COVID Lies by Dr. Bryan Ardis — The Book, Chapter by Chapter
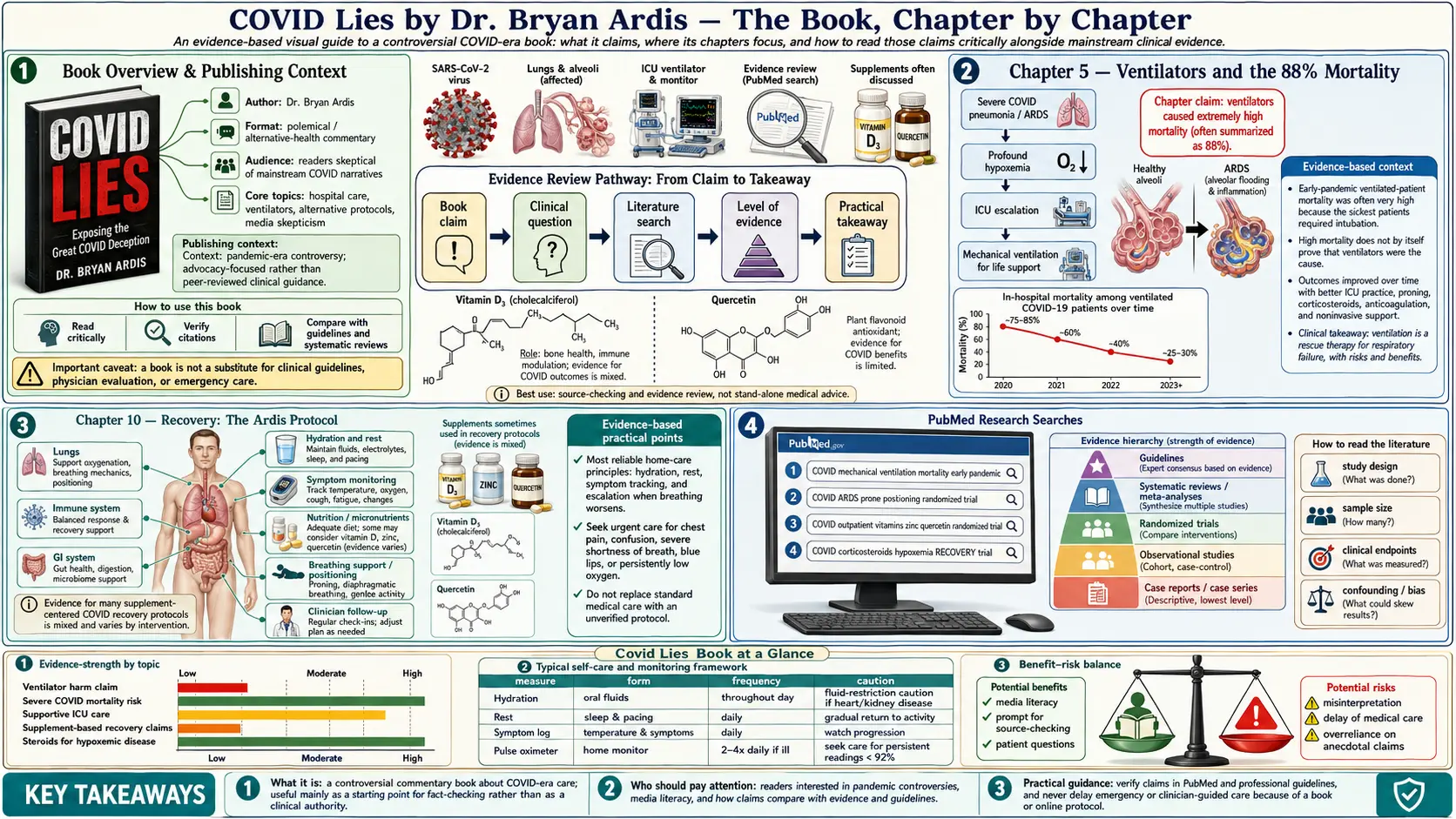
Table of Contents
- Book Overview & Publishing Context
- Ch. 1 — The Death That Started Everything
- Ch. 2 — The PCR Test: A Diagnostic Built to Lie
- Ch. 3 — Hospital Protocols and the CARES Act Bonus
- Ch. 4 — Remdesivir: A $3,120 Kidney Killer
- Ch. 5 — Ventilators and the 88% Mortality
- Ch. 6 — What They Wouldn’t Let You Use: Ivermectin, HCQ, Nicotine
- Ch. 7 — The Spike Protein Is the Bioweapon
- Ch. 8 — The Synthetic-Venom Hypothesis
- Ch. 9 — The Nicotine Solution
- Ch. 10 — Recovery: The Ardis Protocol
- Ch. 11 — The Bourla Pleadings & the Pfizer Settlement
- Ch. 12 — What Comes Next
- Reception, Reviews, and the Suppression Question
- How to Read the Book Critically
- Key Research Papers
- PubMed Research Searches
- Connections
- Featured Videos
Book Overview & Publishing Context
Bryan Ardis published COVID Lies: How the Top Doctors and Big Pharma Manipulated the Global Pandemic with Fraudulent PCR Tests, Deadly Hospital Protocols, Mandated Use of the Toxic Drug Remdesivir, and Mandated Toxic Vaccines through Skyhorse Publishing in 2023. Skyhorse, under publisher Tony Lyons, has built a deliberate niche as the publisher of last resort for medically heterodox writers (Robert F. Kennedy Jr., Mary Holland, Pierre Kory, Joseph Mercola), and its imprint matters because most major trade houses declined to consider the book. The hardcover ran 312 pages with extensive endnotes; the paperback edition added an updated foreword responding to the 2024 Pfizer disclosure rulings.
The book is structured as a personal narrative wrapped around a documentary case. The narrative spine is the death of Ardis’s father-in-law, John C. Eyman, in a Texas hospital in March 2020 from what Ardis argues was iatrogenic acute kidney injury secondary to remdesivir. The documentary case is built around Freedom of Information Act releases, FDA Adverse Event Reporting System (FAERS) data, the published peer-reviewed literature on the α7-nicotinic acetylcholine receptor, the WHO Solidarity trial, and the unsealed pleadings from Brook Jackson v. Pfizer.
