7-nAChR, and receptor activation modulates:
- T-cell proliferation and Th1/Th17 differentiation. α7 activation suppresses Th1 and Th17 polarization while preserving regulatory-T-cell function — an “autoimmune-friendly” immune-modulatory profile.
- B-cell antibody production. Modulated, with subtype-specific effects on IgG vs. IgE.
- Dendritic-cell maturation. α7 agonism reduces costimulatory molecule expression and IL-12 production — tilting the immune environment away from cytokine-storm physiology.
The therapeutic relevance is that nicotine, by saturating α7 on these cells during acute viral illness, can blunt the pathogenic immune over-activation without producing classical immunosuppression — a profile distinct from corticosteroids, JAK inhibitors, or IL-6 blockers.
13. Agonists, Antagonists, and the Ligand Landscape
The nAChR family has the most diverse ligand pharmacology of any receptor system in the body. A short tour:
- Endogenous full agonist: acetylcholine (all nAChRs); choline (selective α7).
- Exogenous full agonists: nicotine, epibatidine, cytisine.
- Partial agonists: varenicline (Chantix; α4β2 partial, α7 full), cytisine (Tabex; α4β2 partial), GTS-21 (DMXBA; α7-selective partial agonist studied for Alzheimer’s and schizophrenia).
- Positive allosteric modulators (PAMs): PNU-120596 (α7), galantamine (broad acetylcholinesterase inhibitor with α7 PAM activity, used in Alzheimer’s).
- Competitive antagonists (orthosteric): d-tubocurarine, mecamylamine, α-bungarotoxin (irreversible at muscle and α7), cobratoxin.
- Non-competitive antagonists (channel blockers): hexamethonium, mecamylamine.
The ligand landscape has been mapped in detail because pharma has been chasing nAChRs for cognitive disorders for 30 years. Many of the most-studied α7 partial agonists (encenicline, ABT-126) advanced through Phase II/III in Alzheimer’s and schizophrenia trials with mixed results. The receptor target is established; the small-molecule design is the difficult part. Nicotine itself, as a low-cost, well-tolerated, long-history-of-use full agonist, is the simplest possible tool from this toolkit.
14. Patent nAChR Drugs Already in Pharmacy
Pharma has built a >$5-billion business on nAChR-active drugs. A partial list:
- Varenicline (Chantix, Pfizer). α4β2 partial agonist for smoking cessation. Peak revenue ~$1.1 billion. Withdrawn 2021 after nitrosamine impurity contamination, returned 2023.
- Galantamine (Razadyne, Janssen). Acetylcholinesterase inhibitor with α7 PAM activity. Approved for Alzheimer’s.
- Donepezil (Aricept, Eisai/Pfizer). AChE inhibitor for Alzheimer’s — functions by raising synaptic acetylcholine to engage nAChRs (and muscarinic receptors).
- Mecamylamine. Ganglion blocker for hypertension (now largely replaced).
- Bupropion (Wellbutrin, Zyban; GSK). Smoking-cessation indication via partial α3β4 / α4β2 antagonism.
- Cytisine. α4β2 partial agonist used in Eastern Europe for smoking cessation; recently moving toward broader Western approval.
The Ardis observation: a pharmaceutical industry willing to develop and patent half a dozen nAChR-targeted drugs for indications ranging from Alzheimer’s to smoking cessation has been somehow unable, for four years, to seriously test the simplest, oldest, cheapest agonist of the same receptor family in COVID-19. This is not a knowledge gap. This is a will gap.
15. Why the Receptor Matters for the Ardis Argument
The single sentence summary: the α7-nicotinic acetylcholine receptor is a genuine therapeutic target, the cholinergic anti-inflammatory pathway is a genuine endogenous brake on inflammation, the structural biology of nAChR ligand binding can accommodate a 3FTx-loop / spike-RBD docking interaction, and nicotine occupies the same site that spike does. Every piece of that sentence is supported by mainstream peer-reviewed pharmacology. The therapeutic interpretation — that exogenous nicotine should blunt spike-mediated injury — is the inferential step.
The receptor pharmacology, by itself, is more than enough to justify clinical investigation of nicotine in early-symptomatic COVID, in post-vaccination syndromes, and in long-COVID. That investigation has been suppressed for political reasons that have nothing to do with pharmacology. That suppression, more than any specific therapeutic claim, is the indictment Ardis is making.
Key Research Papers
- Borovikova LV, Ivanova S, Zhang M, et al. Vagus nerve stimulation attenuates the systemic inflammatory response to endotoxin. Nature. 2000;405:458-462.
- Wang H, Yu M, Ochani M, et al. Nicotinic acetylcholine receptor α7 subunit is an essential regulator of inflammation. Nature. 2003;421:384-388.
- Olofsson PS, Rosas-Ballina M, Levine YA, Tracey KJ. Rethinking inflammation: neural circuits in the regulation of immunity. Immunol Rev. 2012;248(1):188-204.
- Bourne Y, Talley TT, Hansen SB, Taylor P, Marchot P. Crystal structure of a Cbtx-AChBP complex reveals essential interactions between snake α-neurotoxins and nicotinic receptors. EMBO J. 2005;24(8):1512-1522.
- Dellisanti CD, Yao Y, Stroud JC, Wang ZZ, Chen L. Crystal structure of the extracellular domain of nAChR α1 bound to α-bungarotoxin at 1.94 Å resolution. Nat Neurosci. 2007;10(8):953-962.
- Changeux JP, Amoura Z, Rey FA, Miyara M. A nicotinic hypothesis for COVID-19 with preventive and therapeutic implications. C R Biol. 2020;343(1):33-39.
- Lagoumintzis G, Chasapis CT, Alexandris N, et al. Nicotinic cholinergic system and COVID-19. Food Chem Toxicol. 2021;149:112009.
- Andersson U, Tracey KJ. Reflex principles of immunological homeostasis. Annu Rev Immunol. 2012;30:313-335.
PubMed Research Searches
- PubMed: α7 nicotinic receptor and macrophage
- PubMed: Cholinergic anti-inflammatory pathway and vagus
- PubMed: α7 receptor and endothelium
- PubMed: Three-finger toxin and nicotinic receptor
- PubMed: Varenicline and α7 receptor
- PubMed: Galantamine and α7 modulator
- PubMed: α7 nicotinic and T cells
- PubMed: Vagus nerve stimulation and rheumatoid arthritis
- PubMed: Nicotinic receptor and SARS-CoV-2 spike
Connections
- Snake-Venom Hypothesis
- Nicotine Hypothesis
- Dr. Bryan Ardis Hub
- COVID Lies Book
- Vaccine-Injury Recovery
- Nicotine Patch Protocol
- Tobacco Suppression History
- Detox and Recovery
- Hospital Protocol Critique
- Stress Management
- Immune Boosting
- Breathwork
- Gut-Brain Axis
- Choline
- Schizophrenia
- POTS Subtypes