Tobacco, Indigenous Medicine & the 60-Year Suppression of Therapeutic Nicotine
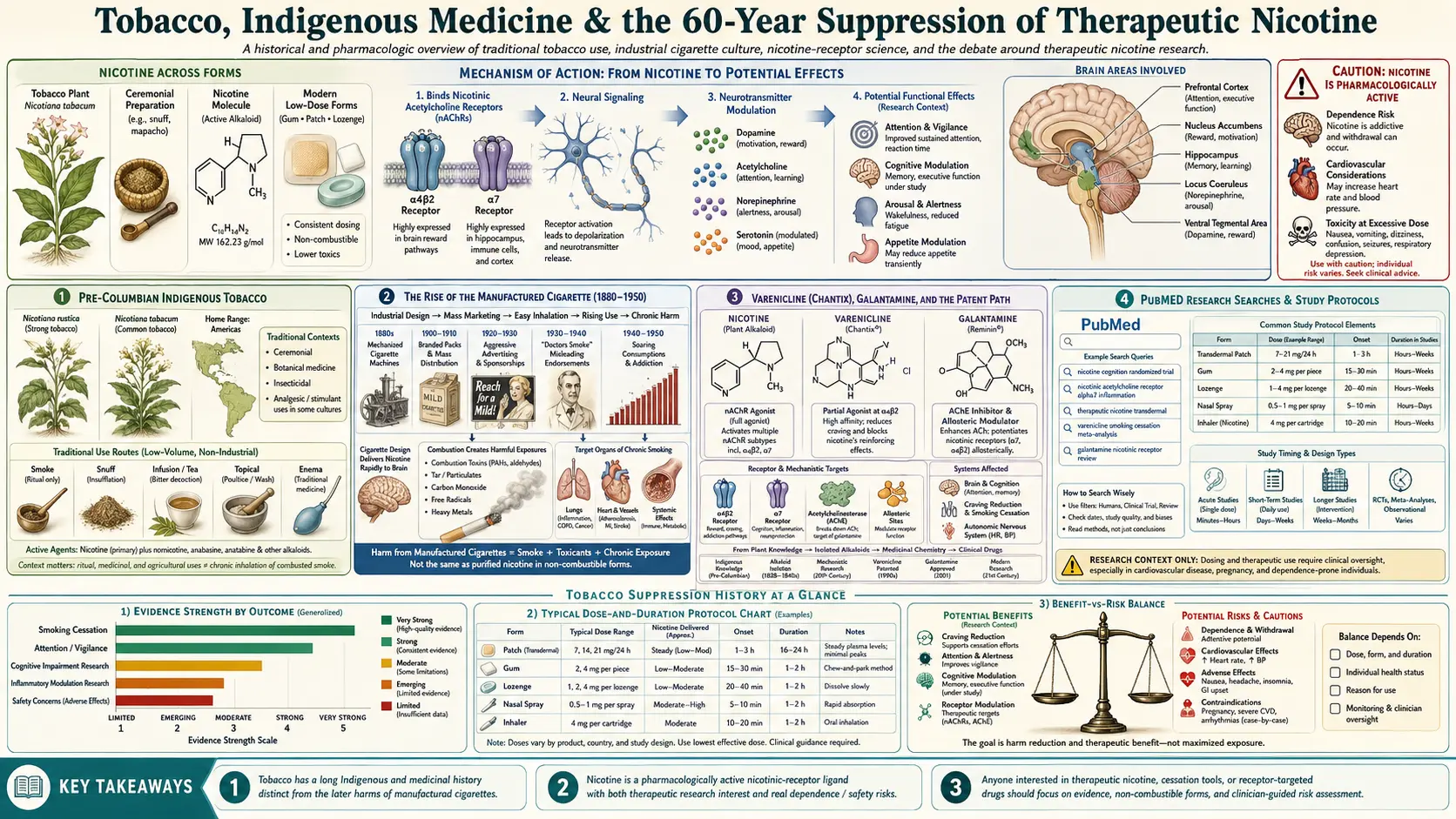
Table of Contents
- Pre-Columbian Indigenous Tobacco
- The European Arrival and Early Medical Tobacco (1492–1700)
- Enlightenment Pharmacy: Tobacco as Materia Medica
- The Nicotiana Genus and Its Subspecies
- Nicotine Isolated — Posselt and Reimann, 1828
- The Rise of the Manufactured Cigarette (1880–1950)
- The Carcinogenic Discovery and the 1964 Surgeon General Report
- The Conceptual Bundling of Nicotine with Combustion
- The NRT Paradox: Approved Nicotine When You’re Quitting Tobacco
- Varenicline (Chantix), Galantamine, and the Patent Path
- The Royal College of Physicians 2016 Report
- Snus, Pouches, and Tobacco Harm Reduction
- The Suppression Argument
- What Restoration Would Look Like
- Key Research Papers & Documents
- PubMed Research Searches
- Connections
- Featured Videos
1. Pre-Columbian Indigenous Tobacco
Tobacco (Nicotiana spp.) was domesticated in the Americas at least 8,000 years ago. By the time of European contact, tobacco was a sacred and medicinal plant across virtually every Indigenous nation of North, Central, and South America. The medicinal applications documented in the ethnobotanical record:
- Respiratory medicine: chewed leaves and decoctions for asthma, cough, congestion. The Maya, Aztec, and Mississippian cultures all used tobacco in respiratory remedies.
