Vaccine-Injury Recovery: The Bryan Ardis Protocol for Post-Vaccination Symptoms
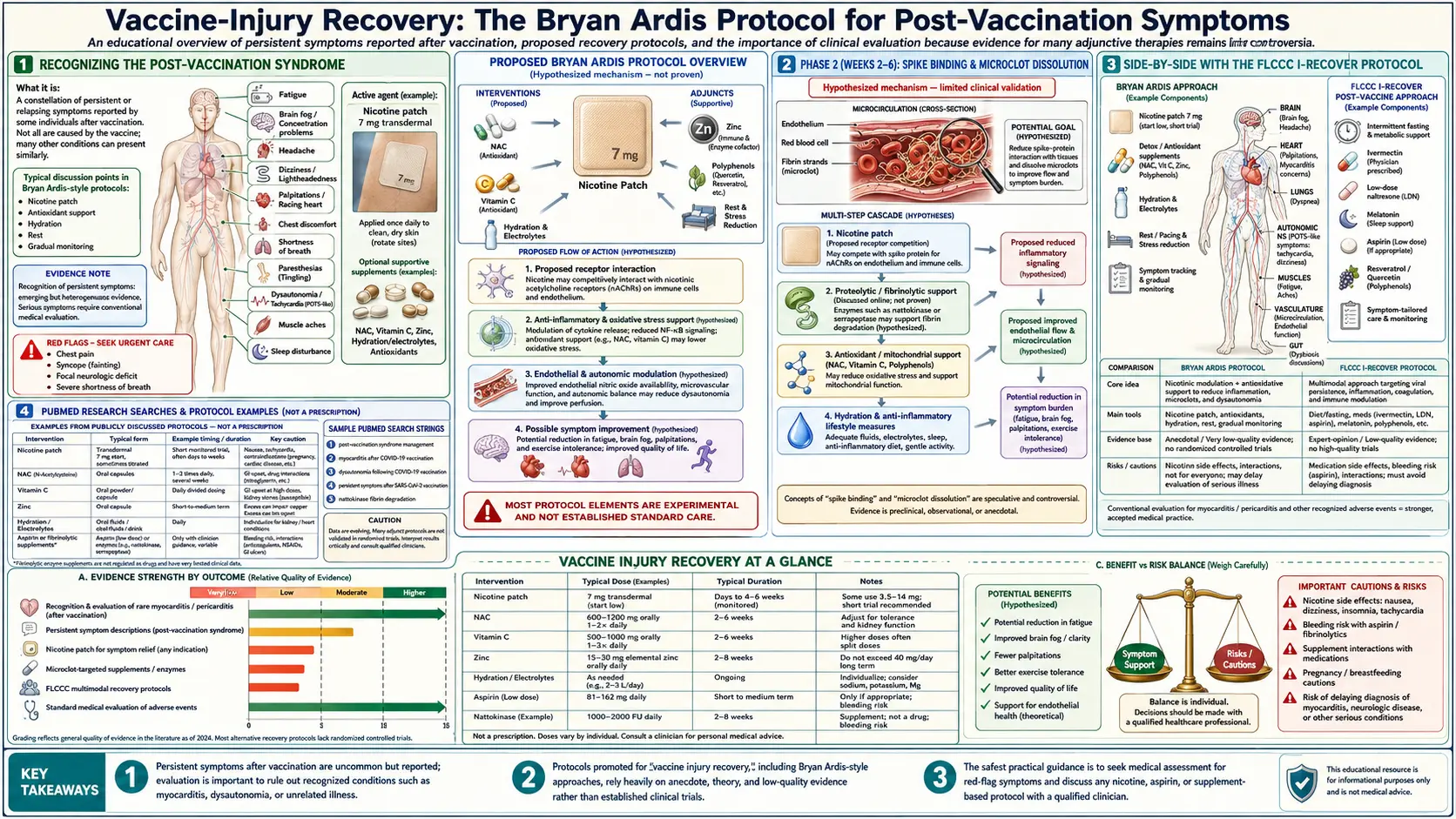
Table of Contents
- Recognizing the Post-Vaccination Syndrome
- Mechanistic Framework: Spike, Lipid Nanoparticles, Microclots
- Initial Clinical Evaluation
- Recommended Lab Panel
- Phase 1 (Days 1–14): Receptor Saturation & Glutathione
- Phase 2 (Weeks 2–6): Spike Binding & Microclot Dissolution
- Phase 3 (Weeks 6–12): Mitochondrial & Autonomic Recovery
- Phase 4 (Months 3–12): Long-Term Maintenance
- The Nicotine Patch Component
- Side-by-Side with the FLCCC I-RECOVER Protocol
- Special Case: Post-Vaccination Myocarditis
- Special Case: Neurological Symptoms (POTS, Tinnitus, Brain Fog)
- What to Expect — Realistic Trajectories
- Patient Advocacy & Compensation Resources
- Key Research Papers
- PubMed Research Searches
- Connections
- Featured Videos
1. Recognizing the Post-Vaccination Syndrome
The clinical presentation that Ardis and a growing body of independent clinicians describe as “post-vaccination syndrome” (PVS) overlaps substantially with long-COVID, ME/CFS, and dysautonomia syndromes. Common features include:
- Persistent fatigue, often with post-exertional malaise pattern
- Cognitive symptoms: brain fog, word-finding difficulty, short-term memory impairment
- Cardiovascular: palpitations, exercise intolerance, orthostatic intolerance / POTS phenotype
- Neurological: tinnitus, paresthesias, internal vibrations, autonomic dysfunction
- Reproductive: menstrual irregularities (the published Lee et al. signal in Vaccine)
- Dermatological: hives, flushing, mast-cell-activation features
- Musculoskeletal: myalgias, arthralgias, new-onset autoimmune signals
- Psychiatric: anxiety, depression, sleep disturbance — often refractory to standard treatment
The Yale LISTEN study (Krumholz et al., BMJ Public Health 2024) documented the syndrome in 241 patients and characterized its lab and symptom phenotype. The NIH has acknowledged the entity through its post-vaccination arm of the RECOVER initiative. Patients reporting these symptoms should be taken seriously, evaluated thoroughly, and given access to candidate recovery strategies — the precondition the Ardis protocol assumes.
2. Mechanistic Framework: Spike, Lipid Nanoparticles, Microclots
The Ardis recovery protocol is built on a four-mechanism model of post-vaccination injury:
- Endogenous spike production. Lipid-nanoparticle-encapsulated mRNA enters cells systemically (the LNP biodistribution is not confined to the deltoid; it includes liver, spleen, ovary, lymph node, and adrenal). Translated spike protein circulates for at least 14 days post-injection (Ogata 2022) and exosomally for longer (Bansal 2021).
