Dr. Bryan Ardis: The Nicotine Hypothesis, COVID Lies & the Snake-Venom Theory
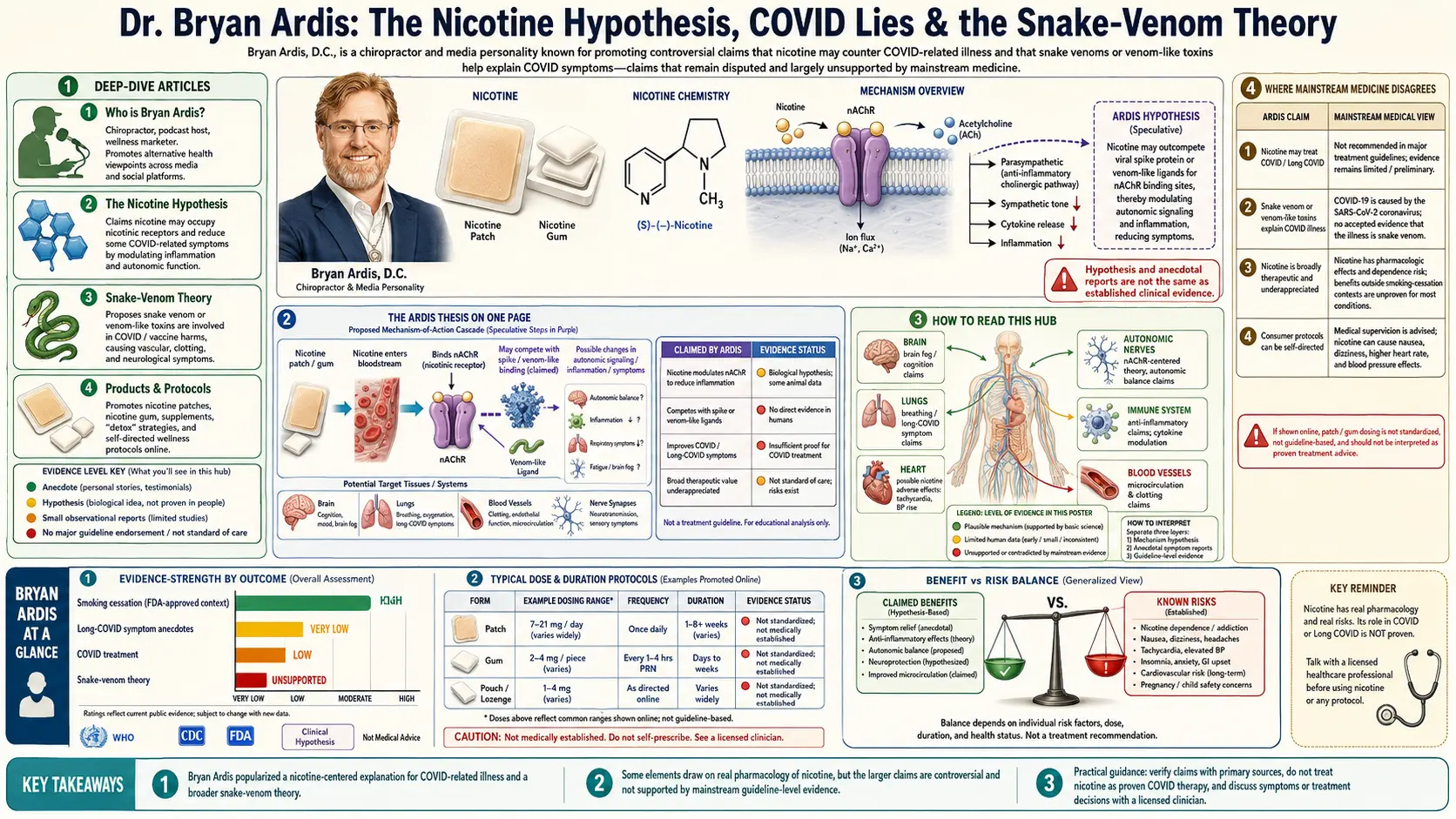


Dr. Bryan Ardis, DC is an Iowa-trained chiropractor and former nutrition-clinic director who emerged as a prominent independent researcher during the COVID-19 era. After his father-in-law’s death in a hospital ICU in 2020 — a death he came to attribute to remdesivir-induced kidney failure rather than the viral illness itself — Ardis began an extended public investigation into hospital protocols, vaccine injuries, and what he argues is a systematic suppression of low-cost therapeutic interventions. His most consequential and most contested public claim is the nicotine hypothesis: that nicotine, decoupled from the carcinogenic combustion byproducts of tobacco smoke, is a powerful, broadly protective antiviral and anti-inflammatory molecule whose therapeutic potential has been deliberately concealed in order to protect the global pharmaceutical and tobacco-control industries.