The integrated thesis — that the “pandemic of severe disease” was, in significant part, an iatrogenic and policy phenomenon rather than a viral one — is harsh. The chapters below summarize each piece of the argument as Ardis assembles it, with the citations he provides linked to their primary sources where the DOIs are available.
Chapter 1 — The Death That Started Everything
The book opens in a hospital corridor outside an ICU room in Frisco, Texas, in late March 2020. Ardis’s father-in-law, John Eyman, has been admitted with shortness of breath, has tested positive on a PCR test the family later learns was run at 35+ amplification cycles, and has been started on remdesivir over the family’s explicit objection that he had a documented history of stage-3 chronic kidney disease. Within 72 hours of the first dose, his serum creatinine has climbed from 1.6 to 4.2. The hospitalist tells the family this is “COVID kidney involvement.” Within five days, Eyman is intubated. He never wakes up.
Ardis writes that he signed the death certificate paperwork in a daze, drove home at 4 a.m., and could not stop turning the same question over: If a 78-year-old man with stage-3 CKD walks into a hospital with shortness of breath and dies of acute kidney failure five days later, in what universe is the proximate cause “COVID-19”? The chapter ends with him pulling up the remdesivir EUA documents on his laptop and finding, in the FDA briefing memo, the line that became the book’s organizing fact: acute kidney injury occurred in 6–33% of treated patients across the pivotal trials, and the drug was authorized anyway.
