Vitamin B3 (Niacin) in the Gerson Therapy
Vitamin B3 (niacin, also called nicotinic acid) is one of the foundational supplements in the Gerson Therapy. Within the protocol it is given alongside the strict organic plant-based diet, intensive juicing program, potassium compound, Lugol’s iodine, thyroid extract, B12, pancreatic enzymes, and CoFactor10 to treat cancer and other chronic degenerative diseases. Gerson’s framing was that niacin restores peripheral circulation, drives oxygen and nutrient delivery into hypoxic tissues, supports fatty-acid metabolism, and supplies the precursor nicotinamide for the NAD+/NADP+ coenzyme system that powers Phase I oxidative detoxification, the mitochondrial electron transport chain, and DNA repair via the PARP enzymes.
This page documents how niacin is dosed in the Gerson protocol, the biochemistry behind Gerson’s rationale, the contemporary research literature on niacin in cancer biology, lipid metabolism, neurodegeneration, and DNA repair, and the safety considerations that accompany pharmacologic dosing. It is written for patients and curious readers, not as medical advice; high-dose niacin is a pharmacologic intervention and the Gerson schedule should be followed only under qualified medical supervision.
Table of Contents
- What Is Niacin (Vitamin B3)?
- The Gerson Niacin Dose and Schedule
- The Niacin Flush — What It Is and Why Gerson Welcomed It
- Gerson’s Rationale: Circulation, Oxygen, and Metabolism
- NAD+, Sirtuins, and DNA Repair — The Modern Mechanistic View
- Niacin in Cancer Biology — What the Research Shows
- Niacin and Lipid Metabolism
- Niacin in Neurology and Psychiatry — Hoffer, Pellagra, and Schizophrenia
- Forms of B3: Nicotinic Acid vs. Nicotinamide vs. NR vs. NMN vs. “No-Flush”
- Safety, Contraindications, and Drug Interactions
- Monitoring on the Gerson Niacin Schedule
- Dietary Niacin in the Gerson Diet
- Key Research Papers
- PubMed Topic Searches
- Connections
- Featured Videos
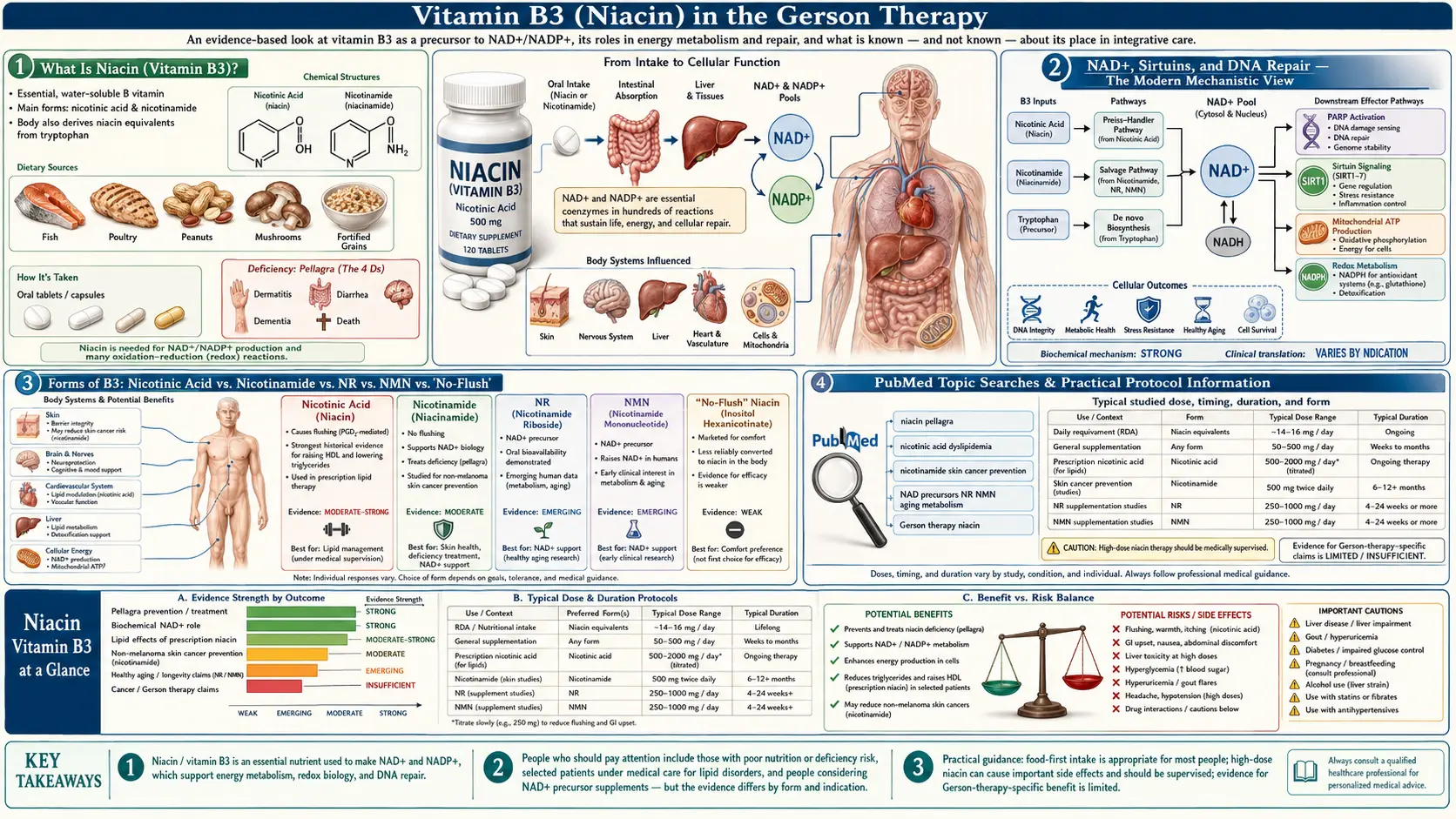
What Is Niacin (Vitamin B3)?
Vitamin B3 is the umbrella term for several closely related compounds that the body converts into the same active coenzymes:
- Nicotinic acid (niacin proper) — the form Gerson specifies. Causes the prostaglandin-mediated “flush.” Lowers LDL cholesterol and triglycerides, raises HDL.