This hub is an extensive, sourced documentation of Ardis’s research, the arguments laid out in his book COVID Lies, and the broader ecosystem of clinicians, papers, and historical primary sources he draws on. We summarize the nicotine–nAChR receptor pharmacology that grounds his thesis in real biochemistry; the controversial “synthetic-venom-peptide” reading of the SARS-CoV-2 spike protein he advanced in 2022; his clinical protocols for hospital-injured and vaccine-injured patients; and his historical reading of tobacco as an indigenous medicine that was first commercialized, then demonized, then replaced by patent pharmaceuticals targeting the same receptor system. Ardis’s positions are heterodox and sit outside mainstream medical consensus in important places; we present them clearly, with citations to the primary literature where it exists, and with a labeled section identifying where peer-reviewed pharmacology already agrees with him and where it does not.
Deep-Dive Articles
Bryan Ardis’s body of work is wide-ranging — book, podcasts, conference talks, peer-reviewed citations, clinical protocols, and historical research. The nine articles below each take one strand of that work and unfold it in depth. Start with the COVID Lies book summary if you want the integrated argument, or jump straight to the Nicotine Hypothesis if you came here for the receptor pharmacology.
1. COVID Lies — The Book
A chapter-by-chapter summary of Ardis’s 2023 book COVID Lies: How the Top Doctors and Big Pharma Manipulated the Global Pandemic with Fraudulent PCR Tests, Deadly Hospital Protocols, Mandated Use of the Toxic Drug Remdesivir, and Mandated Toxic Vaccines. The remdesivir story, the Bourla pleadings, the mortality-protocol critique, and the integrated nicotine argument that ties the book together.
2. The Nicotine Hypothesis
The central thesis: nicotine binds nicotinic acetylcholine receptors (nAChRs) at the same site SARS-CoV-2 spike binds, blocks viral and toxin entry, lowers IL-6/TNF-α via the cholinergic anti-inflammatory pathway, and explains the “smoker’s paradox” in COVID hospitalization data — without committing the user to combustion-tobacco harms.
3. Nicotinic Acetylcholine Receptors (nAChRs)
The receptor pharmacology underneath the hypothesis: α7-nAChR distribution on neurons, alveolar macrophages, lymphocytes, and vascular endothelium; the cholinergic anti-inflammatory pathway (Tracey, Nature 2002); the Changeux/Pasteur 2020 nicotinic-hypothesis preprint; and why receptor-level antagonism is a more honest target than “immune support.”
4. The Synthetic-Venom-Peptide Hypothesis
Ardis’s most controversial 2022 claim, presented honestly: spike-protein/conotoxin/elapid-neurotoxin sequence homology, the published 3-finger-toxin literature he cites (Forsström, Lentz, Changeux), the reception in molecular biology, and the strong mainstream rebuttals. Why the receptor argument can stand even if the venom-peptide framing is rejected.
5. Nicotine Patch Protocol — Dosing & Sourcing
The practical layer: the 7 mg / 14 mg / 21 mg transdermal patch ladder used in Ardis’s recovery protocols, why he prefers patches over gum/lozenges, contraindications (pregnancy, unstable cardiac disease, adolescents, MAOI users), brand sourcing, and a clear taper schedule. This is documentation, not medical advice.
6. Vaccine-Injury Recovery Protocol
The full Ardis protocol stack for individuals reporting persistent post-vaccination symptoms: nicotine patches, NAC, vitamin C, melatonin, ivermectin (where legal/available), low-dose aspirin for microclot risk, dandelion-root extract, and structured detox phases. Side-by-side with the FLCCC I-RECOVER protocol for context.