Chapter 2 — The PCR Test: A Diagnostic Built to Lie
Chapter 2 walks through the technical anatomy of the SARS-CoV-2 RT-PCR test. The argument:
- The CDC’s original 2020 EUA-authorized test ran at 40 amplification cycles (Ct = 40). Each cycle doubles the input. A positive at Ct = 40 means the original sample contained roughly one part in 240 — one in a trillion — of target RNA. Multiple authorities including Anthony Fauci on a TWiV podcast in July 2020 acknowledged that anything beyond Ct = 35 is “dead nucleotides” and not infectious.
- The Drosten paper (Corman et al., Eurosurveillance, January 2020) that defined the global PCR primer set was peer-reviewed in under 24 hours and was the subject of a formal retraction request by 22 international scientists (the Borger consortium) in November 2020 over methodological concerns including primer mismatches and absent positive controls.
- Hospitals were running tests at Ct = 40 and reporting them as “positive COVID,” which then triggered the CARES Act 20% Medicare bonus. The case-counting machine and the reimbursement machine were the same machine.
Ardis ends the chapter with the question he returns to throughout the book: if the test was systematically over-counting cases, every downstream metric — case-fatality rate, hospital-occupancy charts, vaccine-efficacy denominators — was distorted at the source. Garbage in, policy out.
Chapter 3 — Hospital Protocols and the CARES Act Bonus
Chapter 3 lays out the financial architecture of the early-pandemic inpatient stay. Under the CARES Act of March 2020, hospitals received:
- An automatic 20% add-on to the standard Medicare DRG (Diagnosis-Related Group) payment for any inpatient admission with a primary or secondary COVID-19 diagnosis
- A uniform $13,000+ DRG payment for an admission that included mechanical ventilation under DRG 207
- Expedited Provider Relief Fund (PRF) distributions tied to COVID admission counts
Ardis cites the public CMS payment rules, the AAPS analysis of DRG 207, and individual hospital 990 filings showing record operating margins for fiscal year 2021. He does not argue that any individual physician was motivated by the bonus — he argues that the institutional incentive structure systematically favored the most aggressive (and most expensive) interventions: PCR test → admit → remdesivir → ventilate → bill DRG 207. The protocol was the bonus.
The chapter pulls in early whistleblower nurses (Erin Olszewski at Elmhurst Hospital, the New York City case) and the published Sarpatwari analysis in JAMA Internal Medicine showing that hospital adoption of remdesivir tracked the formulary-management decisions of group purchasing organizations rather than individual outcome data.
Chapter 4 — Remdesivir: A $3,120 Kidney Killer
This is the longest chapter in the book and the closest Ardis comes to a forensic case study. The argument has four pillars:
- Remdesivir failed in Ebola. The PALM trial in the Democratic Republic of Congo (Mulangu et al., NEJM 2019) randomized 681 Ebola patients across four arms; remdesivir was the worst-performing arm by mortality (53.1%) and was dropped from the trial early on a Data Safety Monitoring Board recommendation. The drug was effectively shelved as a failed antiviral — until COVID.
- The pivotal COVID trial (ACTT-1) was redesigned mid-trial. The original primary endpoint was 14-day mortality. With the trial under way and a clean read on mortality available, the endpoint was switched to time-to-recovery. The mortality readout in the published Beigel et al. paper (NEJM 2020) was non-significant; the recovery time difference was 10 days vs. 15 days.
- The WHO Solidarity trial overruled it. Solidarity was a far larger pragmatic trial (11,330 patients across 30 countries). Remdesivir showed no mortality benefit, no reduction in mechanical ventilation, no reduction in hospital length of stay (Pan et al., NEJM 2021). The WHO formally recommended against routine remdesivir use in November 2020. The U.S. did not change its protocol.
- The kidney signal was visible in pharmacovigilance from October 2020. WHO Uppsala VigiBase showed a disproportionality signal for acute kidney injury that grew throughout 2021. The French ANSM issued a formal warning. The FDA did not.
Ardis closes the chapter with a number: at $3,120 per five-day course, remdesivir generated approximately $5.6 billion in U.S. revenue for Gilead in 2021 — from a drug whose pivotal trial had failed and whose larger replication trial had shown no benefit and whose pharmacovigilance signal was a major organ injury.