- Anti-parasitic: external paste for skin parasites, internal preparations for intestinal worms.
- Wound healing: poultice and topical application; the antibacterial and vasoconstrictor effects of nicotine support this in retrospect.
- Pain management: chewed and inhaled forms for toothache, headache, neuralgia.
- Ceremonial / cognitive: tobacco as a sacred plant connecting the human and spirit worlds, used in carefully prescribed ceremonial contexts.
The traditional ceremonial use was distinct from recreational consumption. Tobacco was a powerful plant-medicine handled with respect, used in measured doses, and integrated into a framework of prayer, healing, and community ritual. The mass-market cigarette is a 19th-century industrial product that has almost nothing in common with the Indigenous ceremonial pipe.
2. The European Arrival and Early Medical Tobacco (1492–1700)
Columbus’s 1492 expedition was the first documented European contact with tobacco. Within decades, the plant had been carried to Europe, and by the mid-1500s it was being grown and prescribed across the continent as a wonder medicine.
- Jean Nicot (1530–1600), French ambassador to Portugal, sent tobacco seeds and dried leaf to the French court in 1559–1560 as a treatment for the migraines of Catherine de’ Medici. The genus Nicotiana takes its name from him.
- Nicolás Monardes, a Spanish physician in Seville, published Historia medicinal de las cosas que se traen de nuestras Indias Occidentales (1565–1574), praising tobacco for asthma, headache, kidney stones, joint pain, and a long list of other conditions. The book was widely translated and shaped European medical practice for two centuries.
- The Royal College of Physicians of London in the 17th century included tobacco in its Pharmacopoeia Londinensis as an officially recognized medicine.
- Plague doctors across Europe smoked or chewed tobacco both as a presumed prophylactic against the “miasma” of plague and as an antiseptic.
For more than 200 years, tobacco was Europe’s default herbal medicine for respiratory and inflammatory conditions. The medical-tobacco era was longer than the cigarette-as-public-health-disaster era has yet been.
3. Enlightenment Pharmacy: Tobacco as Materia Medica
By the 18th and early 19th centuries, tobacco appeared in major pharmacopoeias across Europe and the Americas as a recognized agent in the materia medica. Recommended uses included:
- Tobacco-smoke enemas for cardiopulmonary resuscitation of drowning victims (the original meaning of “blowing smoke up someone’s ass” was a literal medical procedure)
- Tobacco poultices for inflammation and abscesses
- Tobacco infusions for asthma and bronchitis
- Topical tobacco for skin conditions and parasites
- Internal preparations (in carefully limited doses) for cardiac dysrhythmias
The understanding that tobacco was a powerful, dose-dependent agent — medicinal at low dose, toxic at high dose — was widely held in the medical literature of the period. The cigarette had not yet been invented.
4. The Nicotiana Genus and Its Subspecies
The genus Nicotiana contains approximately 75 species, of which two are commercially significant:
- Nicotiana tabacum: the dominant commercial species, originally from South America, now the source of essentially all global cigarette tobacco.
- Nicotiana rustica: an older Indigenous variety with substantially higher nicotine content (10–18% by dry weight, vs. 1–3% in tabacum), still used in traditional ceremonies. Sometimes called “Aztec tobacco” or “mapacho.”
- Other species: ornamental Nicotianas (N. alata, N. sylvestris) with low nicotine; Nicotiana glauca with the toxic alkaloid anabasine instead of nicotine; Nicotiana attenuata the wild U.S. southwestern species.