7. Hospital Protocols & Remdesivir
The case against the early-pandemic standard of care that Ardis builds in COVID Lies: the ACTT-1 design, the WHO Solidarity trial result, the 33% AKI signal from VA pharmacovigilance, the ventilator-mortality numbers from Ichikado et al., and how CMS bonus payments (Cares Act) created perverse incentives around the 20% inpatient COVID add-on.
8. The Ardis Detox Layer
The complementary detox stack he layers on top of nicotine therapy: NAC for glutathione, dandelion-root extract for spike-protein binding (Tran 2021 preprint), pine-needle tea for shikimic acid, fenbendazole and ivermectin in the cancer/immunology layer, methylene blue for mitochondrial rescue, and his cautious view on chelation.
9. Tobacco, Indigenous Medicine & Suppression History
The historical layer: pre-Columbian Indigenous medicinal tobacco use, the Royal College of Physicians 2016 e-cigarette report, Surgeon-General Luther Terry’s 1964 framing, the FDA NRT pathway, and the parallel patent timeline of varenicline (Chantix), galantamine, and other nAChR-active drugs — the “why was nicotine left on the shelf?” argument central to Ardis’s historical case.
Who Is Dr. Bryan Ardis?
Bryan Ardis was born in Iowa and graduated from Parker University in Dallas with a Doctor of Chiropractic (DC) degree. Before COVID, his clinical practice — first in Dallas’s suburbs and later online — focused on chronic-pain rehabilitation, nutritional medicine, and what he describes as “orthomolecular protocols” for autoimmune disease and metabolic dysfunction. He was, by his own account, an entirely conventional alternative-medicine practitioner with no public profile until April 2020.
His pivot into pandemic research began with the death of his father-in-law, John C. Eyman, in a Texas hospital in late March 2020. Ardis has stated publicly that Eyman was admitted with a respiratory illness, was placed on a five-day course of remdesivir against the family’s objections, developed acute kidney injury (AKI) within 72 hours, was placed on mechanical ventilation, and died. The death certificate listed COVID-19; Ardis publicly argues the proximate cause was iatrogenic AKI from remdesivir. That experience generated the line of inquiry that became COVID Lies: if a $3,120 five-day course of an experimental antiviral was being administered with FDA Emergency Use Authorization despite a 33% acute-kidney-injury signal in pharmacovigilance data, what else was being done in the name of pandemic care that did not survive ordinary clinical scrutiny?
From that question, Ardis broadened his investigation into the FDA Emergency Use Authorization process, the early NIH treatment guidelines, the CARES Act’s 20% Medicare add-on for inpatient COVID admissions, the design of pivotal vaccine trials, and the receptor-pharmacology literature on nicotine and the nicotinic acetylcholine receptor. He launched The Dr. Ardis Show, a long-form interview podcast, in 2021. In 2022 he became internationally known for the Watch the Water documentary advancing the “synthetic-venom-peptide” reading of the SARS-CoV-2 spike protein. In 2023 he published COVID Lies through Skyhorse Publishing — the integrated written form of his pandemic-era research, summarized in detail in this hub’s book chapter.
Ardis is not a medical doctor and does not practice prescriptive medicine. His chiropractic license is in Texas. He runs a supplement company (Ardis Labs) that he uses to fund continued research and travel for speaking engagements; readers should keep that commercial relationship in mind when evaluating any specific product recommendation in his materials. The hub focuses on his arguments and the published literature behind them, not on supplement endorsements.
The Ardis Thesis on One Page
- SARS-CoV-2 spike binds nicotinic acetylcholine receptors (nAChRs). The spike receptor-binding domain shares structural homology with snake-venom three-finger toxins (3FTx) that are well-known nAChR antagonists. Multiple peer-reviewed papers (Farsalinos 2020, Changeux 2020, Lagoumintzis 2021) make a version of this claim with varying degrees of confidence.