- Receptor-mediated injury. Circulating spike binds ACE2, α7-nAChR, TLR4, and CD147, producing endothelial dysfunction, cytokine release, and microclot formation (Lei Circ Res 2021; Avolio 2021).
- Microclot persistence. Pretorius et al. (Cardiovasc Diabetol 2021) documented amyloid-fibrin microclots in long-COVID patients that resist normal fibrinolysis and trap inflammatory mediators — the microclot phenotype now extended to PVS in independent reports.
- Autoimmune cross-reactivity. Spike-induced antibodies cross-react with self-antigens in some patients (the “molecular mimicry” pathway documented by Vojdani et al.), producing post-vaccine autoimmune syndromes that follow rather than precede the injection.
The protocol layers attack each of these mechanisms in sequence: receptor saturation in Phase 1, spike clearance and microclot dissolution in Phase 2, mitochondrial and autonomic recovery in Phase 3, long-term maintenance in Phase 4.
3. Initial Clinical Evaluation
A patient reporting post-vaccination symptoms should be evaluated as a real medical patient with a documented exposure and a documented symptom timeline. The minimum work-up:
- Detailed timeline: dates of doses, lot numbers, type (Pfizer/Moderna/J&J/Novavax), symptom onset relative to dose
- Pre-vaccination baseline (for comparison): prior fatigue, sleep, exercise tolerance, cognitive function
- Cardiovascular evaluation: 12-lead ECG, basic echo if symptomatic, troponin if cardiac symptoms within 30 days of dose, Holter or event monitor if palpitations
- Orthostatic vitals: HR/BP supine and after 3, 5, 10 min of standing (POTS criteria: HR rise ≥30 bpm in adults, ≥40 in adolescents)
- Neurological exam if neurological symptoms present
- Symptom-severity scoring (PROMIS, FIQR for fibromyalgia overlap, COMPASS-31 for autonomic)
4. Recommended Lab Panel
The Ardis-recommended lab panel for an initial PVS work-up:
- CBC + differential
- Comprehensive metabolic panel
- D-dimer (microclot/thrombosis screening)
- Fibrinogen
- CRP and ESR
- Ferritin (inflammation marker, not iron storage in this context)
- LDH
- Troponin I or T (cardiac involvement)
- BNP or NT-proBNP if dyspneic
- Full thyroid panel: TSH, free T3, free T4, reverse T3, TPO and TG antibodies
- 25-OH vitamin D (target 50–80 ng/mL)
- Ferritin + serum iron + TIBC + transferrin saturation (for the iron-overload-vs-anemia question)
- ANA, complement (C3, C4) if autoimmune signals
- Histamine, tryptase if mast-cell signals
- Spike antibodies (anti-S, anti-N): anti-S indicates post-vaccination or post-infection humoral; anti-N indicates wild-type infection. The pattern helps distinguish PVS from long-COVID.