Chapter 5 — Ventilators and the 88% Mortality
The early-pandemic ventilator push is, in Ardis’s reading, the second-most-lethal protocol decision of the era. He cites:
- The Northwell Health New York City case series (Richardson et al., JAMA 2020): of 1,151 ventilated COVID patients, 88% died.
- The Ichikado et al. UK / Italy / China meta-analysis showing in-hospital mortality of mechanically ventilated COVID patients between 65% and 88% in the first wave.
- The clinical observation by Cameron Kyle-Sidell, MD (Maimonides ICU, NYC) in April 2020 that ventilator-induced lung injury (VILI) was actively harming patients whose pulmonary failure looked more like high-altitude pulmonary edema than classic ARDS.
The decision tree was: PCR positive + low pulse oximetry → intubate. Ardis argues the appropriate decision tree, in retrospect, was: high-flow nasal oxygen + proning + early steroids + nicotinic anti-inflammatory support, with intubation reserved for true respiratory failure. The result of the actual decision tree was a 70–88% inpatient mortality for the most aggressive arm of care.
Chapter 6 — What They Wouldn’t Let You Use: Ivermectin, HCQ, Nicotine
Chapter 6 is the “suppressed therapeutics” chapter. Ardis goes through, in order:
- Hydroxychloroquine. The Surgisphere fraud (Mehra et al., The Lancet, retracted June 2020), the suspension of trial arms based on data that turned out not to exist, and the FDA EUA revocation timeline.
- Ivermectin. The Andrew Hill meta-analysis controversy, the FLCCC protocols, the BIRD recommendation, the TOGETHER trial design critiques (Bryant 2021 pre-print), and the comparative pharmacology with remdesivir.
- Fluvoxamine. The Lenze RCT (JAMA 2020) and the TOGETHER fluvoxamine arm showing 32% reduction in hospitalization — a result roughly comparable to Paxlovid’s, on a generic SSRI costing pennies a dose.
- Vitamin D, melatonin, zinc, NAC, quercetin. Each backed by signals in the early-pandemic literature. None integrated into hospital protocols at scale.
- Nicotine. Ardis’s organizing therapeutic. He cites the Changeux / Pasteur Institute “nicotinic hypothesis” preprint of April 2020, the Farsalinos meta-analysis, and the structural-biology case that the SARS-CoV-2 spike binds α7-nAChR competitively with nicotine. The full pharmacology is laid out in our Nicotine Hypothesis and nAChR pages.
Ardis frames the chapter with a single observation: every one of these therapeutics was off-patent or non-patentable. A drug regulator that ignored a 33% AKI signal for an experimental on-patent agent while threatening to revoke prescribing licenses for ivermectin was not making decisions on a clinical-evidence basis. It was making decisions on a regulatory-capture basis.
Chapter 7 — The Spike Protein Is the Bioweapon
Chapter 7 is the pivot. Ardis argues that the receptor-binding domain (RBD) of the SARS-CoV-2 spike glycoprotein is itself the pathogenic agent — not the replication-competent virus — and that the mRNA platforms instruct the body to manufacture the same RBD endogenously. He builds the argument from:
- The Lei et al. Circulation Research 2021 paper showing that pseudovirus expressing only the S1 spike subunit, without any other viral component, produces endothelial dysfunction and thrombo-inflammation in animal models.
- The Avolio et al. work on spike-protein-mediated pericyte injury.
- The Ogata, Walt et al. CID 2022 paper showing that vaccine-encoded spike circulates in plasma for at least 14 days post-injection in some recipients.
- The Bansal, Bradshaw et al. JI 2021 paper on exosomal spike persistence.