- Nicotinamide (niacinamide) — the amide form. Does not cause flushing and does not affect blood lipids, but supplies the same NAD+ precursor.
- Nicotinamide riboside (NR) and nicotinamide mononucleotide (NMN) — newer NAD+ precursors popular in longevity research; not part of the historical Gerson protocol.
- Inositol hexanicotinate (“no-flush niacin”) — explicitly not used in Gerson because the lack of flush correlates with markedly reduced therapeutic effect on lipids and circulation.
All forms ultimately feed into the synthesis of nicotinamide adenine dinucleotide (NAD+) and its phosphorylated form NADP+. These coenzymes are central to over 400 enzymatic reactions in human metabolism, including glycolysis, the citric-acid cycle, the electron transport chain, beta-oxidation of fatty acids, the cytochrome P450 detoxification system, and DNA-damage signaling through the PARP and sirtuin enzyme families. The U.S. RDA is 16 mg/day for adult men and 14 mg/day for women; the tolerable upper intake level (UL) for nicotinic acid is 35 mg/day in healthy adults — a threshold the Gerson protocol intentionally exceeds.
The Gerson Niacin Dose and Schedule
The classic Gerson cancer protocol calls for 50 mg of plain (immediate-release) nicotinic acid taken with each of 5 to 6 juices per day, totaling 250–300 mg of niacin daily. The dose is taken with a juice (not on an empty stomach) to slow absorption slightly and reduce the intensity of the flush. The schedule typically runs for the full 18–24 month duration of the cancer protocol, with periodic pauses if liver enzymes rise or if a menstruating patient experiences unusually heavy bleeding.
Two practical rules of the Gerson niacin schedule:
- Plain crystalline nicotinic acid only. Slow-release (sustained-release) niacin is explicitly forbidden because it is the form most strongly associated with hepatotoxicity. Inositol hexanicotinate (“flush-free”) is also rejected because its therapeutic effect is unreliable.
- Niacin is paused during menstruation in female patients, because the vasodilatory effect can intensify menstrual flow. The Gerson Institute typically resumes dosing 24–48 hours after the period ends.
For non-cancer wellness applications of the modified Gerson, the niacin dose is often reduced to 50 mg one to three times per day, primarily as a circulatory and lipid-modifying intervention rather than as part of the full oncology protocol.