Specialty labs that some patients pursue: micro-clot imaging via Pretorius lab (commercially available through select clinics), exosomal spike via Resia Pretorius’s collaborators, full antiphospholipid panel.
5. Phase 1 (Days 1–14): Receptor Saturation & Glutathione
The first two weeks aim to saturate α7-nAChR (preventing further spike-mediated receptor damage) and restore glutathione (the central antioxidant pool depleted in spike-mediated oxidative stress).
- Nicotine patch: 7 mg / 24-h, applied 16 hours on / 8 off. Half-patch first 1–2 days. (See Patch Protocol for full dosing.)
- NAC: 600 mg twice daily on an empty stomach. (See NAC.)
- Glycine: 3 g at bedtime — co-precursor of glutathione, also improves sleep quality.
- Vitamin C (whole-food or buffered): 2 g three times daily. (See Vitamin C.)
- Vitamin D3: 5,000 IU daily with K2 (100–200 mcg MK-7) and adequate magnesium intake. (See Vitamin D3.)
- Magnesium glycinate or threonate: 400–600 mg evenly split through day. (See Magnesium.)
- Melatonin: 5–20 mg at bedtime. The Reiter group has documented its anti-inflammatory and mitochondrial-protective effects; high-dose melatonin is well-tolerated.
- Sleep hygiene + stress reduction: non-negotiable foundation. (See Sleep Hygiene, Stress Management.)
6. Phase 2 (Weeks 2–6): Spike Binding & Microclot Dissolution
Once the receptor and antioxidant layer is established, Phase 2 adds agents targeting circulating spike and microclot resolution:
- Continue all Phase 1 agents. Step nicotine patch up to 14 mg if tolerated and indicated.
- Dandelion-root extract: 2 cups of strong tea daily, or 500–1,000 mg standardized extract twice daily. The Tran et al. 2021 preprint reported in-vitro inhibition of spike–ACE2 binding by dandelion root.
- Pine-needle tea: traditional preparation (1 tablespoon of fresh white-pine or eastern-white-pine needles steeped in 8 oz water). Source of shikimic acid; traditional respiratory remedy.
- Nattokinase: 2,000 FU twice daily on empty stomach — fibrinolytic enzyme with documented microclot-dissolving activity (Pretorius lab work). Hold or pause if on anticoagulants without physician guidance.
- Serrapeptase: 80,000 SPU twice daily on empty stomach — complementary fibrinolytic.
- Low-dose aspirin: 81 mg daily, with food, if not contraindicated by bleeding risk or peptic disease. (See Aspirin.)
- Quercetin: 500 mg twice daily — zinc ionophore, mast-cell stabilizer.
- Zinc: 25–50 mg daily with copper 2–4 mg to maintain ratio. (See Zinc.)
7. Phase 3 (Weeks 6–12): Mitochondrial & Autonomic Recovery
Phase 3 layers in mitochondrial-recovery and autonomic-regulation agents for patients still symptomatic at 6 weeks:
- Methylene blue: 5–10 mg morning, working up to twice daily. Mitochondrial electron-bypass agent. Avoid with SSRIs/SNRIs (serotonin-syndrome risk). (See Methylene Blue.)
- CoQ10 (ubiquinol form): 200–400 mg daily.
- L-carnitine (acetyl-L-carnitine): 1,000 mg twice daily — fatty-acid oxidation support, often dramatic for fatigue.
- Creatine monohydrate: 3–5 g daily — mitochondrial energetics support. (See Creatine.)
- NAD+/NMN: NMN 250–500 mg daily, or NAD+ IV course where available. (See NAD+ and NMN.)