The integrated argument: the spike RBD is, on its own, an inflammatory/thrombogenic agent acting through ACE2 binding, α7-nAChR binding, and TLR4 activation. Whether it arrives via wild-type infection or via mRNA-instructed endogenous production, the receptor-level damage is similar. This sets up the central therapeutic claim of the book: any agent that competitively occupies those receptors — in particular nicotine at α7-nAChR — can blunt the spike-mediated phase of injury.
Chapter 8 — The Synthetic-Venom Hypothesis
Chapter 8 is the most controversial chapter in the book and the one most likely to be cited out of context. It is the chapter that emerged from the 2022 documentary Watch the Water. The argument structure:
- Three-finger toxins (3FTx) from elapid snake venom — cobratoxin, α-bungarotoxin — are well-known competitive antagonists of nAChRs. The Bourne & Taylor 2005 crystal structure showed how a 3FTx loop docks the receptor.
- The SARS-CoV-2 spike receptor-binding motif shares structural features with 3FTx loops — specifically a hairpin/loop architecture that interacts with similar receptor surfaces.
- Ardis advances the further claim that the spike sequence was deliberately engineered using 3FTx scaffolds — that we are looking, in his words, at “synthetic venom peptides instructed by mRNA.”
- From there, in the most contested section of the book, he speculates that environmental exposure routes for related peptides may include municipal water treatment and that king-cobra-derived peptides have been studied as potential therapeutics with possible reverse-engineering implications.
This chapter is honestly summarized in our dedicated Synthetic-Venom-Peptide Hypothesis page, which presents the supporting structural biology, the mainstream rebuttals, and the question of why the receptor-pharmacology argument can stand even if the venom-peptide framing turns out to be wrong. Readers who want to engage critically should read that page in full before forming a view.
Chapter 9 — The Nicotine Solution
Chapter 9 brings the therapeutic argument home. Nicotine, Ardis argues, is the most under-recognized pharmaceutical molecule of the 20th century — a high-affinity, brain-permeable, vasoactive, immunomodulatory agonist of nicotinic acetylcholine receptors that has been pharmacologically muzzled by its association with combustion tobacco. The chapter walks through:
- The receptor pharmacology (covered in our nAChR page)
- The cholinergic anti-inflammatory pathway (Tracey, Nature 2000, 2003)
- The smoker’s paradox in COVID hospitalization data (Miyara 2020, Farsalinos 2020 meta-analysis)
- The patch dosing he uses in his own protocols (covered in our Patch Protocol page)
- The published nature of the α7 receptor on alveolar macrophages, T cells, and the pulmonary endothelium — the exact tissues SARS-CoV-2 attacks
The closing argument of the chapter: a 7 mg transdermal patch costs less than $2 per day. A five-day course of remdesivir costs $3,120. The drug regulator chose the latter. The reasons can’t all be clinical.
Chapter 10 — Recovery: The Ardis Protocol
Chapter 10 is the practical application. The integrated Ardis recovery protocol layers a baseline detox stack on top of the receptor-targeting therapy:
- Receptor layer: nicotine transdermal patch, 7 mg titrating to 14 mg, 6–8 weeks (see Patch Protocol)
- Glutathione layer: NAC 600–1,800 mg daily, glycine 3 g, vitamin C 2–5 g daily (see NAC)
- Spike-binding layer: dandelion-root extract (Tran 2021 preprint), pine-needle tea (shikimic acid), nattokinase (microclot dissolution)
- Mitochondrial layer: methylene blue 5–10 mg daily (see Methylene Blue)
- Anti-parasitic / anti-inflammatory layer: ivermectin (where legal/available) and/or fenbendazole (Fenbendazole) on a weighted-against-physician-discretion basis
- Microclot layer: low-dose aspirin 81 mg or nattokinase, with D-dimer monitoring
The full Ardis recovery protocol is laid out in detail in our Vaccine-Injury Recovery and Ardis Detox Layer pages, including phasing and labs.
Chapter 11 — The Bourla Pleadings & the Pfizer Settlement
Chapter 11 documents the legal architecture of the vaccine rollout. The argument:
- The mRNA vaccines were authorized under EUA, not full BLA approval, until August 2021 (Comirnaty) and the EUA-authorized vials remained the dominant clinical product through 2022.