The Niacin Flush — What It Is and Why Gerson Welcomed It
Within 15–30 minutes of taking 50 mg of immediate-release nicotinic acid, most patients experience a characteristic warm pink-to-red flush over the face, neck, chest, and sometimes the arms, often accompanied by tingling, mild itching, and a prickling sensation. The flush typically peaks at 30 minutes and resolves over 30–60 minutes. Most patients tolerate the dose better as the schedule continues; tachyphylaxis (tolerance) develops within days to weeks and the flush diminishes substantially with regular dosing.
Mechanistically, the flush is driven by activation of the GPR109A (HCA2) receptor on epidermal Langerhans cells and macrophages, which triggers cyclooxygenase-dependent release of prostaglandins D2 and E2. These prostaglandins act on dermal vasculature to cause cutaneous vasodilation. The mechanism was definitively characterized by Benyo and colleagues in 2005 (PMID: 16167070) and is independent of the lipid-lowering and NAD+-precursor effects of niacin.
Gerson treated the flush as a desirable signal: visible evidence that peripheral circulation was being driven into the small vessels of the skin and, by extension, into hypoxic tumor tissue. Modern interpretation is more guarded — the flush is real and the vasodilation is real, but whether peripheral skin vasodilation translates into improved oxygenation of deep solid tumors is not established. Gerson’s instinct that the flush was useful is partly vindicated by the GPR109A literature: the same receptor is expressed on adipocytes, immune cells, and colonic epithelium, and its activation has documented anti-inflammatory and immunomodulatory effects (Graff et al., 2014, PMID: 24336100).
Gerson’s Rationale: Circulation, Oxygen, and Metabolism
Max Gerson’s working theory of chronic disease, set out most fully in A Cancer Therapy: Results of Fifty Cases (1958), held that degenerative illness arises when cellular metabolism shifts from aerobic respiration to fermentation — an idea he drew directly from Otto Warburg’s 1924–1931 work on the “Warburg effect” in tumor cells (Warburg, 1956, PMID: 13298683). In Gerson’s framework, restoring aerobic respiration required three converging interventions: (1) flooding cells with potassium and depleting sodium to restore the membrane potential needed for mitochondrial function; (2) supplying iodine and thyroid extract to drive metabolic rate; and (3) maximizing oxygen delivery to tissues. Niacin’s circulatory and metabolic roles fit cleanly into the third pillar.
Three of Gerson’s specific claims for niacin map onto modern biochemistry as follows:
- Improved capillary perfusion. The cutaneous flush is a direct demonstration of arteriolar and capillary vasodilation. Gerson assumed the same mechanism increased perfusion of liver, kidney, and tumor parenchyma. Direct measurements in deep tissue are limited, but cerebral blood flow studies in healthy volunteers do show measurable increases after immediate-release niacin (Saareks et al., 1999, PMID: 10417631).
- Support for fatty-acid metabolism. Beta-oxidation of fatty acids in the mitochondrial matrix is NAD+-dependent at multiple steps; replenishing the NAD+ pool with niacin sustains mitochondrial fuel oxidation. Gerson did not have the molecular-biology language for this in 1958, but his clinical instinct that niacin helped patients metabolize the small amount of flax oil he eventually added to the protocol is consistent with what is now known.
- Phase I detoxification co-factor. The cytochrome P450 enzymes of the liver, which perform the bulk of Phase I biotransformation of drugs, hormones, and environmental toxins, all use NADPH as a reducing co-factor. Niacin supports the regeneration of this pool. Gerson framed this as “activating the liver’s detoxification capacity,” which is a reasonable plain-language description of NADPH-dependent monooxygenase activity.
NAD+, Sirtuins, and DNA Repair — The Modern Mechanistic View
The most active modern research on niacin centers on the role of NAD+ in cellular aging, DNA repair, and cancer biology. Three findings of the past two decades are directly relevant to the Gerson rationale:
- NAD+ declines with age. Tissue NAD+ levels fall progressively from young adulthood through old age in human skin, brain, liver, and skeletal muscle (Massudi et al., 2012, PMID: 22874941). Restoring NAD+ with B3 precursors reverses several markers of mitochondrial dysfunction in aged tissue.
- PARP-1 is the largest single consumer of NAD+. Poly(ADP-ribose) polymerase 1 is activated by DNA strand breaks and consumes NAD+ to mark damaged sites for repair. Chronic genomic stress — from radiation, chemicals, oxidative damage, or tumor biology — depletes the cellular NAD+ pool and impairs both DNA repair and mitochondrial function (Bai & Cantó, 2012, PMID: 22682218).