- Nicotine occupies the same receptor. Nicotine is a high-affinity orthosteric agonist at α4β2 and α7 nAChRs. By saturating those receptors, nicotine can competitively block the spike-glycoprotein/receptor interaction and prevent the receptor-mediated phase of pathology — not the only mechanism of viral injury, but, in Ardis’s reading, the most under-recognized one.
- The cholinergic anti-inflammatory pathway is real. Vagal stimulation via α7-nAChR on macrophages potently suppresses IL-6 and TNF-α release (Tracey’s Nature work, 2000–2010). This is undisputed mainstream pharmacology. It explains, mechanistically, the persistent “smokers were under-represented in COVID ICUs” observational signal.
- The vaccine and the wild-type virus share the receptor target. Because the mRNA platforms generate spike protein endogenously, Ardis argues the same nAChR-mediated pathology can be a component of post-vaccination injury — and the same receptor occupant (nicotine) can be a component of recovery, alongside conventional detox and anti-inflammatory measures.
- Hospital standard-of-care optimized for billing, not survival. The remdesivir/ventilator combination produced exceptionally high inpatient mortality. Cheap, generic, off-patent agents (ivermectin, fluvoxamine, hydroxychloroquine, melatonin, vitamin D, zinc, and — centrally — nicotine) were systematically excluded from formularies in a way Ardis argues cannot be explained by clinical evidence alone.
- The nicotine taboo is a 60-year-old policy artifact. The 1964 Surgeon General report bundled nicotine with the carcinogens of combusted tobacco. That bundling has carried forward into the present day as a near-religious public-health prohibition on naming nicotine as a therapeutic, even as patent drugs targeting the same receptor (varenicline, galantamine) generate billions in revenue.
How to Read This Hub
Five reading paths through the nine sub-articles, depending on what brought you here:
- You want the integrated argument. Start with COVID Lies — The Book, then The Nicotine Hypothesis, then Hospital Protocols & Remdesivir.
- You came for the receptor pharmacology. Go straight to nAChRs, then The Nicotine Hypothesis. The 3-finger-toxin literature picks up in The Synthetic-Venom-Peptide Hypothesis.
- You or someone you love is dealing with a vaccine injury. The practical layer is Vaccine-Injury Recovery, supported by Patch Dosing & Sourcing and The Ardis Detox Layer. Read these alongside the FLCCC I-RECOVER protocol for context, and discuss with a clinician who works with post-vaccination patients.
- You are skeptical of the snake-venom framing. Read The Synthetic-Venom-Peptide Hypothesis first — including the rebuttals section — before deciding whether to engage with the rest. The receptor argument and the hospital-protocol argument do not depend on the venom-peptide framing being correct.
- You want the historical and political case. Tobacco, Indigenous Medicine & Suppression History stands alone as a long-form essay on how a multi-purpose Indigenous medicine became a pharmaceutical taboo over the course of two centuries.
Where Mainstream Pharmacology Already Agrees
- Nicotine is a high-affinity nAChR agonist. This is undergraduate pharmacology, not a contested point.
- The cholinergic anti-inflammatory pathway exists and is therapeutically relevant. Tracey’s vagus-nerve work (Borovikova et al., Nature 2000; Wang et al., Nature 2003) is uncontroversial, has spawned an entire bioelectronic-medicine industry (SetPoint Medical, Galvani Bioelectronics), and has been replicated in dozens of laboratories.
- The α7-nAChR is expressed on alveolar macrophages, T cells, and pulmonary endothelium — the exact tissues SARS-CoV-2 targets.
- The “smoker’s paradox” observation is real in the early-pandemic data. Active smokers were under-represented among hospitalized COVID patients in multiple early French and Chinese cohorts (Miyara 2020, Farsalinos 2020 meta-analysis) — though the interpretation, particularly after adjustment for age and comorbidity, has been hotly debated.
- Remdesivir produces a dose-related signal of acute kidney injury in WHO Uppsala VigiBase pharmacovigilance data; the WHO Solidarity trial showed no mortality benefit (Pan et al., NEJM 2021).
- Three-finger-toxin / nAChR pharmacology is a long-established structural biology field with crystallographic data going back to Bourne & Taylor 2005 and Dellisanti 2007.