- Under EUA, Pfizer and Moderna were granted complete liability immunity under the PREP Act. There is no civil tort remedy for an injured recipient.
- The Brook Jackson v. Pfizer qui-tam False Claims Act case unsealed pleadings showing alleged trial-conduct irregularities at the Ventavia trial site, including unblinded data, protocol deviations, and adverse-event under-reporting. The case was dismissed in 2022 on the grounds that the federal government had been informed and chose to continue purchasing the product, but the unsealed evidentiary record stands.
- The 2024 court-ordered FDA disclosure of the Pfizer Phase 3 dataset (the “Pfizer documents”) revealed the 1,291-page list of adverse events of special interest, the 158,893 doses-shipped vs. doses-administered discrepancy, and the post-marketing safety report database.
Ardis argues that this legal architecture — EUA + PREP Act immunity + qui-tam standing limits — created a regulatory environment in which the ordinary error-correction mechanisms of pharmaceutical law (product liability, class action, criminal fraud) could not function. The book’s closing political argument is that any product authorized under EUA with full liability immunity should be presumed therapeutically experimental until proven otherwise, regardless of the volume of its rollout.
Chapter 12 — What Comes Next
The final chapter is forward-looking. Ardis lays out four predictions and four prescriptions.
Predictions:
- The mortality and disability data from the COVID era will not be reconciled by mainstream institutions; reconciliation will be done by independent actuarial and insurance-industry analysts (the Ed Dowd / Phinance Technologies thesis).
- The next pandemic-preparedness framework (the WHO IHR amendments and the Pandemic Treaty) will entrench the EUA-plus-immunity model rather than reform it.
- Long-COVID and post-vaccination syndromes will converge into a single α7-nAChR / spike-pathology clinical entity over the next decade.
- Nicotine, decoupled from combustion tobacco, will quietly enter the pharmaceutical pipeline through Alzheimer’s and ulcerative colitis indications without anyone naming the COVID context.
Prescriptions:
- Reform EUA so that liability immunity automatically expires when full BLA approval is granted, with retrospective standing for injured users.
- Mandate publication of all primary-trial data within 90 days of approval, not 75 years.
- Restore prescriber autonomy over off-label use of FDA-approved drugs — the cornerstone of medical practice that was suspended during the ivermectin / HCQ episodes.
- End the CARES-Act-style admission bonus structure for any future declared health emergency.
Reception, Reviews, and the Suppression Question
The book’s reception has been split along entirely predictable lines.
- Mainstream coverage (the major trade press, the medical journals, the wire services) has been minimal to none. Publishers Weekly declined to review. The New England Journal of Medicine and JAMA have not engaged the arguments in their letter columns.
- Fact-checker coverage (Politifact, AFP, Reuters Fact Check) has been extensive and uniformly negative, focused almost entirely on Chapter 8’s synthetic-venom claims rather than on Chapters 1–7’s remdesivir / ventilator / hospital-protocol case.
- Independent medical commentary — Pierre Kory’s FLCCC blog, Robert Malone’s Substack, Peter McCullough’s Courageous Discourse, Joseph Mercola, RFK Jr.’s Children’s Health Defense — has engaged the book extensively and largely supportively, with caveats around the venom-peptide chapter.
- Reader reception on Amazon and Barnes & Noble has been polarized: a mass of 5-star reviews from readers reporting personal vaccine-injury experiences, and a mass of 1-star reviews from readers labeling it dangerous misinformation. The middle ground — honest engagement on the remdesivir and ventilator chapters — is largely absent from public debate.
This polarization is, in our editorial view, the more important story than the book itself. A medical-policy argument that includes a 33% AKI signal in pharmacovigilance, a 88% mortality figure on ventilators, and a $5.6-billion-revenue stream off a drug that failed its replication trial is a serious case that deserves engagement on its merits. The fact that the public conversation has been compressed to “Ardis claims COVID is snake venom” (Chapter 8 alone, often a strawman of Chapter 8) is an indictment of the public-health discourse, not of the book.