- Sirtuins require NAD+. The seven mammalian sirtuin enzymes (SIRT1–SIRT7) are NAD+-dependent deacetylases that regulate gluconeogenesis, mitochondrial biogenesis, anti-inflammatory gene expression, and the DNA-damage response. NAD+ depletion silences sirtuin activity (Imai & Guarente, 2014, PMID: 24786309).
From this perspective the Gerson niacin schedule of 250–300 mg/day looks less like a circulatory intervention and more like a sustained NAD+-loading strategy that should support mitochondrial function, sirtuin activity, and PARP-mediated DNA repair throughout the multi-month treatment. None of this proves Gerson’s overall cancer claims, but it does locate niacin within an active and well-funded area of current biology rather than the fringe.
Niacin in Cancer Biology — What the Research Shows
Niacin and its amide nicotinamide have been studied in cancer biology since the 1980s. The literature does not show that niacin cures cancer, and Gerson’s “Fifty Cases” case series remains uncorroborated by controlled trials. What the literature does show is more limited but real:
- Pellagra-cancer link. Tissue niacin status is depressed in many cancer patients, and severe niacin deficiency (pellagra) has long been associated with elevated rates of esophageal and other epithelial cancers in populations subsisting on corn-based diets (Jacobson, 1993, PMID: 8409076).
- Radiation sensitization. Nicotinamide given alongside radiotherapy improves tumor oxygenation and radiosensitivity in animal and Phase II human studies, particularly for head-and-neck and bladder cancers (Hoskin et al., 2010, PMID: 20697091). The mechanism is partly hemodynamic (the same flush-related vasodilation) and partly metabolic.
- Skin-cancer chemoprevention. A 2015 randomized controlled trial (Chen et al., New England Journal of Medicine) showed that 500 mg of nicotinamide twice daily reduced the rate of new non-melanoma skin cancers in high-risk patients by 23% over 12 months (PMID: 26488693). This is one of the cleanest positive randomized trials for a B vitamin in any cancer indication.
- Tumor NAD+ biology. Many tumors upregulate the NAD+-salvage enzyme NAMPT and are sensitive to NAMPT inhibitors. This means tumor NAD+ dependence is a real therapeutic target, though the implication for niacin supplementation is double-edged: more NAD+ can support either healthy mitochondria or tumor metabolism depending on context (Chiarugi et al., 2012, PMID: 22576659).
What this does not prove. None of the above validates the Gerson cancer claim. The skin-cancer trial used nicotinamide (no flush) at higher dose than Gerson’s nicotinic acid schedule. Radiation-sensitization studies are adjuncts to conventional radiotherapy, not standalone treatments. The honest summary is that niacin has biologically plausible and partially research-supported roles in cancer biology, particularly as an adjunct, but the Gerson protocol as a whole does not have controlled-trial support — see the Research and Evidence page for the full picture.
Niacin and Lipid Metabolism
Outside the Gerson context, immediate-release nicotinic acid at 1–3 g/day was the first lipid-modifying drug shown to reduce cardiovascular events. The Coronary Drug Project (1975) demonstrated that 3 g/day of niacin reduced nonfatal myocardial infarction in survivors of a first heart attack, and a follow-up paper at 15 years showed an 11% reduction in all-cause mortality (Canner et al., 1986, PMID: 3782631). Niacin lowers LDL by 10–25%, lowers triglycerides by 20–50%, lowers Lp(a) by 20–30%, and raises HDL by 15–35% — effects no other single agent matches.
Two large more recent statin-era trials — AIM-HIGH (2011, PMID: 22085343) and HPS2-THRIVE (2014, PMID: 25014686) — failed to show that adding extended-release niacin to a statin further reduced events, and HPS2-THRIVE showed an excess of side effects. Mainstream cardiology no longer routinely uses niacin for lipid modification on top of statins, although the older monotherapy data remain respected.
The Gerson 250–300 mg/day dose is well below the 1–3 g/day cardiology range. Patients on the protocol can still expect modest LDL and triglyceride reductions and modest HDL increases — consistent with the protocol’s broader cardiometabolic benefits driven by the diet itself.