The shift from traditional Indigenous use of N. rustica in ceremonial contexts to industrial use of N. tabacum in recreational cigarettes is a substantial shift in both species and context. The Ardis case is, in part, that the public-health critique of cigarettes has been allowed to extend through the genus into the molecule itself, a confusion of taxonomy with pharmacology.
5. Nicotine Isolated — Posselt and Reimann, 1828
Nicotine was first isolated as a pure compound in 1828 by the German chemists Wilhelm Heinrich Posselt and Karl Ludwig Reimann at the University of Heidelberg. The discovery decoupled, for the first time, the active alkaloid from the leaf and the smoke. From 1828 onward, it was scientifically possible to study nicotine itself, separately from any specific consumption pathway. This is the moment from which the modern nicotinic-receptor pharmacology eventually grew.
By the late 19th century, nicotine had been characterized as the agent responsible for tobacco’s rapid effects on heart rate, mood, and cognition. The receptor that bound it — the nicotinic acetylcholine receptor — was identified pharmacologically by John Newport Langley around 1900, and isolated as a protein by Jean-Pierre Changeux in the 1970s. The same Changeux who would, in 2020, propose a nicotinic hypothesis for COVID-19.
6. The Rise of the Manufactured Cigarette (1880–1950)
The pre-modern tobacco-consumption pattern was the pipe, the cigar, the chew, and the snuff. Each of these delivers tobacco at a relatively slow rate, with relatively low daily nicotine intake, and (importantly) with relatively low pulmonary penetration of combustion byproducts. The manufactured cigarette is a different product entirely.
- 1881: James Bonsack’s cigarette-rolling machine industrialized cigarette production.
- 1900–1920: mass-marketing of cigarettes to civilian and military populations. The packed-paper combustion vehicle delivered nicotine deep into the alveoli at speeds incomparable to any traditional preparation.
- WWI and WWII: military cigarette rations turned a generation of soldiers into nicotine-dependent consumers. Returning veterans drove the post-war consumption boom.
- 1950s: peak cigarette consumption in the United States. ~50% of adult men, ~30% of adult women smoking.
The cigarette is a delivery system optimized for combustion-product penetration into the lung. The Indigenous ceremonial pipe is not. Lumping these two things together as “tobacco use” is the conceptual move that the 1964 Surgeon General report cemented and that the public-health establishment has not unmade.
7. The Carcinogenic Discovery and the 1964 Surgeon General Report
The epidemiological discovery of cigarette–cancer association is one of the great public-health victories of the 20th century:
- Doll & Hill (1950): case-control study in BMJ showing strong association between cigarette smoking and lung cancer.
- Doll & Hill British Doctors Study (1956 onward): prospective cohort confirming dose-response relationship.
- Wynder & Graham (1953): tar painting on mice produced tumors, confirming the chemical-carcinogen mechanism.
- 1964 Surgeon General report (Luther Terry, MD, U.S. Surgeon General): formal U.S. government statement that “cigarette smoking is causally related to lung cancer in men.”
The 1964 report was, on its narrow target, correct. Cigarette smoking does cause lung cancer. The harm is from the combustion products: tar, polycyclic aromatic hydrocarbons, tobacco-specific nitrosamines (NNK, NNN, NAT), heavy metals, and a long list of carcinogens that form when plant material is burned at >600 °C.
The report did not, however, distinguish between nicotine and the combustion products. That elision became the foundation of 60 years of policy.
8. The Conceptual Bundling of Nicotine with Combustion
From 1964 onward, U.S. public-health discourse has treated nicotine and combustion-tobacco as a single entity. Examples:
- The FDA assertion of jurisdiction over nicotine as a “drug delivery device” in cigarettes (the 2009 Tobacco Control Act).
- The CDC framing of all nicotine exposure as harmful in young people (the e-cigarette “EVALI” episode of 2019, where vitamin-E-acetate-containing illegal THC vapes were responsible for the lung injuries but vaping nicotine was bundled with them in messaging).
- The WHO MPOWER framework treating any tobacco-derived nicotine product the same as combustion cigarettes.
- School-based prevention messaging that “nicotine is addictive and harmful” without distinguishing combustion from non-combustion delivery.
The Ardis observation: this bundling is not science. It is policy-as-science. The molecule of nicotine, in non-combustion delivery, has a profile that bears almost no relationship to the cigarette–cancer relationship. Forty years of nicotine-replacement-therapy use as a smoking-cessation tool have not produced a cancer signal. That fact is, in the framework of public-health messaging, somehow always treated as not falsifying the “nicotine is harmful” bundle.