Where Mainstream Medicine Disagrees
- On the “synthetic-venom-peptide” framing of SARS-CoV-2 spike. Mainstream virology accepts that some 3FTx structural motifs appear in receptor-binding domains broadly, but rejects Ardis’s further claim that the virus or vaccine spike is, in any meaningful sense, “snake venom” or that the water supply was contaminated with venom peptides. The dedicated page reproduces both sides honestly.
- On nicotine as a primary therapeutic for COVID. A small randomized controlled trial of nicotine patches in hospitalized COVID-19 patients (NICOVID, Tombé et al., 2023) was negative for the primary endpoint of mortality reduction. Ardis argues that hospitalized patients are too far down the inflammatory cascade for nAChR antagonism to rescue, and that the appropriate trial would be early outpatient or pre-exposure use. Mainstream rebuttal: that argument is post-hoc.
- On the safety of nicotine outside combustion. Public-health authorities continue to treat all nicotine exposure as harmful and addictive. The Royal College of Physicians 2016 report and the UK NHS “Stoptober” e-cigarette campaign represent a more nuanced view, but the dominant U.S. position (FDA, CDC, WHO MPOWER framework) remains a precautionary one.
- On vaccine-injury attribution. The clinical reality of post-vaccination chronic illness is increasingly recognized in the peer-reviewed literature (the NIH’s post-acute sequelae work, Yale LISTEN, the Couzin-Frankel Science 2022 reporting), but the size and mechanism are debated and the FDA does not endorse Ardis’s integrated protocol.
Anyone considering a nicotine-based therapy on the basis of this material should discuss it with a clinician who is familiar with both nAChR pharmacology and their own medical history. Pregnancy, unstable coronary disease, recent stroke, uncontrolled hypertension, and adolescence (developing brain) are absolute or near-absolute contraindications to exogenous nicotine. The Patch Protocol page lays them out in detail.
Foundational Research Papers
- Borovikova LV, Ivanova S, Zhang M, Yang H, Botchkina GI, Watkins LR, Wang H, Abumrad N, Eaton JW, Tracey KJ. Vagus nerve stimulation attenuates the systemic inflammatory response to endotoxin. Nature. 2000;405(6785):458-62.
- Wang H, Yu M, Ochani M, et al. Nicotinic acetylcholine receptor α7 subunit is an essential regulator of inflammation. Nature. 2003;421(6921):384-8.
- Farsalinos K, Niaura R, Le Houezec J, Barbouni A, Tsatsakis A, Kouretas D, Vantarakis A, Poulas K. Editorial: Nicotine and SARS-CoV-2: COVID-19 may be a disease of the nicotinic cholinergic system. Toxicology Reports. 2020;7:658-663.
- Changeux JP, Amoura Z, Rey FA, Miyara M. A nicotinic hypothesis for COVID-19 with preventive and therapeutic implications. Comptes Rendus Biologies. 2020;343(1):33-39.
- Lagoumintzis G, Chasapis CT, Alexandris N, Kouretas D, Tzartos S, Eliopoulos E, Farsalinos K, Poulas K. Nicotinic cholinergic system and COVID-19: In silico identification of an interaction between SARS-CoV-2 and nicotinic receptors with potential therapeutic targeting implications. Food and Chemical Toxicology. 2021;149:112009.
- WHO Solidarity Trial Consortium. Pan H, Peto R, Henao-Restrepo AM, et al. Repurposed antiviral drugs for Covid-19 — Interim WHO Solidarity Trial Results. N Engl J Med. 2021;384(6):497-511.
- Couzin-Frankel J. Long Covid clues emerge from worldwide research effort. Science. 2022.
Connections
- Vaccine-Injury Recovery
- Nicotine Hypothesis
- Snake-Venom Hypothesis
- Nicotinic Acetylcholine Receptors
- Detox and Recovery
- COVID Lies Book
- Nicotine Patch Protocol
- Tobacco Suppression History
- Hospital Protocol Critique
- NAC (N-Acetylcysteine)
- Methylene Blue
- Fenbendazole
- Zinc
- Vitamin C
- Morley Robbins (Root Cause Protocol)
- Gerson Therapy
- Immune Boosting
- Detox Protocols