Niacin in Neurology and Psychiatry — Hoffer, Pellagra, and Schizophrenia
Severe niacin deficiency causes pellagra, classically described by the four D’s: dermatitis, diarrhea, dementia, and (untreated) death. The dementia of pellagra documented an unambiguous link between niacin status and brain function long before NAD+ biology was understood. The Canadian psychiatrist Abram Hoffer extended this observation in the 1950s and 1960s to argue that some forms of schizophrenia were responsive to high-dose niacin (1–3 g/day), a thesis later contested but never fully resolved (Hoffer & Osmond, 1966, PMID: 5333085).
Modern interest in niacin for the brain centers on three threads: NAD+ as a substrate for neuronal SIRT1 and PARP1; nicotinamide as neuroprotective in models of Parkinson’s and Alzheimer’s disease (Liu et al., 2013, PMID: 23438705); and nicotinamide riboside trials in mild cognitive impairment. The Gerson protocol predates all of this, but its niacin schedule remains pharmacologically consistent with the modern NAD+-restoration hypothesis.
Forms of B3: Nicotinic Acid vs. Nicotinamide vs. NR vs. NMN vs. “No-Flush”
- Nicotinic acid (Gerson form) — flushes; lowers LDL/triglycerides; activates GPR109A; raises uric acid (caution in gout).
- Nicotinamide — no flush; equivalent NAD+ precursor; no lipid effect; preferred for skin-cancer chemoprevention; can cause hepatotoxicity at very high doses (> 3 g/day).
- Inositol hexanicotinate (“no-flush niacin”) — minimal flush; minimal lipid effect; not used in Gerson because effect is unreliable.
- Nicotinamide riboside (NR) and nicotinamide mononucleotide (NMN) — newer, more direct NAD+ precursors with growing trial data in metabolic disease and aging; not part of the historical protocol but sometimes used by modified-Gerson practitioners.
- Slow-release / sustained-release niacin — explicitly avoided in Gerson because it is the form most strongly associated with cholestatic and hepatocellular liver injury.
Safety, Contraindications, and Drug Interactions
High-dose niacin is a pharmacologic intervention with a non-trivial side-effect profile.
- Hepatotoxicity. The single most important risk. Plain immediate-release nicotinic acid at the Gerson 250–300 mg/day dose is at the lower end of the hepatotoxicity range, but liver enzymes (AST, ALT, alkaline phosphatase, total bilirubin) should still be monitored. Sustained-release formulations carry a much higher risk and are forbidden in Gerson for this reason.
- Active liver disease, cirrhosis, hepatitis — absolute contraindications.
- Active peptic ulcer disease — relative contraindication; niacin can stimulate gastric acid secretion.
- Gout / hyperuricemia — relative contraindication; niacin raises serum uric acid.
- Type 2 diabetes / insulin resistance — niacin raises fasting glucose and HbA1c modestly; monitor glucose, may need to adjust antidiabetic medication.
- Pregnancy — doses above the RDA are not established safe; the full Gerson niacin schedule is not used in pregnancy.
- Drug interactions:
- Statins + high-dose niacin = increased risk of myopathy and rhabdomyolysis.
- Anticoagulants (warfarin, DOACs) + niacin = additive bleeding risk via platelet effects.
- Antihypertensives + niacin = additive hypotensive effect from vasodilation, especially during the flush.
- Allopurinol or febuxostat for gout = niacin opposes their action.
- Levodopa = niacin may modify dopaminergic balance in Parkinson’s disease.
- Pre-medication with aspirin (325 mg taken 30 minutes before the niacin dose) blunts the flush by inhibiting cyclooxygenase. The Gerson Institute generally does not recommend aspirin pre-medication because aspirin antagonizes other elements of the protocol and the flush is considered therapeutically useful. Standard cardiology practice does the opposite.
Monitoring on the Gerson Niacin Schedule
Patients on the full Gerson cancer protocol should have, at minimum:
- Comprehensive metabolic panel including AST, ALT, alkaline phosphatase, and total bilirubin at baseline, at 4 weeks, at 12 weeks, and every 3 months thereafter.
- Fasting glucose and HbA1c at baseline and every 3 months.
- Uric acid at baseline and at 6–12 weeks, especially in patients with any history of gout.
- Lipid panel at baseline and at 12 weeks — useful as a marker of overall protocol response.