- Low-dose naltrexone (LDN): 1.5–4.5 mg at bedtime — immune-modulatory and central-pain-modulating in dysautonomia and ME/CFS. Requires prescription. (See Low-Dose Naltrexone.)
- Ivermectin: where legal/available, 0.2–0.4 mg/kg per FLCCC long-COVID protocol guidance, in cycles. The legal status varies by jurisdiction; this is documentation, not a recommendation to obtain it through extralegal channels.
- Vagal-tone training: slow diaphragmatic breathing, cold-face exposure, gargling, humming, progressive cardio reconditioning where tolerated. (See Breathwork.)
8. Phase 4 (Months 3–12): Long-Term Maintenance
For patients still symptomatic at 3 months, a maintenance regimen layered on continued lifestyle reconditioning:
- Continue NAC, vitamin D, magnesium, melatonin (lower doses)
- Methylene blue ongoing if tolerated and helping
- LDN ongoing
- Nattokinase or low-dose aspirin ongoing if D-dimer elevated
- Progressive aerobic reconditioning, ideally with HRV biofeedback
- Consider hyperbaric oxygen therapy (mHBOT) where accessible: 40–60 sessions at 1.5–2.0 ATA
- Re-evaluate every 3 months; many patients improve substantially by month 12
9. The Nicotine Patch Component
The nicotine patch is the receptor-saturating anchor of the protocol and the most distinctive feature compared to the FLCCC and other PVS protocols. It is most appropriate when:
- Symptoms are within 30–60 days of vaccine dose (highest circulating spike likelihood)
- Cardiac evaluation is clean (no contraindication)
- The patient is a healthy adult, non-pregnant, non-adolescent
- The patient is willing to commit to a 4–8 week course
The patch is a tool, not a panacea. It does its biggest work in Phase 1 and Phase 2; by Phase 3 the receptor-saturation work is largely done and the residual benefit is maintenance-level. The full dosing ladder, contraindications, and tapering are in our Patch Protocol page.
10. Side-by-Side with the FLCCC I-RECOVER Protocol
The Front Line COVID-19 Critical Care Alliance (FLCCC), led by Pierre Kory and Paul Marik, publishes the I-RECOVER protocol for post-vaccination injury. Major similarities and differences with the Ardis protocol:
- Both use: NAC, vitamin C, vitamin D, melatonin, low-dose aspirin, ivermectin (where legal), low-dose naltrexone, fluvoxamine option, antihistamines for mast-cell features.
- FLCCC adds: stronger emphasis on fluvoxamine (SSRI with sigma-1 receptor activity), corticosteroids in select cases, more detailed cardiac and POTS-specific arms.
- Ardis adds: the nicotine patch as a central receptor-saturation agent. FLCCC does not currently include nicotine in I-RECOVER, though Pierre Kory has discussed the receptor-pharmacology rationale on podcasts.
- Ardis emphasizes: dandelion root and pine-needle tea more strongly; methylene blue earlier.
The two protocols are largely compatible. A reasonable implementation strategy is to start with the FLCCC I-RECOVER framework and add the nicotine-patch component from the Ardis protocol if the patient is in the appropriate window and free of cardiac contraindications.
11. Special Case: Post-Vaccination Myocarditis
Post-vaccination myocarditis is a well-documented adverse event, particularly in young men after mRNA vaccines (Witberg et al., NEJM 2021; Mevorach et al., NEJM 2021). Patients with documented or suspected post-vaccination myocarditis require:
- Cardiology partnership (do not self-treat suspected myocarditis)
- Cardiac MRI for diagnosis
- Standard-of-care for myocarditis (rest, anti-inflammatory protocols)
- Caution with nicotine. Active myocarditis is a contraindication to nicotine therapy. The patch is appropriate only after cardiac recovery, and only in consultation with the treating cardiologist.
- NAC, vitamin C, melatonin, omega-3 fatty acids are reasonable supportive layers without the cardiovascular concerns of nicotine.
12. Special Case: Neurological Symptoms (POTS, Tinnitus, Brain Fog)
Neurological PVS phenotypes have specific additional considerations:
- POTS phenotype: hydration (3 L/day), 8–10 g sodium/day where blood pressure permits, compression garments, gradual cardio reconditioning per the Levine protocol, midodrine or fludrocortisone if needed. (See POTS.)
- Tinnitus: NAC, glycine, taurine, ginkgo biloba EGb 761. (See Tinnitus.)