9. The NRT Paradox: Approved Nicotine When You’re Quitting Tobacco
The single most absurd feature of the regulatory landscape: nicotine itself is FDA-approved as an over-the-counter consumer product in three forms (patch, gum, lozenge) when used to help smokers quit smoking. Therapeutic nicotine for tobacco cessation is uncontroversial. Therapeutic nicotine for any other indication — ulcerative colitis (where it works), Alzheimer’s (where the trials are mixed), COVID-19 (where Changeux published a hypothesis) — is, somehow, simultaneously dangerous, untested, and irresponsible.
The same molecule, the same delivery vehicle, the same plasma concentration. The regulatory difference is the indication. The framework is internally inconsistent and the inconsistency is doing political work.
10. Varenicline (Chantix), Galantamine, and the Patent Path
The pharmaceutical industry, meanwhile, has built a substantial business on nAChR-active drugs — just not on nicotine itself.
- Varenicline (Chantix, Pfizer): α4β2 partial agonist for smoking cessation. Approved 2006. Peak revenue ~$1.1 billion. Same receptor as nicotine.
- Galantamine (Razadyne, Janssen): AChE inhibitor + α7-nAChR positive allosteric modulator. Approved for Alzheimer’s. Same receptor as nicotine.
- Donepezil (Aricept): AChE inhibitor that raises synaptic acetylcholine to engage nAChRs and muscarinic receptors. Approved for Alzheimer’s.
- Encenicline, ABT-126: α7-selective partial agonists in development for Alzheimer’s and schizophrenia. Same receptor as nicotine.
The pharmacology is unambiguous: pharma believes nAChRs are a real therapeutic target and will develop and patent novel agonists at considerable expense to engage them. What pharma will not do is run a Phase III trial of low-cost transdermal nicotine in any indication where the receptor pharmacology predicts benefit, because the molecule is not patentable. The pattern is consistent with the Ardis suppression hypothesis without requiring any cinematic conspiracy: it is just the natural behavior of a patent-driven industry.
11. The Royal College of Physicians 2016 Report
The most important official document on the modern pharmacology of nicotine is the Royal College of Physicians 2016 report, “Nicotine without smoke: Tobacco harm reduction.” Published by the United Kingdom’s oldest medical college, founded 1518, the report stated unambiguously:
“Although nicotine is the addictive component of tobacco smoke, it is not a major cause of smoking-related diseases. Most of the harm from tobacco smoking arises from the combustion products in smoke, not from nicotine itself. Smoke, not nicotine, is the killer.”
The RCP report endorsed e-cigarettes as a tobacco-harm-reduction tool and called for a regulatory framework that recognized the very large difference between nicotine-as-molecule and tobacco-as-combusted-product. The position was endorsed by Public Health England, the UK NHS, and the British Medical Association.
The U.S. public-health establishment has not adopted this framing. The CDC, FDA, and most state public-health agencies continue to treat all nicotine exposure as a uniform harm. The transatlantic divergence on this question is itself a useful window into the institutional blindspot.
12. Snus, Pouches, and Tobacco Harm Reduction
The Swedish experience is the strongest empirical case for the molecule-vs-combustion distinction:
- Snus: a moist, smokeless oral tobacco product placed under the upper lip. Used by ~20% of Swedish adult men. EU-banned outside Sweden, where it has a special exemption.
- Outcome data: Swedish men have one of the highest rates of nicotine use in Europe and one of the lowest rates of tobacco-related cancer. The “Swedish paradox” is a real population-level signal that combustion, not nicotine, is the carcinogen.
- Modern oral pouches (Zyn, Velo, On!, etc.): tobacco-free nicotine pouches that deliver pure nicotine sublingually without any tobacco leaf or combustion. The market segment is the fastest-growing in the U.S. tobacco-equivalent space and is essentially a real-world version of the Ardis “nicotine without combustion” argument.
The Swedish epidemiological data are not contested. They are simply not centered in U.S. policy. The Royal College of Physicians position and the Swedish snus data, taken together, constitute a working empirical case that nicotine-without-combustion is a quantitatively different exposure from cigarette smoking. The policy framework that treats them as equivalent is choosing to ignore the data.
13. The Suppression Argument
The Ardis suppression argument, in its strongest form:
- Nicotine is a high-affinity nAChR agonist with established therapeutic effects in ulcerative colitis (Pullan 1994), with strong supporting evidence in Alzheimer’s (Newhouse 2012), Parkinson’s (Quik laboratory), schizophrenia self-medication, and a serious receptor-pharmacology case in COVID-19 (Changeux 2020, Farsalinos 2020).