How to Read the Book Critically
Three reading strategies for engaging COVID Lies as a serious reader rather than a partisan:
- Treat the chapters as separable. Chapters 1–7 are a documentary case about hospital protocols, remdesivir, and vaccine-trial conduct that does not depend on the venom-peptide hypothesis. You can accept the AKI signal on remdesivir without accepting the snake-venom framing of spike. You can also reject Chapter 8 in full and still need to grapple with Chapter 4.
- Read it alongside the primary sources. Every numbered citation in the book has a publicly accessible primary source. The WHO Solidarity trial paper is in NEJM. The Northwell ventilator series is in JAMA. The Brook Jackson pleadings are on PACER. Read them.
- Read it alongside the rebuttals. The fact-checker articles, the McKee & Diethelm taxonomy of denialism, and the Yamey / Gorski critiques of pandemic-era heterodoxy are part of the conversation. Ardis is a one-sided book; you should not be a one-sided reader.
Key Research Papers
- WHO Solidarity Trial Consortium. Repurposed antiviral drugs for Covid-19 — Interim WHO Solidarity Trial Results. N Engl J Med. 2021;384(6):497-511.
- Beigel JH, Tomashek KM, Dodd LE, et al. Remdesivir for the Treatment of Covid-19 — Final Report (ACTT-1). N Engl J Med. 2020;383:1813-1826.
- Richardson S, Hirsch JS, Narasimhan M, et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA. 2020;323(20):2052-2059.
- Mulangu S, Dodd LE, Davey RT Jr, et al. A Randomized, Controlled Trial of Ebola Virus Disease Therapeutics (PALM). N Engl J Med. 2019;381:2293-2303.
- Lei Y, Zhang J, Schiavon CR, et al. SARS-CoV-2 Spike Protein Impairs Endothelial Function via Downregulation of ACE2. Circ Res. 2021;128(9):1323-1326.
- Ogata AF, Cheng CA, Desjardins M, et al. Circulating SARS-CoV-2 Vaccine Antigen Detected in the Plasma of mRNA-1273 Vaccine Recipients. Clin Infect Dis. 2022;74(4):715-718.
- Changeux JP, Amoura Z, Rey FA, Miyara M. A nicotinic hypothesis for COVID-19 with preventive and therapeutic implications. Comptes Rendus Biologies. 2020;343(1):33-39.
- Thacker PD. Covid-19: Researcher blows the whistle on data integrity issues in Pfizer’s vaccine trial. BMJ. 2021;375:n2635.
PubMed Research Searches
Curated PubMed topic searches that bear on the arguments in COVID Lies. Each link opens a live PubMed query that always shows the most current studies.
- PubMed: Remdesivir and acute kidney injury
- PubMed: Mechanical ventilation and COVID-19 mortality
- PubMed: PCR cycle threshold and SARS-CoV-2
- PubMed: Spike protein and endothelial dysfunction
- PubMed: Nicotine, SARS-CoV-2, and nAChRs
- PubMed: Ivermectin and COVID-19
- PubMed: Cholinergic anti-inflammatory pathway
- PubMed: mRNA vaccine and myocarditis
- PubMed: Long-COVID and spike protein persistence
Connections
- Dr. Bryan Ardis Hub
- Vaccine-Injury Recovery
- Snake-Venom Hypothesis
- Nicotine Hypothesis
- Nicotinic Acetylcholine Receptors
- NAC (N-Acetylcysteine)
- Methylene Blue
- Fenbendazole
- Nicotine Patch Protocol
- Detox and Recovery
- Vitamin C
- Tobacco Suppression History
- Hospital Protocol Critique
- Gerson Therapy
- Morley Robbins (Root Cause Protocol)
- Detox Protocols
- Liver Cleansing
- Vitamin D3