- Brain fog / cognitive: nicotine’s α4β2 occupancy gives a small pro-cognitive bonus; methylene blue is often dramatic; lion’s mane mushroom (1–3 g daily) for BDNF.
- MCAS phenotype: H1 + H2 blockers (loratadine + famotidine), quercetin, low-histamine diet trial. (See MCAS.)
13. What to Expect — Realistic Trajectories
Recovery patterns vary widely. Honest framing for patients beginning the protocol:
- Two-week mark: Some patients report meaningful improvement (energy, brain fog clearing). Many report no change yet but tolerate the regimen well.
- Six-week mark: Most patients can identify whether the protocol is producing benefit. Non-responders should be re-evaluated for missed diagnoses (autoimmune, structural cardiac, undiagnosed thyroid).
- Three-month mark: The majority of responders are 50–80% improved. A substantial minority require Phase 3 layering.
- Twelve-month mark: Most responders are at or near pre-vaccination baseline. A persistent subset (~20%) remain disabled and require chronic management akin to ME/CFS.
Setbacks happen. The illness is real. Patience with one’s own recovery is part of the protocol, and over-exertion in Phases 1–2 is the most common reason for relapse.
14. Patient Advocacy & Compensation Resources
- VAERS (Vaccine Adverse Event Reporting System): if you have not reported your adverse event, do so. The data, while imperfect, is the only public-domain pharmacovigilance signal.
- CICP (Countermeasures Injury Compensation Program): the federal program for COVID-vaccine injury compensation, with a 1-year filing deadline from injury date. Compensation rates have been low historically but the program is the official avenue.
- React19: patient-advocacy nonprofit specifically for COVID-vaccine injuries. Resources, peer support, and clinician referrals.
- Children’s Health Defense: legal-resources clearinghouse.
- FLCCC clinician network: the FLCCC maintains a directory of physicians familiar with PVS / I-RECOVER.
- Yale LISTEN study: still enrolling at the time of writing; a way for patients to contribute their data to formal research.
Key Research Papers
- Ogata AF, Cheng CA, Desjardins M, et al. Circulating SARS-CoV-2 Vaccine Antigen Detected in the Plasma of mRNA-1273 Vaccine Recipients. Clin Infect Dis. 2022;74(4):715-718.
- Lei Y, Zhang J, Schiavon CR, et al. SARS-CoV-2 Spike Protein Impairs Endothelial Function via Downregulation of ACE2. Circ Res. 2021;128(9):1323-1326.
- Pretorius E, Vlok M, Venter C, et al. Persistent clotting protein pathology in Long COVID/PASC is accompanied by increased levels of antiplasmin. Cardiovasc Diabetol. 2021;20(1):172.
- Mevorach D, Anis E, Cedar N, et al. Myocarditis after BNT162b2 mRNA Vaccine against Covid-19 in Israel. N Engl J Med. 2021;385(23):2140-2149.
- Witberg G, Barda N, Hoss S, et al. Myocarditis after Covid-19 Vaccination in a Large Health Care Organization. N Engl J Med. 2021;385(23):2132-2139.
- Krumholz HM, Wu Y, Sawano M, et al. Post-Vaccination Syndrome: A Descriptive Analysis of Reported Symptoms and Patient Experiences After Covid-19 Immunization. BMJ Public Health. 2024.
- Couzin-Frankel J. Long Covid clues emerge from worldwide research effort. Science. 2022.
PubMed Research Searches
- PubMed: Post-vaccination syndrome and long-COVID
- PubMed: Spike protein and microclot fibrin
- PubMed: mRNA vaccine and myocarditis
- PubMed: NAC and spike protein
- PubMed: Nattokinase and fibrinolysis
- PubMed: Low-dose naltrexone and long-COVID
- PubMed: POTS and post-vaccination
- PubMed: Ivermectin and long-COVID
- PubMed: Hyperbaric oxygen and long-COVID
Connections
- NAC (N-Acetylcysteine)
- Methylene Blue
- Vitamin C
- POTS
- Zinc
- Vitamin D3
- Magnesium
- MCAS
- Nicotine Patch Protocol
- Low-Dose Naltrexone
- Dr. Bryan Ardis Hub
- Hospital Protocol Critique
- Snake-Venom Hypothesis
- Nicotinic Acetylcholine Receptors
- COVID Lies Book
- Detox and Recovery
- Post-Viral Triggers (CFS/ME)
- Myocarditis