- Patent law incentivizes drug development away from off-patent molecules. Nicotine, in pharmaceutical-industry terms, has zero molecule-development incentive.
- Public-health policy, post-1964, has framed nicotine as inseparable from combustion tobacco, creating cultural and regulatory obstacles to trialing the molecule in non-combustion delivery for non-cessation indications.
- The combination of (2) and (3) is the suppression mechanism. It is not a conspiracy in the cinematic sense. It is the predictable equilibrium of a patent-driven pharmaceutical industry in a public-health framework that bundles molecule with combustion.
- The cost of this equilibrium has been a sixty-year freeze on a therapeutic molecule that the receptor pharmacology says deserves serious investigation in multiple indications. The COVID era is the most acute case but not the only one.
Restoration of therapeutic nicotine to its proper place in the pharmacopoeia requires unbundling the molecule from combustion in policy and discourse, funding non-industry trials of nicotine in candidate indications, and recognizing that “nicotine is harmful in adolescents” and “therapeutic nicotine is appropriate in adults with documented indications” can both be true.
14. What Restoration Would Look Like
A proper restoration of nicotine to the medical toolkit would include:
- Federally funded Phase III trials of transdermal nicotine in: early-symptomatic COVID-19; long-COVID; post-vaccination syndrome; refractory ulcerative colitis; mild cognitive impairment; ADHD-comorbid cognitive impairment.
- Repeal or modification of state-level FDA preemption that prevents physicians from prescribing nicotine for off-label indications without licensure threat.
- Public-health messaging that distinguishes nicotine-the-molecule from cigarettes-the-combustion-product.
- Recognition of Indigenous medicinal-tobacco traditions as part of the public ethnobotanical record and the history of receptor pharmacology.
- Reversal of the conceptual bundling that allowed Indian-Health-Service patients in the U.S. to be told that ceremonial tobacco is the same as Pall Mall cigarettes — an extension of public-health overreach into Indigenous cultural sovereignty that has not been honestly evaluated.
The Ardis case ends here, in the policy implications. Whatever the outcome of the synthetic-venom-peptide debate, the historical and pharmacological case for therapeutic nicotine deserves to stand on its own. That is the conversation COVID Lies is trying to make possible.
Key Research Papers & Documents
- Royal College of Physicians (London). Nicotine without smoke: Tobacco harm reduction. 2016.
- Pullan RD, Rhodes J, Ganesh S, et al. Transdermal nicotine for active ulcerative colitis. N Engl J Med. 1994;330(12):811-815.
- Newhouse P, Kellar K, Aisen P, et al. Nicotine treatment of mild cognitive impairment. Neurology. 2012;78(2):91-101.
- Changeux JP, Amoura Z, Rey FA, Miyara M. A nicotinic hypothesis for COVID-19. C R Biol. 2020;343(1):33-39.
- Farsalinos K, Niaura R, Le Houezec J, et al. Nicotine and SARS-CoV-2. Toxicology Reports. 2020;7:658-663.
- Borovikova LV, Ivanova S, Zhang M, et al. Vagus nerve stimulation attenuates the systemic inflammatory response to endotoxin. Nature. 2000;405:458-462.
- Doll R, Hill AB. Smoking and carcinoma of the lung; preliminary report. BMJ. 1950;2(4682):739-748.
- Mayer B. How much nicotine kills a human? Arch Toxicol. 2014;88(1):5-7.
PubMed Research Searches
- PubMed: Tobacco history and medicine
- PubMed: Indigenous tobacco and ceremonial use
- PubMed: Snus, cancer, and Sweden
- PubMed: Nicotine and therapeutic indications
- PubMed: Tobacco harm reduction
- PubMed: Varenicline and α7
- PubMed: Nicotine and ulcerative colitis
- PubMed: Galantamine and nicotinic receptor
Connections
- Dr. Bryan Ardis Hub
- Snake-Venom Hypothesis
- COVID Lies Book
- Vaccine-Injury Recovery
- Nicotine Hypothesis
- Nicotine Patch Protocol
- Detox and Recovery
- Nicotinic Acetylcholine Receptors
- Hospital Protocol Critique
- Gerson Therapy
- Morley Robbins (Root Cause Protocol)
- Cancer
- Ulcerative Colitis
- Asthma
- Post-Viral Triggers (CFS/ME)
- Schizophrenia