- Clinical re-evaluation if the patient develops unexplained nausea, right-upper-quadrant pain, jaundice, dark urine, or pruritus; these can signal hepatic injury and warrant immediate cessation pending labs.
Dietary Niacin in the Gerson Diet
Beyond the supplement, the Gerson diet itself supplies meaningful niacin. Carrots (one of the diet’s staples), apples, leafy greens, and the “Hippocrates soup” together provide several milligrams per day, and the body synthesizes additional niacin from the amino acid tryptophan at a 60-to-1 conversion ratio. The supplemental 250–300 mg dwarfs this dietary contribution but the dietary background matters in the early induction phase before the patient is fully tolerating the supplement schedule.
Key Research Papers
- Benyo Z et al. (2005). “GPR109A (PUMA-G/HM74A) mediates nicotinic acid-induced flushing.” J Clin Invest. PMID: 16167070 — defines the receptor mechanism of the flush.
- Chen AC et al. (2015). “A Phase 3 randomized trial of nicotinamide for skin-cancer chemoprevention.” N Engl J Med. PMID: 26488693 — the cleanest positive RCT for B3 in cancer.
- Hoskin PJ et al. (2010). “Carbogen and nicotinamide in locally advanced bladder cancer: long-term results.” Lancet Oncol. PMID: 20697091 — nicotinamide as a radiosensitizer.
- Canner PL et al. (1986). “Fifteen-year mortality in Coronary Drug Project patients: long-term benefit with niacin.” J Am Coll Cardiol. PMID: 3782631 — the seminal CV-mortality benefit study.
- HPS2-THRIVE Collaborative Group (2014). “Effects of extended-release niacin with laropiprant in high-risk patients.” N Engl J Med. PMID: 25014686 — the negative statin-era trial.
- AIM-HIGH Investigators (2011). “Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy.” N Engl J Med. PMID: 22085343
- Massudi H et al. (2012). “Age-associated changes in oxidative stress and NAD+ metabolism in human tissue.” PLoS ONE. PMID: 22874941
- Imai S, Guarente L (2014). “NAD+ and sirtuins in aging and disease.” Trends Cell Biol. PMID: 24786309
- Bai P, Cantó C (2012). “The role of PARP-1 and PARP-2 enzymes in metabolic regulation and disease.” Cell Metab. PMID: 22682218
- Chiarugi A et al. (2012). “The NAD metabolome — a key determinant of cancer cell biology.” Nat Rev Cancer. PMID: 22576659
- Jacobson EL (1993). “Niacin deficiency and cancer in women.” J Am Coll Nutr. PMID: 8409076
- Saareks V et al. (1999). “Nicotinic acid and pyridoxine modulate arachidonic acid metabolism.” Pharmacol Toxicol. PMID: 10417631
- Hoffer A, Osmond H (1966). “Treatment of schizophrenia with nicotinic acid: a ten year follow-up.” Acta Psychiatr Scand. PMID: 5333085
- Liu D et al. (2013). “Nicotinamide forestalls pathology and cognitive decline in Alzheimer mice.” J Neurosci. PMID: 23438705
- Warburg O (1956). “On the origin of cancer cells.” Science. PMID: 13298683 — the metabolic-theory paper Gerson built upon.
- Graff EC et al. (2014). “Anti-inflammatory effects of the hydroxycarboxylic acid receptor 2.” Metabolism. PMID: 24336100
- NCI PDQ — Gerson Therapy (Patient Version). National Cancer Institute. cancer.gov — the NCI’s formal review of the Gerson protocol cited in the request.
- NIH Office of Dietary Supplements — Niacin Fact Sheet for Health Professionals. ods.od.nih.gov
PubMed Topic Searches
- niacin nicotinic acid cancer
- nicotinamide chemoprevention skin cancer
- NAD+ aging sirtuin
- PARP NAD DNA repair
- niacin flush GPR109A
- niacin lipid cardiovascular outcomes
- Gerson therapy
- niacin hepatotoxicity
- nicotinamide riboside clinical trial
- Warburg effect tumor metabolism
Connections
- Research Evidence
- Detoxification
- Gerson Therapy
- Supplements
- Diet Protocol
- Cancer Treatment
- Vitamin B3
- Vitamin B12
- Pellagra and Niacin Deficiency
- Cancer
- Schizophrenia
- Potassium
- Tryptophan
- Dementia
- Gout
- Practical Guide